
Abstract
New Delhi metallo-β-lactamase (NDM) is a serious challenge to the treatment of infections and public health. Serbia has been designated as an endemic region for isolates carrying the blaNDM-1 gene, as well as one of several commonly proposed countries of origin. This is the first report of NDM-1-positive Escherichia coli from Serbia. A carbapenem-resistant clinical isolate of E. coli strain IMD989, isolated from the blood culture of a pediatric patient with leukemia, was subjected to antimicrobial susceptibility tests, molecular typing, and conjugation experiments. The strain exhibited resistance to meropenem and was classified as a novel sequence type, ST5123, belonging to E. coli phylogenetic group A. ST5123 showed similarity to veterinary isolates ST93 and ST3977. The blaNDM-1 gene was detected by polymerase chain reaction (PCR) and sequencing. Cloning and sequencing of genomic clones confirmed that strain IMD989 produces an NDM-1 variant. Conjugation experiments, pulsed-field gel electrophoresis, and Southern blot hybridization revealed that blaNDM-1 was located in IMD989 on a transmissible 80 kb plasmid, designated as pIMD989. PCR analysis confirmed that pIMD989 belongs to the IncF plasmid family. Propagation of IMD989 and selected transconjugants carrying pIMD989 over 14 days in solid media with and without antibiotic selection showed that pIMD989 is a stable plasmid.
Introduction
T
Among mechanisms of carbapenem resistance, metallo-beta-lactamases are of great clinical significance since they hydrolyze all beta-lactams, except monobactams, and currently no inhibitor is available for clinical use. Soon after it was described, New Delhi metallo-beta-lactamase (NDM) became one of the commonly isolated and widely distributed metallo-beta-lactamases worldwide. 5 The blaNDM gene has mainly been located on plasmids, enhancing its rapid dissemination and spread among different bacterial species.6,7
Although the blaNDM gene is now disseminated around the globe, there is a presumption that the Indian subcontinent, the Balkans region, and some parts of the Middle East are reservoirs of patients infected by blaNDM-positive bacterial strains.8,9 Furthermore, Serbia has been designated as one of several possible countries of origin for imported isolates carrying blaNDM-1, along with Iraq and Pakistan. 8 Several studies have reported on NDM-1-carrying bacteria from Serbia and dealt with the issue of blaNDM-1 endemicity.10–12 However, it seems plausible that the prevalence of NDM-1-producing bacteria in Serbia is underestimated due to a lack of systematic surveillance.
Although infections caused by carbapenem-resistant Enterobacteriaceae are in the spotlight of the medical community worldwide, the risk factors and clinical outcomes of those infections in pediatric patients are still not well described. 13 However, blaNDM-1 carrying strains have been detected in pediatric patients with a variety of nosocomial and other infections.13–15 The first reported Enterobacteriaceae species producing NDM-1 in Serbia was a Klebsiella pneumoniae isolated from the urine of a 7-month-old male outpatient receiving antibiotic prophylaxis in 2011. 11 In this article, we report on the first case of NDM-1-positive E. coli in Serbia.
Materials and Methods
Bacterial strain and species identification
A clinical isolate of carbapenem-resistant E. coli IMD989 was isolated from the blood culture of a 16-year-old boy who was being treated for acute lymphoblastic leukemia at the Institute for Mother and Child Healthcare “Dr. Vukan Cupic,” a university-affiliated tertiary care pediatric hospital in Belgrade, Serbia, in March 2015. After the last round of intensive chemotherapy, at the point of complete agranulocytosis, he became febrile. Blood cultures were collected and treatment with amikacin, meropenem, ceftazidime, and vancomycin was started. As blood cultures revealed a carbapenem-resistant strain of E. coli, colistin was also added. The boy received granulocyte colony-stimulating factor as well. He became apyrexial after 11 days of antibiotic treatment and at that point his neutrophils recovered. Soon after this septic episode, allogeneic bone marrow transplantation (BMT) was successfully performed and he is currently in complete remission and is followed as an outpatient.
