
Abstract
Introduction
T
The lineage clonal complex 17 (CC17) contains several sequence types (STs), such as ST17, ST18, ST78, and ST117.2,17,38 Through sequential acquisition of hospital-clade-specific genes, including resistance genes and putative virulence genes, CC17 gains a selective advantage and is well adapted to the hospital environment, which emerges as the high-risk clone responsible for the worldwide spread of VRE.10,20,27,41 Recently, CC17 has been divided into three lineages (lineage 17, 18, and 78) that are significantly associated with hospital isolates. 44
Several genes have been identified as putative virulence factors that may enable enterococcal strains to survive in the hospital environment, colonize patients, and cause various infections.16,32 They include: (i) the esp gene (
In China, the Enterococci exhibited low resistance rate to vancomycin, and only 4.9% of clinical enterococcal isolates were identified as VRE in 2010. 48 However, a number of VRE strains have been isolated, involving several vancomycin-resistant Enterococcus faecium (VREfm) nosocomial outbreaks in hospitals across the country.3,11,18,25,29,30,36,45,49,50 Among these VREfm isolates, ST78 (member of CC17) was the dominant clone that possessed vanA operon and exhibited resistance to vancomycin and teicoplanin. The prevalence of the esp gene ranged from 76% to 88.9%, while 21.3% to 58% of VREfm carried the hyl gene.18,25,30,36 In this study, we reported the prevalence of VREfm isolates in our hospital, which involved 96 patients and mainly covered three ICUs. The molecular and epidemiological features of the VREfm isolates were analyzed, and the prevalence of virulent factors, including esp, hyl, acm, scm, ecbA, sgrA, pilA, and pilB, were also determined.
Materials and Methods
Bacterial strains
All clinical strains were isolated from clinical samples in a 4,000-bed tertiary care hospital. All clinical isolates were identified by VITEK 2 GP ID cards (bioMérieux, Inc.) and VITEK® MS (bioMérieux SA). Staphylococcus aureus ATCC 25923 and E. faecalis ATCC 29212 were used as the quality control strains for antimicrobial susceptibility testing. Salmonella ser. Braenderup strain (H9812) was used as a reference standard of pulsed-field gel electrophoresis (PFGE).
Antimicrobial susceptibility testing
The minimum inhibitory concentrations (MICs) of vancomycin, teicoplanin, and linezolid were measured by the E-test method (AB bioMérieux). The MICs of ampicillin, ciprofloxacin, levofloxacin, moxifloxacin, erythromycin, clindamycin, tigecycline, and nitrofurantoin were measured by the VITEK 2 AST-GP67 test Kit (bioMérieux, Inc.). All protocols were performed according to the manufacturer's instructions. All susceptibility results were interpreted according to the 2014 CLSI performance standards. 5
PFGE and plasmid analysis
An improved PFGE procedure was used for the subtyping of clinical VRE isolates. 39 To improve the typing procedure, all clinical isolates were cultured in 1.5 ml Brain–Heart infusion with 80 μl bovine serum (5%) overnight at 37°C. After centrifugation, the pellet of each isolate was collected and used for plug preparation. DNA fingerprints were obtained from PFGE profiles of genomic DNA digested with SmaI (New England Biolabs). The PFGE patterns were analyzed by BioNumerics software (Applied Maths NV) using the dice similarity coefficient. Strains were considered as the same clone (type) if they possessed ≥95% genetic similarity or <4 fragment differences of PFGE profiles. 37 S1-PFGE was performed to identify the number and size of plasmids carried in VRE isolates.
Detection of van alphabet and virulence genes
Six types of glycopeptide resistance genes (vanA, vanB, vanC, vanD, vanE, and vanG) and ddl gene (encoding a
Multilocus sequence typing
Multilocus sequence typing (MLST) was carried out for all PFGE types of E. faecium isolates by amplifying and sequencing of seven housekeeping genes according to protocols provided on the MLST website for E. faecium (http://efaecium.mlst.net/).
Statistical analysis
Fisher's exact tests were used in the Chinese High Intellectualized Statistical Software version 2010 to determine the significance of the prevalence values. p < 0.05 was considered to be statistically significant.
