
Abstract
This study assessed the antimicrobial resistance of airborne Staphylococcus spp. strains isolated from healthcare facilities in southern Poland. A total of 55 isolates, belonging to 10 coagulase-negative staphylococci (CoNS) species, isolated from 10 healthcare facilities (including hospitals and outpatient units) were included in the analysis. The most frequently identified species were Staphylococcus saprophyticus and Staphylococcus warneri, which belong to normal human skin flora, but can also be the cause of common and even severe nosocomial infections. Disk diffusion tests showed that the bacterial strains were most frequently resistant to erythromycin and tetracycline and only 18% of strains were susceptible to all tested antimicrobials. Polymerase chain reaction amplification of specific gene regions was used to determine the presence of the Macrolide–Lincosamide–Streptogramin resistance mechanisms in CoNS. The molecular analysis, conducted using specific primer pairs, identified the msrA1 gene, encoding active efflux pumps in bacterial cells, as the most frequent resistance gene. As many as seven antibiotic resistance genes were found in one isolate, whereas the most common number of resistance genes per isolate was five (n = 17). It may be concluded that drug resistance was widely spread among the tested strains, but the resulting antimicrobial resistance profile indicates that in the case of infection, the use of antibiotics from the basic antibiogram group will be effective in therapy. However, before administering treatment, determination of the specific antimicrobial resistance should be conducted, particularly in the case of hospitalized patients.
Introduction
F
Therefore, understanding the mechanisms of such resistance and the underlying genetic phenomena progress the search for new substances (drugs, disinfectants, and antiseptics) active against staphylococci, including multiresistant strains, responsible for nosocomial infections.
Currently, the most frequently identified resistance mechanisms in Staphylococcus spp. include the following: enzymatic inactivation of antibiotic particles involving hydrolases and transferases; active removal of antibiotics from the cell with the so-called efflux mechanism pumps and changing the drug affinity or duplication of target site functions due to mutations within genes encoding proteins representing the target for antibiotics, which may result in a reduction of its binding affinity to the drug. 6 From an epidemiological point of view, the phenomenon of increasing antimicrobial resistance is very dangerous and requires careful monitoring.
Therefore, the primary aim of this study was to isolate and identify species of airborne Staphylococcus strains in selected healthcare facilities in southern Poland. A further aim was to determine the drug resistance profiles of the strains, followed by determination of the presence of genes conferring the resistance to antibiotics of the macrolides, lincosamides, and streptogramins (MLS) group in the examined strains.
Materials and Methods
General overview
Airborne Staphylococcus spp. strains were isolated from 10 healthcare facilities using a single-stage impactor and a Chapman medium. Staphylococcal strains, identified to the species level by API Staph tests, were subjected to disk diffusion tests to assess their antimicrobial resistance profile, followed by polymerase chain reaction (PCR) analyses to determine the presence of genes conferring bacterial resistance to the MLS group of antibiotics.
Air sampling
Bacteria of the genus Staphylococcus were isolated from the air of 10 healthcare facilities in southern Poland 7 (Table 1). The selection of facilities was based on the consent to anonymously participate in this study given by their authorities. In total, 18 randomly chosen different healthcare facilities were contacted, thus, the acceptance rate was 55.6% of the contacted centers. The air sampling was conducted between 2014 and 2015. Each facility was sampled four times, ensuring one sampling per season, that is, spring—April 2014, summer—August 2014, autumn—November 2014, and winter—February 2015, when the patients were present. The samples were collected in triplicate using a MAS-100 (Merck) air sampler set to collect 100 L of air during 1 min, according to the requirements given by the Polish Standard PN-Z-04008-08:1989. 7 Chapman medium (BioCorp) was used for the isolation of Staphylococcus spp. After sampling, the Petri dishes were transported to the laboratory and incubated at 36°C ± 1°C for 48 hr.
ICU, intensive care unit.
