
Abstract
Introduction
T
In many countries, the emergence of KPC-producing bacteria has been associated with the import of isolates from high-prevalence areas. 5 The Croatian Committee for Antibiotic Resistance Surveillance at the Croatian Academy of Medical Sciences has an ongoing antibiotic resistance surveillance program since 1997 with >90% population coverage (Fig. 1). Since 2001, all carbapenem-resistant Enterobacteriaceae have been flagged as alert organisms that need to be sent for retesting to the Reference Center for carbapenem resistance confirmation and investigation of the resistance mechanism. The occurrence of the first case of KPC-producing K. pneumoniae in Croatia dates from February 2011 and was reported by Bedenic et al. 6 The aim of this study was to perform molecular typing, determine the antimicrobial resistance profile, and analyze the dissemination of KPC producers in Croatia, following the report of the first case in February 2011 on isolates systematically collected throughout the country in the period from February 2011 to August 2013.
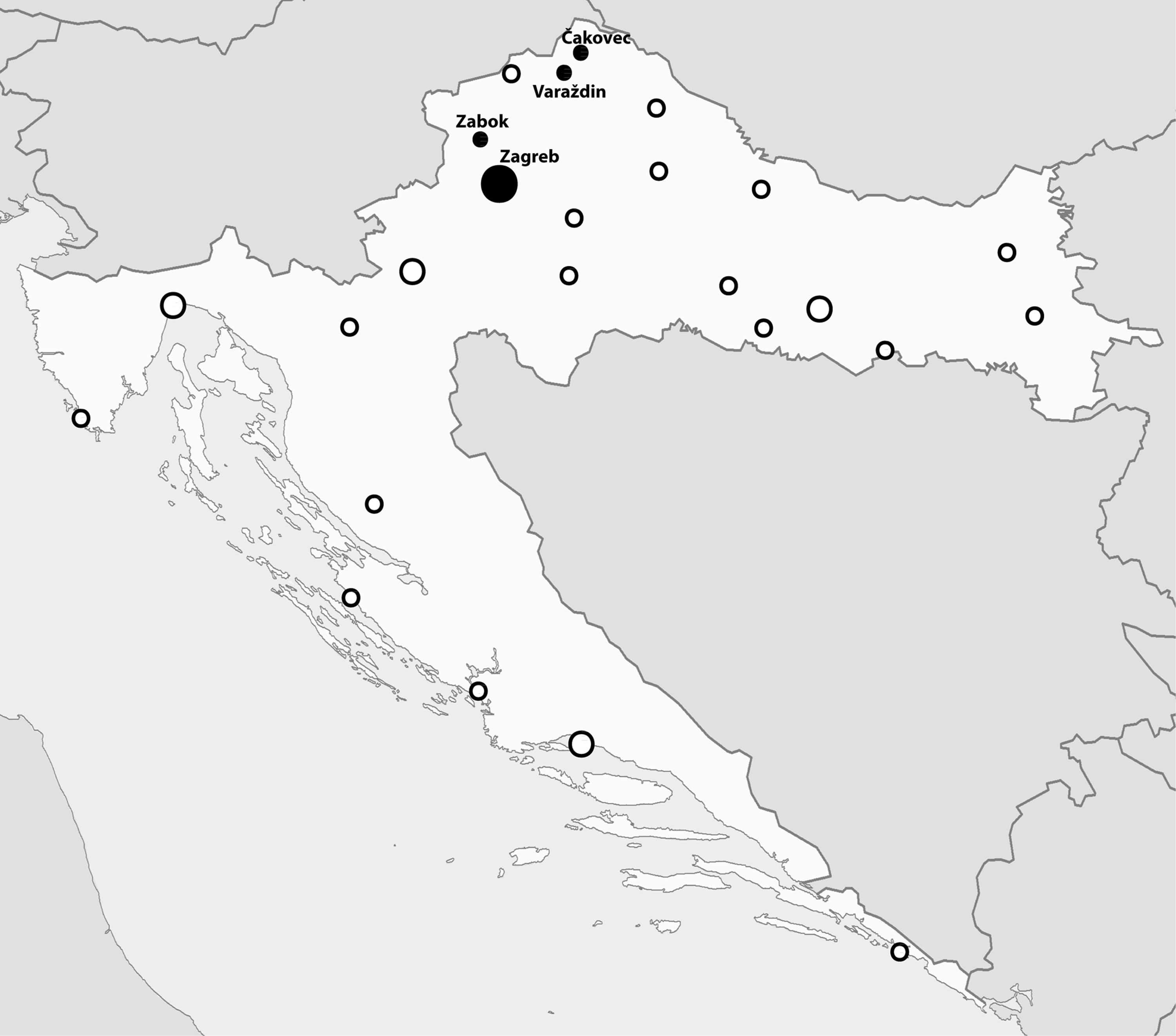
Microbiology laboratories taking part in the Croatian antibiotic resistance surveillance program. ●, Cities with KPC-positive isolates; ◯, Cities without KPC-positive isolates. The size of the circle corresponds to the number of participating laboratories. KPC, Klebsiella pneumoniae carbapenemase.