Results
Isolation of VREfm strains
A total of 96 nonduplicated VREfm strains were isolated from August 2008 to May 2013 (Fig. 1). Among all isolates, 60 (62.5%) were isolated from urine samples, while 12, 10, and 7 strains were isolated from drainage fluid, blood, and catheter, respectively. The median age of the patients was 74 years, and the male-to-female ratio was 1.13 (51 to 45). 73.9% (71/96) of the patients stayed in the three ICUs.
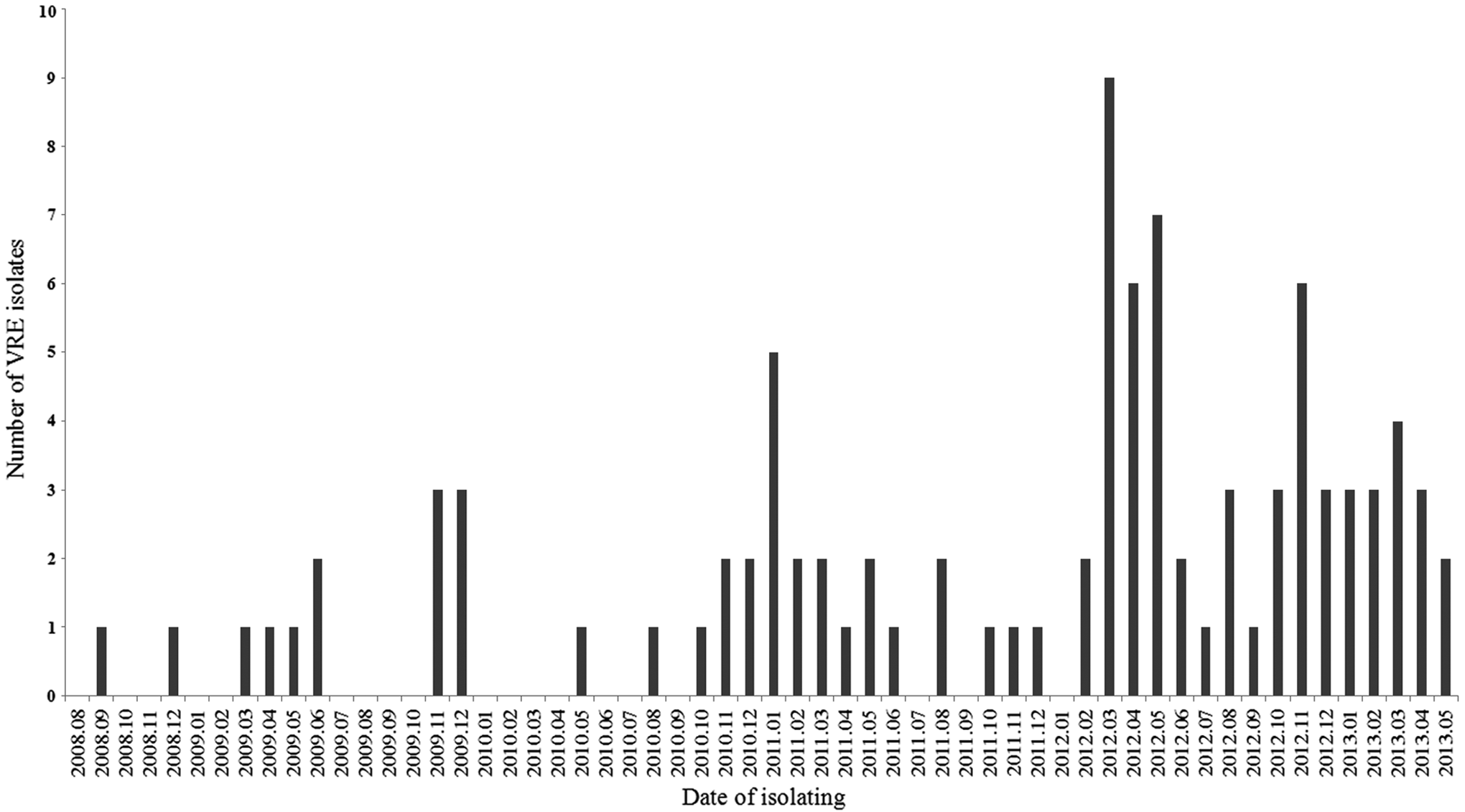
The distribution of the vancomycin-resistant Enterococcus faecium (VREfm) isolates.