Isolation of pure staphylococci cultures
Initial selection of cultures likely to be Staphylococcus spp. was conducted according to the methods outlined in Kloos and Schleifer, 8 Kloos and Bannerman, 9 Gaillot et al., 10 and Murray, 11 detailed below. Pure Staphylococcus spp. cultures were obtained by plate streaking of macroscopically characteristic colonies, grown on Chapman medium. Gram-stained smears were then microscopically observed, followed by a furazolidone susceptibility test to distinguish between Staphylococcus and Micrococcus isolates. Strains susceptible to furazolidone were qualified as Staphylococcus, while the remaining ones (furazolidone resistant)—as Micrococcus. Subsequently, a catalase test was conducted to exclude the presence of catalase-negative streptococci from the cultures obtained. Strains within the Staphylococcus genus were differentiated into coagulase positive and coagulase negative by using free coagulase. The final step of phenotypic identification included biochemical tests conducted using API-Staph system (BioMérieux).
Antimicrobial resistance, disk diffusion method
Disk diffusion tests on Mueller-Hinton Agar II (BioMérieux) were conducted to investigate the susceptibility of the strains to six antibiotics representing a different class: cephamycins (cefoxitin—FOX 30 μg), macrolides (erythromycin—E 15 μg), lincosamides (clindamycin—DA 2 μg), fluoroquinolones (ciprofloxacin—CIP 5 μg), tetracyclines (tetracycline—TE 30 μg), and a bacteriostatic drug trimethoprim/sulfamethoxazole (SXT 1.25/23.75 μg), all manufactured by Oxoid. The bacterial susceptibility assessment was conducted according to the guidelines of The European Committee on Antimicrobial Susceptibility Testing—EUCAST 12 presented by the National Reference Centre for Antimicrobial Susceptibility Testing (pol. Krajowego Ośrodka Referencyjnego ds. Lekowrażliwości Drobnoustrojów—KORLD; www.korld.edu.pl; IV).
Reference strains of methicillin-susceptible S. aureus ATCC 25923 and methicillin-resistant S. aureus MR 3, derived from the collection of the Jan Bober Center for Microbiological Research and Autovaccines in Krakow, were used as positive and negative controls, and the results were interpreted according to the recommendations of KORLD and EUCAST. 12
Determination of genes responsible for the resistance to MLS group antibiotics
DNA extraction from pure cultures of staphylococci was conducted using the Genomic Mini Kit (A&A Biotechnology), following the manufacturer's instructions. Subsequently, the presence of 17 genes conferring resistance in Staphylococcus spp. strains to antibiotics of MLS group was determined by conducting PCR with specific primer sets. Brief characteristics of each of the tested gene regions along with sequences of primers used to amplify them are provided in Table 2. PCR amplification was carried out in a T100 thermal cycler (Bio-Rad), under temperature conditions optimal for each primer (Table 2).
PCR was carried out in 25 μl volumes containing water, 50 ng of DNA template, 12.5 pM of each primer, 2.5 mM of each dNTP, 1× PCR DreamTaq Green buffer, and 1 U DreamTaq DNA polymerase. The PCR products were subjected to electrophoresis for 60 min on a 1% agarose SimplySafe (EurX) stained gel in 1× TBE. The products were visualized in UV light and documented using the Gel Doc (Bio-Rad) system. GeneRuler™ DNA Ladder Mix, 100–1,000 bp (Thermo Scientific) was used to assess the length of the analyzed PCR products (Table 2).
Statistical analysis
To test for the significance of differences between the antimicrobial resistance in strains isolated from individual groups of sites, that is, outpatient and inpatient units, a χ2 test was conducted using a Social Science Statistics calculator. 19
Results
Sampling at the 10 sites yielded 55 strains of staphylococci, 15 from outpatient units and 40 from inpatient units. A total of 10 staphylococcal species were represented among the 15 isolates derived from the outpatient sampling sites, each species was isolated one to three times (only in the case of Staphylococcus simulans and Staphylococcus hominis). A total of 10 staphylococcal species were represented among the 40 isolates derived from the inpatient sampling sites, with species such as S. saprophyticus and S. warneri very abundantly represented (i.e., 13 and 12 isolates, respectively).