Materials and Methods
Study isolates
In a period from February 2011 to August 2013, a total of 547 enterobacterial isolates from 40 participating centers were referred to the Croatian Reference Center for Antibiotic Resistance Surveillance based on the nonsusceptibility to ertapenem by disk diffusion according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines. 7 A total of 167 isolates were found to produce carbapenemases (59% VIM, 31% KPC, 8% NDM, 2% OXA-48), of which 51 were KPCs. KPC production was detected in K. pneumoniae only. Three isolates from one hospital were described as a part of a local hospital outbreak elsewhere 8 and were not included in this study. Altogether, 48 KPC isolates from nine centers were included in this study (Table 1). Only one isolate per patient was included in this study. Majority came from three hospitals, another three hospitals had two patients affected, and three hospitals had a single case each. Most KPC isolates were collected from clinical samples, namely urine (n = 13), blood (n = 4), tracheal aspirate (n = 8), skin and soft tissue samples (n = 2), sputum (n = 1), catheter (n = 1), and cerebrospinal fluid (n = 1). Fourteen isolates were recovered from screening samples (stool samples and rectal swabs). Clinical sample information regarding four isolates in this study could not be obtained. As of July 2012, following the Ministry of Health instructions, all hospitals were obliged to perform active ward screening after each KPC case.
Identified using E-test.
KPC isolates that have successfully transferred carbapenem resistance to Escherichia coli A15R.
S, sputum; TA, tracheal aspirate; RS, rectal swab; U, urine; CSF, cerebrospinal fluid; ST, stool; B, blood; WS, wound swab; C, catheter; ND, not determined; H, hospital; ETP, ertapenem; IMP, imipenem; MEM, meropenem; CST, colistin; SXT, trimethoprim–sulfamethoxazole; KPC, Klebsiella pneumoniae carbapenemase; MIC, minimal inhibitory concentration; PFGE, pulsed-field gel electrophoresis.
Species identification
Bacterial species identification was performed using the Vitek2 compact system (BioMerieux). The identification was confirmed by amplification and sequencing of the 16S rRNA encoding gene, followed by BLAST (Basic Local Alignment Search Tool) querying the National Center for Biotechnology Information (NCBI) nucleotide database (http://blast.ncbi.nlm.nih.gov/Blast.cgi). 9
Antibiotic susceptibility testing
Antimicrobial susceptibility testing of isolates was performed by the disk diffusion method, and minimal inhibitory concentrations (MICs) for ertapenem, imipenem, meropenem, and colistin were detected by E-test (BioMerieux). The results were interpreted using EUCAST breakpoints. Phenotypic detection of carbapenemase production was performed by an inhibitor-based method using combination disk testing with EDTA for detection of metallo-β-lactamases and phenylboronic acid for detection of class A β-lactamases. 10
Pulsed-field gel electrophoresis and multilocus sequence typing
Isolates were typed by pulsed-field gel electrophoresis (PFGE) of XbaI digested genomic DNA using the CHEF-DR III System (Bio-Rad Laboratories) as described for Escherichia coli (www.cdc.gov/pulsenet/pathogens/ecoli.html) 11 with modifications taken from the study of Han et al. 12 Electrophoresis was run at 12°C with a pulse time of 6–36 sec at 6 V/cm on a 120° angle in 0.5× Tris/borate/EDTA buffer for 19.5 hr. The restriction patterns were visually inspected and interpreted according to the criteria of Tenover et al. 13 Multilocus sequence typing (MLST) was performed according to the protocol described on the K. pneumoniae MLST web site (www.pasteur.fr/recherche/genopole/PF8/mlst/Kpneumoniae.html).