The E. coli isolate was initially identified by the Vitek 2 automated system (BioMérieux, Marcy l'Étoile, France) and identification was confirmed by 16S rRNA gene amplification 16 and subsequent sequencing of the amplicon (Macrogen DNA sequencing service, Netherlands). The resulting sequence was deposited in the European Nucleotide Archive (www.ebi.ac.uk/ena/data/view/LN871242-LN871243, accession No. LN871242). The antimicrobial susceptibility of E. coli IMD989 was determined using the Vitek 2 with an AST-N203 card, according to the manufacturer's recommendations. In addition, antibiotic susceptibility profiles were determined in cation-adjusted Mueller-Hinton broth by microdilution testing, with in-house prepared panels, following the Clinical and Laboratory Standards Institute's Performance Standards for Antimicrobial Susceptibility Testing (24th Informational Supplement. CLSI document M100-S24), using their susceptibility and resistance breakpoints.
Phylogenetic characterization of E. coli IMD989
Phylogenetic group determination of E. coli IMD989 was performed by multiplex polymerase chain reaction (PCR) as previously described. 17 The specific primers used in this method amplify chuA and yjaA genes and a DNA fragment labeled as TSPE4.C2. 17 Identification of an isolate and its classification as a member of a certain phylogenetic group depend on the pattern of its amplicons and were performed as previously described. 17
Molecular typing
Multilocus sequence typing (MLST) was performed by PCR and sequencing of seven housekeeping genes using the primers and conditions defined at the E. coli MLST database of the University of Warwick (http://mlst.warwick.ac.uk/mlst/dbs/Ecoli/documents/primersColi_html). 18 According to the allele profile, isolate IMD989 was categorized as a specific sequence type (ST) using the MLST Database at the University of Warwick. 18
Molecular detection and cloning of blaNDM-1 from the genome of E. coli IMD989
Detection of the gene encoding NDM-1 in clinical isolate IMD989 among the total DNA was performed by the PCR method previously described. 19 To determine which variant of NDM is present in IMD989, we cloned the entire gene from its genome. First, the total DNA of IMD989 was isolated and digested with EcoRI restriction enzyme. The digested fragments of DNA of approximately 1,500 bp in size (the size of the region mapped based on the hybridization signal with blaNDM-1 as a probe) were eluted from the agarose gel using a Gel Extraction Kit (Thermo Fisher Scientific, Waltham, MA) and cloned into pBluescript KanR. 10 The ligation mixture was transformed into E. coli DH5α and the transformants were selected onto Luria Bertani (LB) medium supplemented with kanamycin (100 μg/ml) and ampicillin (100 μg/ml). The transformant that was resistant to both kanamycin and ampicillin was selected, and the plasmid construct carrying blaNDM-1 was isolated, and the entire blaNDM-1 gene was sequenced. Sequencing was performed by the Macrogen DNA Sequencing Service (Amsterdam, Netherlands). The resulting sequence was deposited in the European Nucleotide Archive (www.ebi.ac.uk/ena/data/view/LN871242-LN871243, accession No. LN871243).
Plasmid studies
The transfer of the blaNDM-1 gene carried by plasmid pIMD989 from clinical isolate IMD989 was done with azide-resistant E. coli J53 as a recipient strain, under appropriate safety conditions, as previously described. 7 The log cultures of the recipient (J53) and donor (IMD989) strains were added in a ratio of 1:10 (107 and 108 colony forming units) to LB broth and left overnight at 30°C, 37°C, and 42°C. Various dilutions of overnight cultures in physiological saline (10−2 to 10−7) were plated onto selective media supplemented with 100 μg/ml sodium azide and 0.5 μg/ml meropenem and incubated for 24 h at 37°C. The donor and recipient suspensions were also diluted in physiological saline (10−5) and plated onto LB agar to confirm the homogeneity of the cultures and to estimate the colony count. Conjugations were carried out as three independent experiments for each temperature.