In contrast, Staphylococcus capitis, Staphylococcus epidermidis, and Staphylococcus cohnii were not detected in the inpatient units. Five out of the mentioned 13 S. saprophyticus isolates were derived from the isolation ward of the intensive care unit (ICU) and another five from the cardiology ward. In addition, 4 out of 12 isolates of S. warneri were derived from the cardiology ward and 6 isolates from the patient room of the ICU. No seasonal differences were observed in the frequency of individual species. The most frequently detected species, that is, S. saprophyticus and S. warneri, were isolated evenly throughout the year and the same two species, S. saprophyticus and S. warneri, were the predominant ones in the group of bacterial isolates (Table 3).
For these species, the API Staph identification was reported by Mkrtchyan et al. 20 to produce discrepancies in the results compared to the results provided by 16S RNA sequencing and MALDI-TOF.
MALDI-TOF, Matrix Assisted Laser Desorption Ionization Time-of-Flight.
Disk diffusion tests assessed the susceptibility of the bacterial isolates to six antimicrobials, and the results are presented in Fig. 1. Resistance to tetracycline and erythromycin was observed most frequently (49%, n = 27 isolates and 42%, n = 23 isolates, respectively). Conversely, there were no isolates resistant to gentamicin or trimethoprim/sulfamethoxazole.
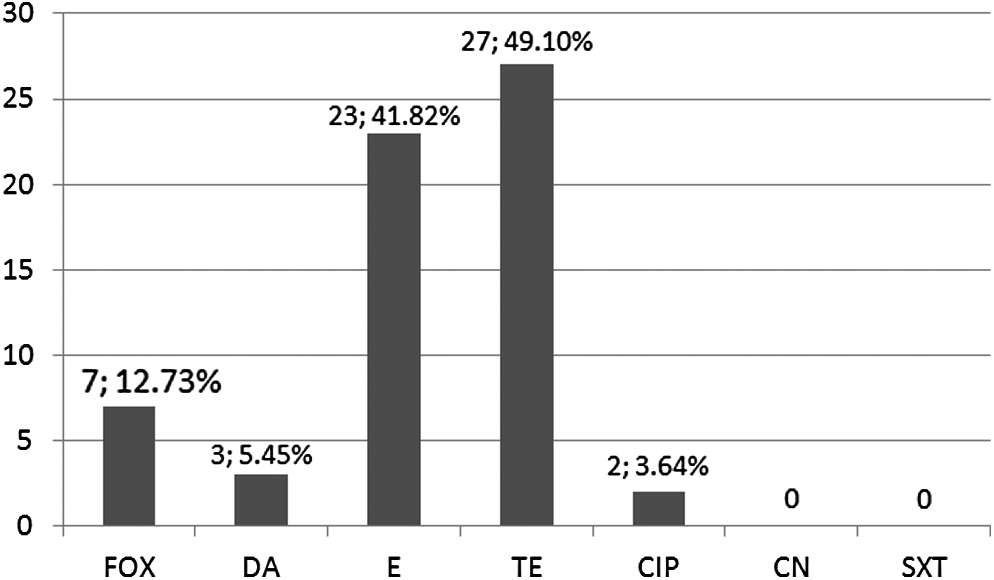
The number and percentage of isolates resistant to the tested antimicrobials. The total number of isolates used in the study was n = 55.
The majority of the tested Staphylococcus spp. isolates were resistant to one (23 isolates—42%) or two antibiotics (19 isolates—35%). The resistant isolates were most frequently detected in the air of patient rooms at the cardiology ward (10 isolates—18%) and ICU (9 isolates—16%). Only one isolate was resistant to three antibiotics (S. simulans, hospital 1) and one isolate to four antibiotics (S. hominis, allergology outpatient clinic).
The distribution of mechanisms of resistance to macrolides, lincosamides, and streptogramins B is shown in Fig. 2. The most common mechanism of resistance to antibiotics of MLSB type in staphylococci is the inducible mechanism (62%, n = 16). The second most frequent mechanism of resistance was MSB type, observed in seven isolates (28%). In contrast, only one isolate (4%) showed the constitutive MLSB.