Molecular characterization of antimicrobial resistance genes
Several genes conferring resistance to different families of antimicrobial agents were tested by polymerase chain reaction (PCR) and sequencing (1) β-lactam agents: class A (blaKPC, blaTEM, blaSHV, blaCTX-M, blaVEB, blaGES, blaPER, bla SME),8,14 class B (blaVIM, blaIMP, blaNDM), plasmid blaAmpC, 15 and class D (blaOXA) 14 ; (2) quinolones: qnrA, qnrB, and qnrS 16 ; (3) aminoglycosides: aadA1/2, aadA5, aac(3)-I, aac(3)-II, aac(3)-III, aac(3)-IV, aph(3′)-Ia, aph(3′)-II, and ant(2′′) 14 ; (4) tetracycline: tet(A)–tet(E) 14 ; and (5) chloramphenicol: cmlA, floR. 14 Sequencing of positive PCR products was performed on ABI310 using BigDye 3.1 technology (Applied Biosystems).
Plasmid analysis
Plasmid number and size in all KPC isolates and obtained transconjugants were determined using S1-nuclease-digested genomic DNA, separated by PFGE using the CHEF-DR III System, as described previously. 17 Subsequently, plasmid DNA was blotted onto a positively charged nylon membrane and hybridized with blaKPC-specific probe using DIG-High Prime DNA Labeling and Detection Starter Kit I (Roche). Furthermore, KPC-harboring plasmids were classified into incompatibility groups using the PCR-based replicon typing (PBRT) scheme and hybridization with replicon FIIs and IncR-specific probes.18,19
Transfer of resistance
Conjugal transfer experiment was carried out by the broth mating method in Luria-Bertani (LB) broth at 37°C, using the E. coli A15R strain as recipient. 8 Transconjugants were selected on LB agar plates supplemented with 256 mg/L rifampicin and 0.5 mg/L meropenem. Transconjugants were subjected to antibiotic susceptibility testing and PCR to determine the presence of blaKPC.
Transfer of resistance for isolate 212/E was not performed due to its resistance to rifampicin.
Results
Clinical cases
KPC-producing K. pneumoniae isolates analyzed in this study represent the entire collection of noncopy KPC isolates gathered from Croatian microbiology laboratories in the period from February 2011 to August 2013 (Table 1). The first KPC-positive K. pneumoniae isolate in this study was recovered in November 2011 from a patient hospitalized in a Zagreb hospital with a history of previous hospitalization in the United States. There are no records of patient travel or hospitalization abroad in other cases. The first interhuman transfer of KPC-producing K. pneumoniae was confirmed in May 2012 in two patients hospitalized at the same ward of a regional hospital northwest from Zagreb. The outbreak in this hospital included 12 patients and ended in December 2012. The first interhospital transfer was documented in June 2012, and until August 2013, altogether six hospitals reported multiple and three hospitals reported single KPC-producing isolates. All affected hospitals are located in Zagreb and the northwest region of Croatia (Fig. 1).
Antibiotic susceptibility testing
All isolates had multidrug-resistant phenotype with high-level resistance to penicillins, cephalosporins, and piperacillin/tazobactam, but showed varying levels of resistance to carbapenems. All isolates were resistant to ertapenem. Twenty isolates were resistant, 4 were susceptible (MIC ≤2 mg/L), and 24 were intermediately susceptible (MIC 4–8 mg/L) to imipenem. Twenty-four isolates were resistant, 22 were intermediately susceptible (MIC 8–4 mg/L), and only 2 were susceptible to meropenem (MIC ≤2 mg/L). All isolates were susceptible to colistin, but expressed resistance to amikacin and ciprofloxacin. The susceptibility to gentamicin and trimethoprim–sulfamethoxazole was common for all isolates except for the PFGE type B isolate (Table 1).
Molecular characterization of the isolates
PFGE demonstrated that all blaKPC-positive isolates were distributed in three patterns (Table 1). Forty-six isolates were indistinguishable and were designated as type A, another isolate demonstrated closely related pattern A1, and one isolate had a different pattern and was designated type B. MLST revealed that all blaKPC-positive isolates in this study displayed ST258. blaKPC was detected by PCR in every isolate and sequencing revealed that they all harbor blaKPC-2. All isolates, except the PFGE type B isolate, harbor blaTEM-116, blaSHV-11, and Aph(3′)-Ia. PFGE type B isolate harbors blaTEM-1, blaSHV-11, cmlA, Aac(3′)-IV, and aad-A. Most prevalent plasmid-borne blaAmpC genes, blaCTX-M and qnr genes were not detected by PCR in any isolate.