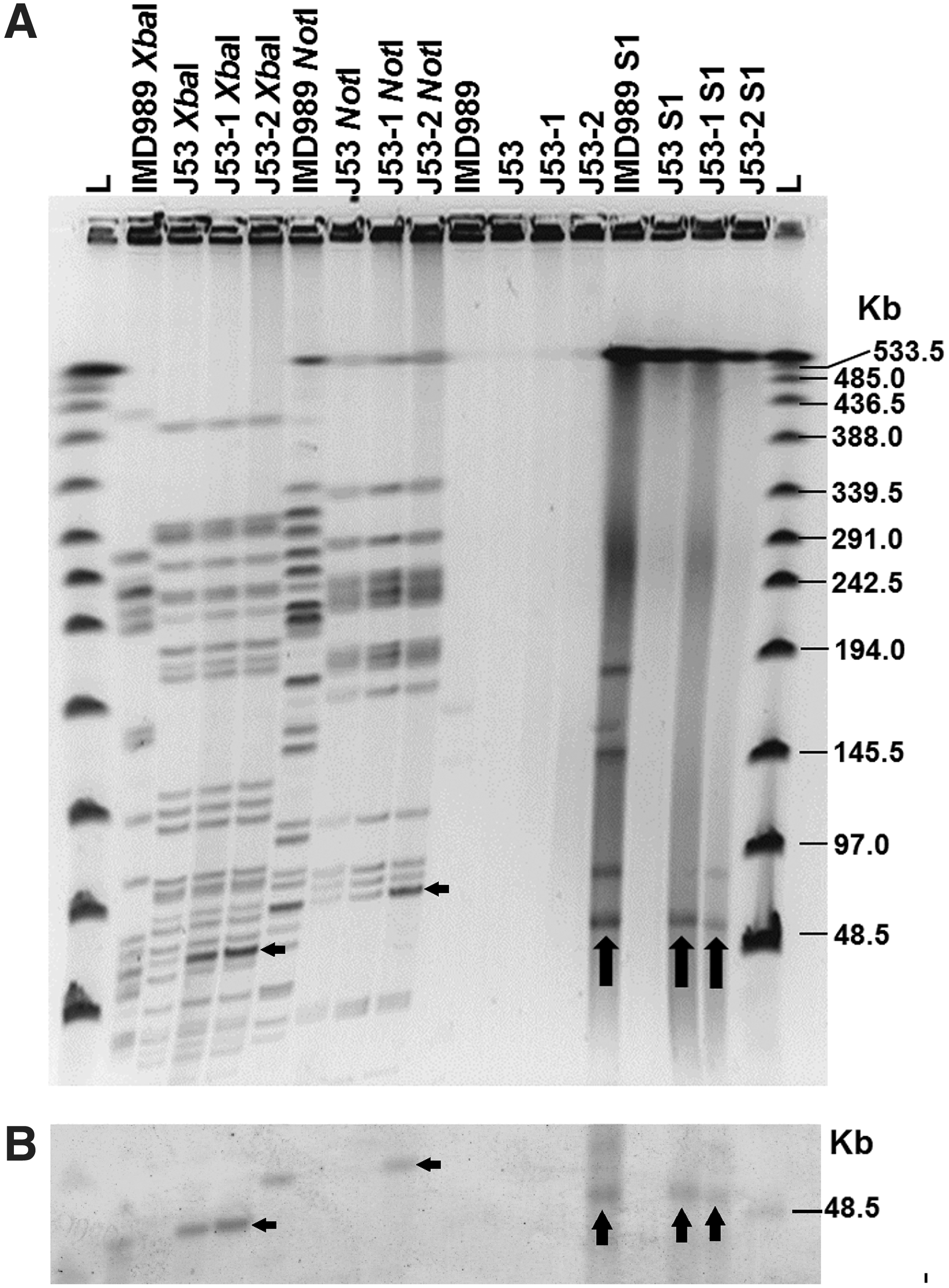
After conjugation, the transconjugants (J53-1 and J53-2) were first confirmed by PCR with primers specific for blaNDM-1. For further confirmation of transconjugants, and determination of blaNDM-1 gene localization in IMD989, Pulsed-field Gel Electrophoresis (PFGE) and S1 nuclease assays were performed, followed by Southern blot hybridization with blaNDM-1 as a probe.