PFGE and MLST analysis
The 96 VREfm isolates were categorized into 38 PFGE types (Fig. 2). Only 8 PFGE types contained 3 or more isolates, while 13 and 17 PFGE types contained 2 and 1 clinical VREfm isolates, respectively (Table 1). The PFGE type 31 strain exhibited significant clonal spread in neurology ICU, so did the PFGE type 22 in respiratory ICU, and the PFGE type 2, PFGE type 19, and PFGE type 36 stains in surgery ICU. Four STs were identified among VREfm isolates in this study. The majority of strains belonged to ST78, while only three PFGE type of strains (type 2, 26, and 35) were categorized with ST17. PFGE type 9 and 10 were identified as ST341 and ST342, respectively (Table 1).
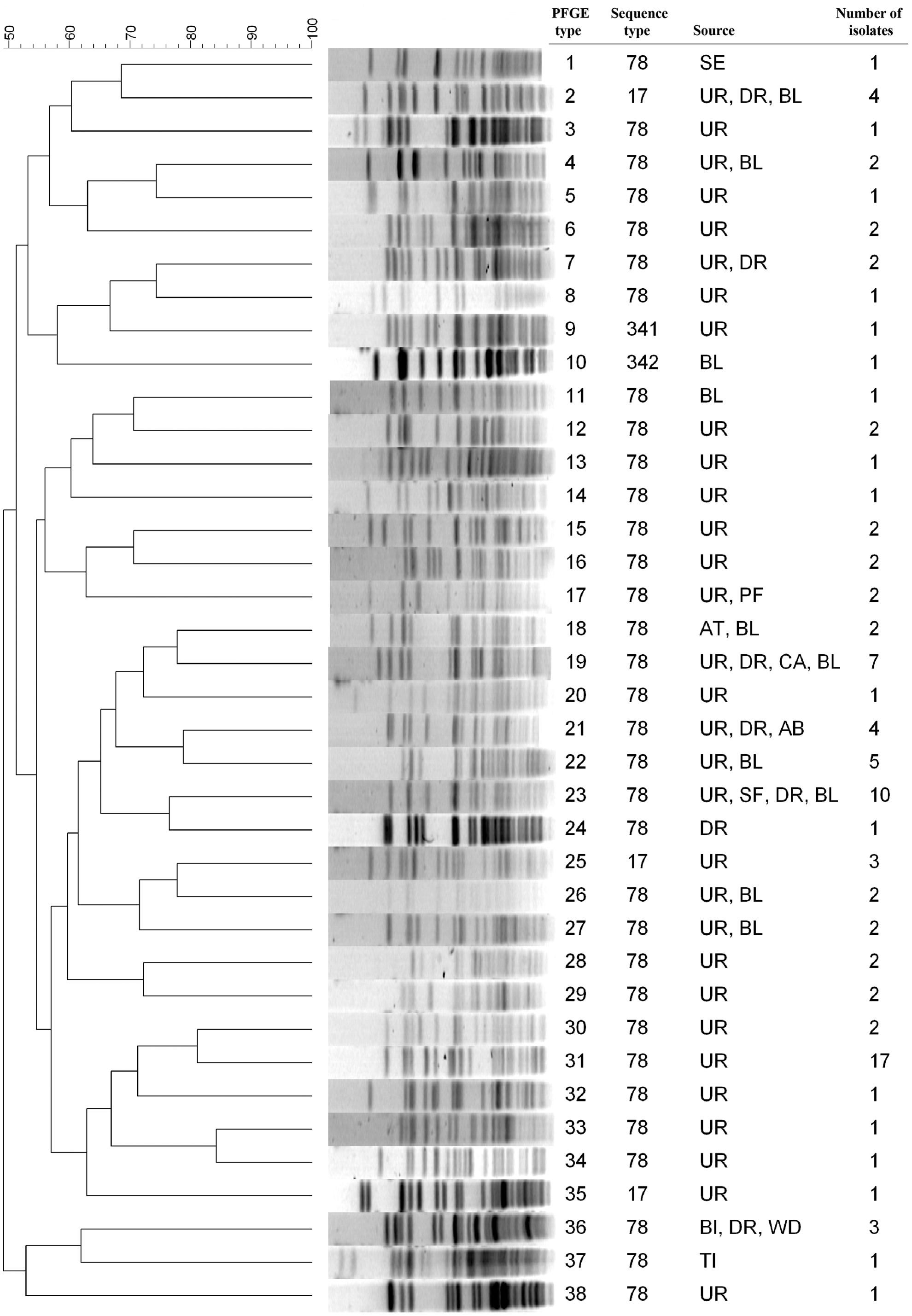
The pulsed-field gel electrophoresis dendrogram of VREfm strains. BL, blood; UR, urine; SE, secretion; DR, drainage; AB, abscess; BI, bile; WD, wound; TI, tissue; CA, catheter; PF, pleural fluid.