Plasmid analysis and transfer of resistance
S1-nuclease-PFGE analysis revealed that all isolates have one–three plasmids ranging in size from ∼60 to ∼210 kb. Southern blot and hybridization with blaKPC-specific probe revealed that blaKPC was located on a single plasmid in all isolates, but varied in size (Table 1). PBRT analysis and subsequent hybridization with FIIs and IncR-specific probes showed that blaKPC-carrying plasmids belonged to the FIIs replicon group, except for isolate 212/E that had the IncR blaKPC-harboring plasmid.
In vitro plasmid transfer experiments using the E. coli A15R strain resulted with transconjugants that were positive for the blaKPC-2 gene. Of 48 KPC isolates, only 12 isolates transferred carbapenem resistance to E. coli A15R (Table 1). Ten transconjugants carried the 160 kb blaKPC-harboring plasmid and two transconjugants carried 180 kb blaKPC plasmids. PBRT analysis and hybridization with FIIs and IncR-specific probe revealed that all blaKPC plasmids in transconjugants belonged to the IncFIIs replicon group.
Discussion
This report highlights the early stage of KPC-producing K. pneumoniae dissemination on a nationwide level in the period following the first case report of KPC-producing K. pneumoniae in Croatia. Isolates analyzed in this study represent the entire collection of noncopy KPC isolates gathered from Croatian microbiology laboratories in the period from February 2011 to August 2013 (Table 1). Even though some diversity among PFGE patterns was observed, MLST analysis revealed that all isolates belong to the pandemic, worldwide disseminated clone ST258. The very first KPC-producing K. pneumoniae isolate in Croatia was reported to belong to ST376 and this observation implies that the epidemic clone was imported through a different route. The KPC-producing K. pneumoniae recovered from a patient previously hospitalized in the United States was found to belong to ST258; however, its PFGE pattern (pulsotype B) and resistance profile differ from those belonging to other isolates. There are no records of patient travel or hospitalization abroad in other cases, so the source of the successful PFGE type A strain remains unknown. High potential for dissemination of the KPC-producing K. pneumoniae ST258 has also been reported earlier and has been implicated in >70% of the outbreaks reported to the U.S. CDC. 11 Since the mid 2000s, the ST258 clone has spread in various parts of the world, including the Middle East, South America, China, and Europe. 20 A high level of resistance to different antimicrobial classes has frequently been observed in KPC-producing isolates worldwide. 21 The resistance profile showing susceptibility to gentamicin is in accordance with earlier reports.22,23 Although colistin-resistant KPC-producing ST258 K. pneumoniae isolates have been reported in Hungary and Greece,24,25 all isolates in this study were susceptible to colistin. Plasmids carrying blaKPC genes, belonging to IncFII and IncR groups, were already observed in K. pneumoniae ST25826,27 and their potential for efficient horizontal spread of blaKPC genes within a narrow host range of Enterobacteriaceae has been documented. 5 This study revealed that most of KPC isolates belonging to epidemic pulsotype (pulsotype A) carry a 160 kb blaKPC plasmid belonging to the FIIS replicon group. This finding strongly suggests that spread of KPC-producing K. pneumoniae isolates in Croatia, in a period from February 2011 to August 2013, was clonal. Slight diversity of S1 plasmid profiles in ST258 organisms has been reported earlier in studies that were conducted during longer time frames and large geographical areas,11,26 which is in accordance with findings documented in our study.
So far, the spread of the outbreak clone has been limited to the northwest region of the country. The ST258, PFGE type A strain, described here demonstrates easy interhuman transfer in hospital settings, which has not been recorded for any carbapenem-resistant enterobacterial strain in Croatia so far. Continuous national efforts and good collaboration among hospitals are needed to prevent further spread of such isolates.
Footnotes
Acknowledgment
This study was funded by the Interdisciplinary Section for Antibiotic Resistance Control (ISKRA) of the Croatian Ministry of Health.
Disclosure Statement
All authors report no competing financial interests exist.