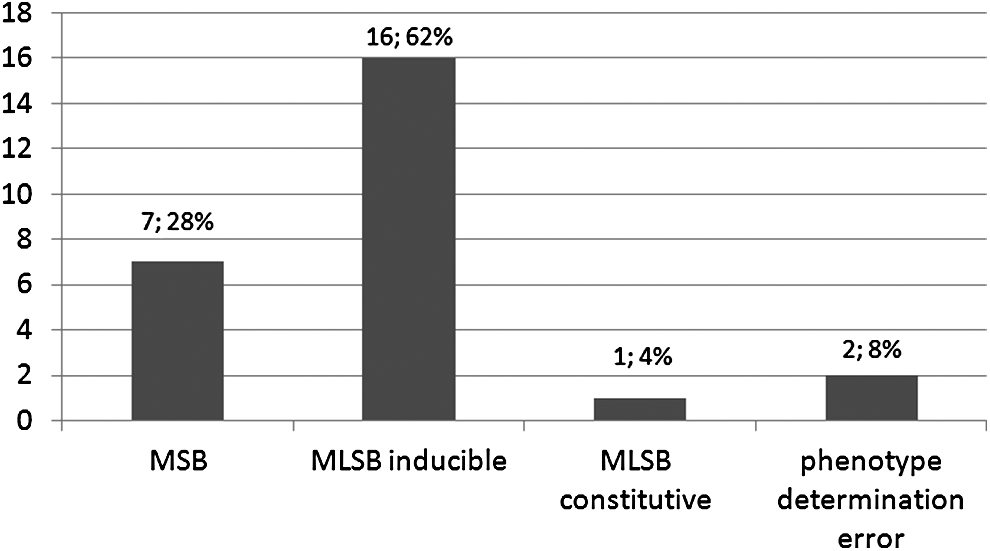
The number and percentage of isolates exhibiting the resistance mechanisms to MLSB type antibiotics. The total number of isolates used in the study was n = 55.
The presence of ermB and ermB1 genes in this study was demonstrated in 11% and 55% of strains, respectively. It can be stated that the msrA1 gene, determining the inducible resistance to erythromycin and streptogramins B in staphylococci (MSB phenotype), was found in the greatest number of the analyzed bacterial isolates of coagulase-negative staphylococci (CoNS; n = 49 isolates, 98%, Fig. 3). Moreover, the genes, msrA, msrA1, msrB, mphC, lnuA, and ermB1, were found in more than half of the tested strains (56%, n = 31; 89%, n = 49; 58%, n = 32; 62%, n = 34; 58%, n = 32; and 55%, n = 30 isolates, respectively). In contrast, during the conducted analyses, the presence of the following genes was not detected: ereA, ermA, ermA1, ermC, vga, vgb, vat, and vatB. The presence of the msrA1 gene was observed in all Staphylococcus spp. strains exhibiting the inducible mechanism of resistance, while the genes msrA and msrB were present in 94% of those strains. Genes mphC and ermB1 were present in 81% of strains, while lnuA gene—in 75%. Only one of all isolated strains of the species Staphylococcus haemolyticus did not have any of the genes determining the resistance to MLSB antibiotics. The greatest number of antimicrobial resistance genes, as many as 7 (msrA, msrA1, msrB, mphC, lnuA, ermB, ermB1), was observed in Staphylococcus xylosus. Most frequently (n = 17), the bacterial isolates possessed as many as five different antimicrobial resistance genes.

The prevalence of genes determining the resistance to MLSB antibiotics in the analyzed bacterial strains. MLS, macrolides, lincosamides, and streptogramins.
The χ2 tests, performed to assess the significance of differences in the susceptibility of bacterial isolates to individual antimicrobials in strains of Staphylococcus spp. isolated from different groups of sites (divided into two groups—inpatent units, i.e., hospitals and outpatient clinics), confirm a statistically significant difference in the incidence of resistant strains (p < 0.05) for cefoxitin, clindamycin, and tetracycline. The value of χ2 statistics for these antibiotics is 14.04, 5.55, and 11.79, respectively.