PFGE, pulsed-field gel electrophoresis; BL, blood; UR, urine; SE, secretion; DR, drainage; AB, abscess; BI, bile; WD, wound; TI, tissue; CA, catheter; PF, pleural fluid; VAN, vancomycin; LNZ, linezolid; TEC, teicoplanin; NIT, nitrofurantoin; TGC, tigecycline; ST, sequence type; MIC, minimal inhibitory concentration.
Antimicrobial susceptibilities
All VREfm strains were resistant to ampicillin, ciprofloxacin, levofloxacin, moxifloxacin, erythromycin, and clindamycin. The MICs of vancomycin, teicoplanin, linezolid, nitrofurantoin, and tigecycline are shown in Table 1.
Plasmid analysis
S1-PFGE analysis showed that all clinical VREfm strains carried plasmids of different sizes. Some strains (PFGE type 3 and 32) carried four plasmids, whereas some strains did not contain any plasmid (PFGE type 14, 20, 28, 37, and 38).
Prevalence of van alphabet and virulent genes
All clinical VREfm strains harbored the vanA gene and were negative for vanB, vanC, vanD, vanE, and vanG. Table 1 displays the prevalence of common virulence determinants among each strain.
Discussion
From August 2008 to May 2013, 96 nonduplicated VREfm strains were isolated. During this period, 1,605 nonduplicated E. faecium strains were isolated from various clinical specimens in our hospital. In general, VREfm was presented at a low prevalence (5.9% [96/1,605]). However, a significant increase in the prevalence of VREfm was observed in this study (February 2012 to May 2013) (Fig. 1), where 9.5% (58/612) of E. faecium isolates were VREfm (p = 0.0038). VREfm isolates have been sporadically reported across China,3,18,24,25,29,30,36,49 and two outbreaks of VREfm (involving 14 and 32 patients, respectively) have also been described.45,50 VREfm exhibited relatively low prevalence in China compared to the United States and some European countries, where the prevalence of VREfm reached 80.7% and 42%, respectively.1,4 Admittedly, the prevalence of VREfm isolates in China might be underestimated due to the lack of epidemiological data. In this study, the median age of the patients reached 74 years, and the majority of patients (73.9%) with VREfm were from the three ICUs, suggesting the critical condition of the patients. Thus, the patient's prognosis was more associated with his/her clinical conditions upon infection, and it is difficult to determine whether a patient can succumb to VRE-associated infections. Furthermore, it is particularly important to take effective infection control measures for the ICU patients with severe conditions to prevent VREfm-caused infections.
Clonal VREfm spreads are observed in this study, that is, several types of VREfm strains, for example, PFGE type 2, 19, 22, 31, and 36 strains spread to multiple patients. Meanwhile, the horizontal transfer of vancomycin-resistant gene may have transformed some vancomycin-susceptible E. faecium strains into VREfm. Although plasmid analysis revealed that all types of clinical VREfm strains possessed a different plasmid profile, we cannot rule out plasmid spread completely because the plasmid size may change during their transfer and give mosaic structures,8,35 and E. faecium plasmids may change their size due to recombination when they are moving into a different strain background. Furthermore, a multiclone prevalence of VREfm was observed in several other studies,25,36,45 suggesting that the vanA gene has spread, to some extent, among clinical E. faecium strains in China.