DNA preparation and restriction enzyme digestion of clinical isolate IMD989, E. coli J53, and two blaNDM-1-positive transconjugants (J53-1 and J53-2) for PFGE were performed as previously described. 10 The DNA was digested with restriction enzymes XbaI, NotI, and S1 nuclease or not digested. PFGE was performed with a 2015 Pulsafor unit (LKB Instruments, Bromma, Sweden) equipped with a hexagonal electrode array for 18 h at 300 V at 9°C. The gels were stained with ethidium bromide and photographed under UV illumination. The DNA fragments were transferred to a nylon membrane (SensiBlotPlus Nylon Membrane, UAB Fermentas, Lithuania), hybridized with a digoxigenin-labeled probe specific to blaNDM-1, and detected using an NBT/BCIP Color Detection Kit (Thermo Fisher Scientific).
To determine the replicon type for the plasmid carrying the blaNDM-1 gene in E. coli IMD989, PCR-based replicon typing was performed with a transconjugant, which carries a single plasmid encoding blaNDM-1, as previously described. 20 The specific primers, which were used for replicon typing, allowed the determination of the plasmid's incompatibility (Inc.) among FIA, FIB, FIC, HI1, HI2, I1-Iγ, L/M, N, P, W, T, A/C, K, B/O, X, Y, F, and FIIA incompatibility groups. 20
We determined the stability of the plasmid carrying blaNDM-1 by serial passage of IMD989 and the selected E. coli J53 transconjugants on antibiotic-free solid LB and solid LB containing 0.5 mg/L meropenem. Carriage of blaNDM-1 was assessed by PCR with specific primers. A plasmid is considered to be unstable if it is lost after two consecutive overnight passages.
Results
Antimicrobial susceptibility of E. coli IMD989
The antimicrobial susceptibility of E. coli IMD989 was initially determined using a Vitek 2 automated system and microdilution testing in cation-adjusted Mueller-Hinton broth (Table 1). According to microdilution testing, strain IMD989 showed resistance to all analyzed beta-lactam antibiotics, except aztreonam. The same pattern of resistance to beta-lactams was found for transconjugant E. coli J53 pIMD989 (Table 1).
MIC, minimum inhibitory concentration; ND, not determined.
Molecular typing and phylogenetic characterization of E. coli IMD989
MLST (http://mlst.ucc.ie/mlst/dbs/Ecoli) and PCR-based phylogroup analysis identified E. coli IMD989 as having a novel sequence type, ST5123, belonging to phylogroup A. Interestingly, according to the database, the closest types to ST5123 are ST93, recovered from the feces of healthy dogs, 21 and ST3977, which is an avian isolate. 22
Molecular basis of resistance and plasmid studies
The presence of blaNDM-1 in the genome of IMD989 was confirmed by PCR. However, since Taq polymerase is a moderately faithful enzyme, and to avoid eventual mismatches introduced by the enzyme, we cloned a 1059 bp EcoRI fragment from the genome of the strain IMD989 containing the entire blaNDM-1 gene. This was done to determine which of the NDM variants are present in the genome of IMD989.
Genetic localization of the blaNDM-1 gene in the genome of IMD989 was determined by conjugation experiments. Conjugation was performed in liquid media at 37°C using azide-resistant E. coli J53 as the recipient strain, and E. coli J53 blaNDM-1 transconjugants appeared after 16 h of cultivation on a selective medium. The presence of blaNDM-1 in the transconjugants was confirmed by PCR, and further confirmation tests included PFGE, an S1 nuclease assay, and Southern blot hybridization with blaNDM-1 as a probe. The S1 nuclease assay revealed that, although E. coli IMD989 carries several plasmids, only one plasmid, of at least 80 kb (according to PFGE NotI digestion), was transferred to E. coli J53 transconjugants (Fig. 1.). A Southern blot experiment revealed that blaNDM-1 is located on a transferred plasmid both in IMD989 and in the transconjugants (J53-1 and J53-2), and the plasmid was designated as pIMD989 (Fig. 1).