Discussion
The species identification of the strains in this study demonstrated that the airborne CoNS isolated from the healthcare facilities belonged to species that rarely cause infections. These are often saprophytic species, such as S. epidermidis, which in most cases do not cause any unwanted symptoms in people with properly functioning immune systems. However, the species identification method used in this study has certain limitations. It has been reported by other authors, for example, Mkrtchyan et al., 20 to produce discrepancies when compared to other, more accurate, methods such as 16S rDNA sequencing and/or Matrix Assisted Laser Desorption Ionization Time-of-Flight (MALDI-TOF). For instance, in the study, staphylococcal strains, identified by API ID32 STAPH as S. saprophyticus, were identified as S. warneri by both MALDI-TOF and 16S rDNA sequencing. In contrast, S. warneri identified by API STAPH was identified as Staphylococcus pasteuri by MALDI-TOF and sequencing.
Nevertheless, in the current study, similar to the one by Augustowska and Dutkiewicz, 21 no strains of S. aureus were isolated, which is considered a major factor in hospital-acquired infections. Although all identified isolates were CoNS, which until recently have been described as only commensals of healthy human skin and mucosa, now they are more frequently being reported as important opportunistic pathogens, sometimes causing even severe nosocomial infections. 22
It must be stressed that the origin of the examined airborne staphylococcal strains is not known and they could have been transferred to the hospital/outpatient clinics from the skin of patients, their families, or personnel. Alternatively, they could be strictly environmental strains. However, the majority of identified species can act as opportunistic pathogens in immunocompromised patients. The most abundant species detected in this study was S. saprophyticus, and although it is a common component of human microflora, it is also one of the most frequent agents of community-acquired urinary tract infections.23,24 It should also be noted that only one out of 14 S. saprophyticus isolates detected in this study originated from an outpatient clinic, while the remainder was isolated from hospitals, including five isolates from the cardiology ward and five from the isolation room of an ICU (Table 3). Patients in these units are often immunocompromised or elderly, and S. saprophyticus could cause severe infections in such patients. The second most frequent species, S. warneri, has been also reported as the causal agent of infections in hospitalized patients and the cause of, among others, ventricular shunt infections, endocarditis, and even sepsis.25,26 Out of 13 S. warneri strains isolated in this study, 4 were from the cardiology ward and 6 from a patient room of an ICU, with sampling conducted when the patients were present in the room. These findings are one of the most important observations of this study, as the presence of such CoNS species (both S. warneri and S. saprophyticus) can cause difficult to treat infections in patients of such healthcare units.
The studied isolates were predominantly resistant to tetracycline (n = 27; 49%), which may be due to the fact that this antibiotic shows bacteriostatic effects, thus not leading to the bacterial cell death, but only decreasing proliferation. Moreover, tetracyclines show antagonistic effect with cephalosporins and penicillins, which may result in elimination of their effects. The finding of frequent resistance of the strains to erythromycin, that is, as much as 42% (23 isolates), may in contrast result from it being the oldest and longest administered macrolide antibiotic. This could have contributed to the increase in bacterial resistance to this drug. 27
Disk diffusion tests showed that 62% of the analyzed Staphylococcus strains possessed an inducible mechanism of resistance to antibiotics of the macrolide, lincosamides, and streptogramin B group. Therefore, the treatment of infections caused by strains presenting such resistance mechanisms should not involve macrolides, lincosamides, or streptogramins B. Such isolates are being reported as resistant to clindamycin because it causes the selection of mutants exhibiting the constitutive mechanism. For the constitutive mechanism, this share was only 4%. These results were opposed to Lina et al., 13 who observed that among CoNS the inducible mechanism was present in 28.7% strains, while the constitutive mechanism was present in 36.6%. In addition, Castro-Alarcon et al. 28 found that among S. epidermidis strains, 47% showed the constitutive mechanism and only 8% the inducible mechanism.