Similar to other research findings,18,29,30,45,50 E. faecium ST78 was the most prevalent clone in this study (Table 1), suggesting that some genetic features of this lineage of E. faecium strains conferred them the advantage in acquiring exogenous resistance- and virulence-related determinants. These determinants enable them to survive in the hospital environment, colonize patients, and cause infections. Recent studies have shown that E. faecium lineage 17, 18, and 78 contain various genes, including mobile genetic elements, membrane proteins encoding genes, regulatory genes, and a putative pathogenicity island, which allow them to adapt to the constraints of the hospital environment.4,44 Overall, these data indicate that the presence of special biological characteristics in these lineages has contributed to their increased prevalence in hospital.
VanA-type resistance is characterized by inducible high-level resistance to both vancomycin and teicoplanin.6,7 However, 11 of 38 (28.9%) VREfm strains were susceptible to teicoplanin (with MIC ≤8 mg/L) in this study (Table 1), which was termed the VanB phenotype–vanA genotype VRE.12,19,23 The VanB phenotype–vanA genotype VREfm strains have also been identified in other studies from China.3,11,36,45,50 Vancomycin resistance in vanA+ isolates is mediated by a group of genes, including vanR, vanS, vanH, vanA, vanX, vanY, and vanZ, which are usually carried on the Tn1546 transposon. Point mutations or deletion in the left end of Tn1546 (vanR and vanS) or the genetic rearrangement of the right part of the transposon (vanX, vanY, and vanZ) are responsible for impaired teicoplanin resistance among VanB phenotype–vanA genotype VRE isolates.11,12,19,23 Furthermore, 92.1% (35/38) of VREfm strains were nonsusceptible (resistant or intermediate) to nitrofurantoin, which is an important antimicrobial agent to treat urinary tract infection. Fortunately, all VREfm strains were susceptible to linezolid and tigecycline, which are the only effective antimicrobial drugs for the treatment of VREfm-caused infections (Table 1).
In this study, 100% and 92.1% of VREfm strains carried the esp and hyl gene, respectively (Table 1). This result is in disagreement with other studies performed on these genes, where 76–88.9% and 21.3–58% of VREfm strains were positive for esp and hyl gene, respectively.18,25,30,36 As a specific marker for hospital-associated E. faecium isolates, Esp (encoding an enterococcal surface protein) has been shown to play a significant role in the prevalence of VREfm,16,32,43 while the hyl gene (encoding a putative glycosyl hydrolase) has been reported to be associated with clinical E. faecium CC17 isolates. 27 In addition, all 38 VREfm strains carried acm, sgrA, pilA, and pilB, while 27 (71.1%) and 23 (60.5%) strains were positive for scm and ecbA, respectively (Table 1). The high prevalence of these MSCRAMMs in this study confirmed that they together with esp and hyl played an important role in the emergence of VREfm CC17 in nosocomial infections. However, the exact biological functions of these surface proteins have not been fully studied yet; their roles in VREfm pathogenesis warrant further investigation, which may enhance our understanding of this emerging pathogen.
The present study has limitations. First, because this study was a retrospective analysis with limited patient information, only phenotypic and genotypic characteristics of the clinical VREfm isolates were analyzed, without considering the patients' clinical features. Second, the location (plasmid or chromosome) and the genetic background of vanA gene were not analyzed. Third, other resistance-related determinants of VREfm remained to be characterized. Forth, other virulence factors (such as pstD) have not been investigated. Fifth, we did not analyze all the isolates within each PFGE type for their genotypic features, which may lead to bias because PFGE-identical isolates may have differences in their genetic content.
Contributors
J.Y. designed the study and drafted the article. L.G. performed molecular genetic analysis. L.Y. and Y.M. participated in the collection of strains and clinical details. Y.J. and Y.L. participated in the organization of the study.
Footnotes
Acknowledgment
The study was supported by the China Mega-Project on Infectious Disease Prevention (grant no. 2013ZX10004217-002-002).
Disclosure Statement
No competing financial interests exist.