Detailed plasmid analysis, including replicon typing, efficiency of conjugation transfer, and stability testing were performed. Replicon typing for a plasmid isolated from transconjugants carrying blaNDM-1 revealed that it is an IncF replicon. Conjugation efficiency at 30°C, 37°C, and 42°C was determined to get insight into its dissemination ability. The highest rate of conjugation was at 30°C where it was 3.3 × 10−7, while the efficiency at 37°C and 42°C was significantly lower (10−8). Passaging of IMD989 and selected transconjugants carrying pIMD989 over 14 days on solid media with and without meropenem (0.5 mg/L) showed that pIMD989 is a stable plasmid.
Discussion
The development of resistance to carbapenems by E. coli and other Enterobacteriaceae is a burning issue. 23
Carbapenemases, and especially NDM, have become a major public health concern due to their rapid dissemination worldwide and association with other determinants of resistance to antibiotics. 24
Most of the outbreaks of NDM-producing bacteria have indicated a link with the Indian subcontinent, the Balkan countries, 25 and the Middle East. 26 However, all documented cases in Serbia have been linked to one adult tertiary referral hospital. E. coli IMD989 is the first NDM-1-producing strain to be discovered in a pediatric hospital in Serbia, as well as the first NDM-1 producing E. coli from Serbia.10,11
A number of antibiotics (ciprofloxacin, levofloxacin, fosfomycin, nitrofurantoin, and aztreonam) were active against E. coli IMD989, offering therapeutic options. It is interesting that E. coli IMD989 was sensitive to fluoroquinolones, since the prevalence of NDM-1-positive strains susceptible to fluoroquinolones is very low. This was shown in a study by Kumarasamy et al. (2010) wherein the sensitivity rates of 180 NDM-1-producing Enterobacteriaceae strains to ciprofloxacin were only 5–10%. 6
The blaNDM-1 gene that occurs in E. coli belongs to diverse phylogenetic lineages. Phylogenetic group B1 was the most frequent host lineage among these isolates from Europe and the Indian subcontinent and the second most frequent was phylogenetic group D.27–30 Serbian isolate IMD989 belongs to phylogroup A. Although rare, other documented cases of NDM-1-producing E. coli from Europe have shown to belong to phylogroup A. 31
As was stated in the Results section, E. coli IMD989 has been designated as ST5123, and according to the MLST E. coli database of Warwick University, this strain type is most similar to ST93 and ST3977, which were isolated from the feces of healthy dogs and birds, respectively. This is of great importance because animals, especially companion animals, are unique and are critical factors related to the potential spread of antimicrobial resistance. 32 Close contact by humans with companion animals creates opportunities for interspecies transmission of antibiotic-resistant bacteria, including carbapenem-resistant strains.33,34 This is speculative, however, since the current knowledge of many aspects of this field is limited and no specific risk assessment has been performed so far.
A previous study by our group, based on the screening of environmental waters in Belgrade, where human cases of NDM-1 infection were documented, indicated that Serbian NDM-1 is in fact a nosocomial, rather than an environmental issue, and that Serbia may not be an endemic region for NDM-1. 12 However, this research did not take into account animals as potential reservoirs of NDM-1. Thus, the role of wildlife and companion animals in the dissemination of blaNDM-1 needs to be assessed to resolve the NDM-1 endemicity issue in Serbia and other parts of the Balkans.
Footnotes
Acknowledgment
This work was supported by grant No. 173019 from the Ministry of Education, Science and Technological Development of the Republic of Serbia.
Disclosure Statement
No competing financial interests exist.