Frequent administration of antibiotics of the macrolide class selects resistant strains much more rapidly than using β-lactam antibiotics. 27 The inducible mechanism results from the production of methylases, which are produced due to the induction of erm genes by 14- and 15-membered macrolides, such as erythromycin. Clindamycin does not induce this mechanism, however, there is a risk that after its application therapeutic effects will not be achieved and that it will cause the selection of bacteria showing the constitutive MLSB mechanism of resistance. This involves the formation of the resistance to macrolides, lincosamides, and streptogramins B in such strains. 12
The genes msr (msrA, msrA1, and msrB), causing resistance to MLSB type antibiotics, were the most frequently detected genes in this study. They determine the inducible mechanism of resistance to erythromycin and streptogramins B in staphylococci (MSB). 14 They differ from the ones exhibiting an MLSB phenotype by the lack of cross-resistance to lincosamides or 16-membered lactone ring macrolides, even after induction. In this study, both erm and lnuA genes were observed to co-occur in 45% of the Staphylococcus spp. strains tested.
One of the tested isolates, identified as S. xylosus, showing the constitutive mechanism of resistance, possessed both msrA1 and mphC genes. Thus, introducing macrolides during antimicrobial therapy will be ineffective in the case of this strain. The presence of the active msrA1 gene will result in active pumping of the antibiotic out of the bacterial cell, while the expression of mphC gene will cause inactivation of the drug due to the phosphotransferase activity. 18 In their study on S. epidermidis isolates, Castro-Alarcon et al. 28 detected the presence of ermA, ermB, ermC, msrA, lnuA, and vga genes in the tested strains. As many as 32% of isolates tested in their study possessed the ermA gene, which was often accompanied by the vga gene in the same isolate. The genes were observed in the bacterial strains exhibiting a constitutive resistance mechanism to MLSB antibiotics. Contrary to this, in our study, none of the CoNS strains possessed ermA or vga genes.
The development of the antimicrobial resistance in Staphylococcus spp. is a process that is influenced by numerous factors, among which belong antibiotic overuse and misuse both in treatment of infections and in nonmedical areas, as well as gaps in infection control programs. 29 The PCR tests allowed detection of antibiotic resistance genes that can be, but not necessarily are, expressed, and therefore, the results of the molecular analyses may vary from the results of disk diffusion tests. However, a high percentage of the CoNS strains were resistant to various antibiotics, and an abundance of antibiotic resistance genes was present.
Taking into consideration the fact that CoNS are widely spread in the community, both as skin commensals and widespread colonizers of the human gut, they may serve as a wide reservoir of antibiotic resistance genes, and the same applies to S. aureus strains. 30 New mechanisms of antimicrobial resistance, their factors, and ways of eradication are constantly being identified and investigated. Unfortunately, we are often unable to limit the increase in antibiotic resistance, as among other factors, it results from naturally occurring horizontal gene transfer. Such observations and studies are very important for control programs of nosocomial infections and stress the importance of implementing surveillance studies to monitor the development and spread of antimicrobial resistance among airborne staphylococcal strains in Polish healthcare facilities.
Conclusions
The predominant species within the group of isolated airborne staphylococci included S. saprophyticus and S. warneri. The tested bacterial isolates were most frequently resistant to erythromycin and tetracycline. Drug resistance was widespread with over 82% of isolates resistant to one or more antimicrobials. In addition, wide variation both in the presence and composition of genes determining antimicrobial resistance was observed among the tested airborne strains of Staphylococcus spp. The msrA1 gene, which is involved in the active efflux of macrolides out of the bacterial cell, was most frequently found in the tested group of isolates. However, before administering treatment, the mechanism of antimicrobial resistance should be determined, particularly in the case of hospitalized patients.
Footnotes
Acknowledgments
This study was funded by the statutory measures of the University of Agriculture—Grant No. DS 3102/KM/2014 and by measures of the Centre for Microbiological Research and Autovaccines in Kraków.
Disclosure Statement
No competing financial interests exist.