
Abstract
Raoultella planticola is a gram-negative bacterium that rarely causes diseases in humans. Here, we present a case of hospital-acquired pneumonia caused by R. planticola that likely originated in the gastrointestinal tract. To the best of our knowledge, this is the second report describing the detection of the gene New Delhi Metallo-β-lactamase-1 (blaNDM-1) in multidrug-resistant R. planticola. Clinical samples were collected for bacterial culture and antimicrobial susceptibility testing from a patient during hospitalization. The presence of blaNDM-1 was detected by PCR and sequencing. An NDM-1-positive R. planticola was isolated from the sputum and stool of the same patient. Further findings confirmed that blaNDM-1 was located on a plasmid. Isolates from the sputum and stool cultures were identical, suggesting that the R. planticola may have originated in the gastrointestinal tract. The patient completely recovered and was discharged after treatment with tigecycline combined with levofloxacin, for a week. In conclusion, R. planticola is a possibly underestimated pathogen that contributes to the spread of the blaNDM-1 gene. Early and precise identification of this pathogen can lead to better prognosis of the associated infections and an improved approach to controlling the spread of carbapenemase-resistant gram-negative bacteria.
Introduction
R
Case Presentation
This study was performed in China, with approval from the Ethics Committee of Zhejiang University. Written informed consent was obtained from the patient not only for sampling but also for publication of the case. Medical records were reviewed for administration of antimicrobial therapy and determination of patient outcome.
The patient was a 74-year-old man from a village in Zhejiang Province. On June 16, 2014, the patient was admitted to the hospital for fever and cough. He was hospitalized for 25 days and discharged on July 11, 2014. He underwent subtotal gastrectomy and Billroth I anastomosis for perforation of a duodenal ulcer and acute peritonitis since 4 weeks. His sputum and stool were sampled for isolation of bacteria and for antimicrobial susceptibility testing. Carbapenem-resistant isolates were collected and investigated further.
Species identification was performed using the MicroScan WalkAway 40 S1 identification system (Dade Behring, Deerfield, IL). The 16s rDNA sequences were also analyzed to confirm the species identity. Susceptibility of the isolates to antimicrobial therapy was determined using the E-test methodology (BioMerieux SA, La Balme-les-Grottes, France). The modified Hodge test was performed to screen for carbapenemases. These results were interpreted according to the 2014 Clinical and Laboratory Standards Institute recommendations and guidelines. R. planticola isolates from the sputum and stool samples were subjected to pulsed-field gel electrophoresis (PFGE), according to previously reported protocols. 4 The location of blaNDM-1 was determined using the PFGE-S1 nuclease method. Separation of large fragments after restriction enzyme digestion was performed using PFGE, using a Bio-Rad CHEF Mapper XA system (Bio-Rad, CA) with an initial switch time of 2.16 sec and a final switch time of 63.8 sec for a run time of 18 hr. Southern hybridization was performed with a 560-bp segment of the blaNDM-1 gene as a probe, using the Roche digoxigenin labeling and NBT/BCIP coloration system (Roche Biochemicals, Mannheim, Germany). Conjugation experiments were carried out by solid surface methods, with sodium azide-resistant E. coli J53 as the recipient. Transconjugants were selected on Luria-Bertani agar plates containing sodium azide (100 mg/L) and ampicillin (100 mg/L), and then confirmed by PCR amplification of blaNDM-1 for NDM-1-positive donors and blaOXA-30 gene for NDM-1-negative donors.
On admission, the patient was coughing up large amounts of sputum and had high fever. Computed tomography (CT) imaging revealed pulmonary infiltration and pleural effusion in both sides of the chest. The patient was empirically treated with broad-spectrum antibiotics (4,500 mg of piperacillin/tazobactam Q8H) and expectorants before evaluation for pneumonia. Four days later, the results of sputum culture remained positive for R. planticola, which showed intermediate resistance to levofloxacin, but complete resistance to ampicillin, ceftriaxone, ceftazidime, trimethoprim–sulfamethoxazole, and several other antimicrobial agents (Table 1). Based on the clinical manifestations of the patient and the results of laboratory examinations, piperacillin/tazobactam was replaced by 500 mg of levofloxacin QD. After 5 days of treatment, the symptoms had not alleviated and the body temperature of patient was fluctuating. Subsequent samples of stool and sputum continued to show R. planticola isolates that were susceptible to tigecycline. Therefore, 50 mg of tigecycline Q12H was added intravenously (double for the first dose) in combination with levofloxacin. The overall symptoms of the patient improved along with reduced sputum production and normal body temperature 3 days later. After treatment for a week, the neutrophil count of the patient normalized and his C-reactive protein levels decreased. CT imaging revealed significant clearing of the chest, and the patient was eventually discharged with relieved symptoms and a stable body temperature. CT imaging performed 2 weeks after discharge revealed complete absorption and resolution of effusions. 16S rDNA sequence analysis confirmed that the isolated bacteria were R. planticola.
Discussion
To understand the mechanisms of carbapenem resistance, PCR and sequencing assays were performed to identify carbapenemase genes (blaKPC, blaIMP, blaVIM, blaNDM, and blaOXA-48). The blaNDM-1 gene was identified in isolates from sputum and stool samples of the same patient. PFGE analysis of these isolates showed identical gel patterns, suggesting that they were derived from the same strain (Fig. 1A). S1-nuclease PFGE analysis showed that isolates from both the samples contained the same plasmid of ca. 50 kb (Fig. 1B). Furthermore, Southern blot hybridization confirmed that the blaNDM-1 gene was located on this plasmid (Fig. 1C).
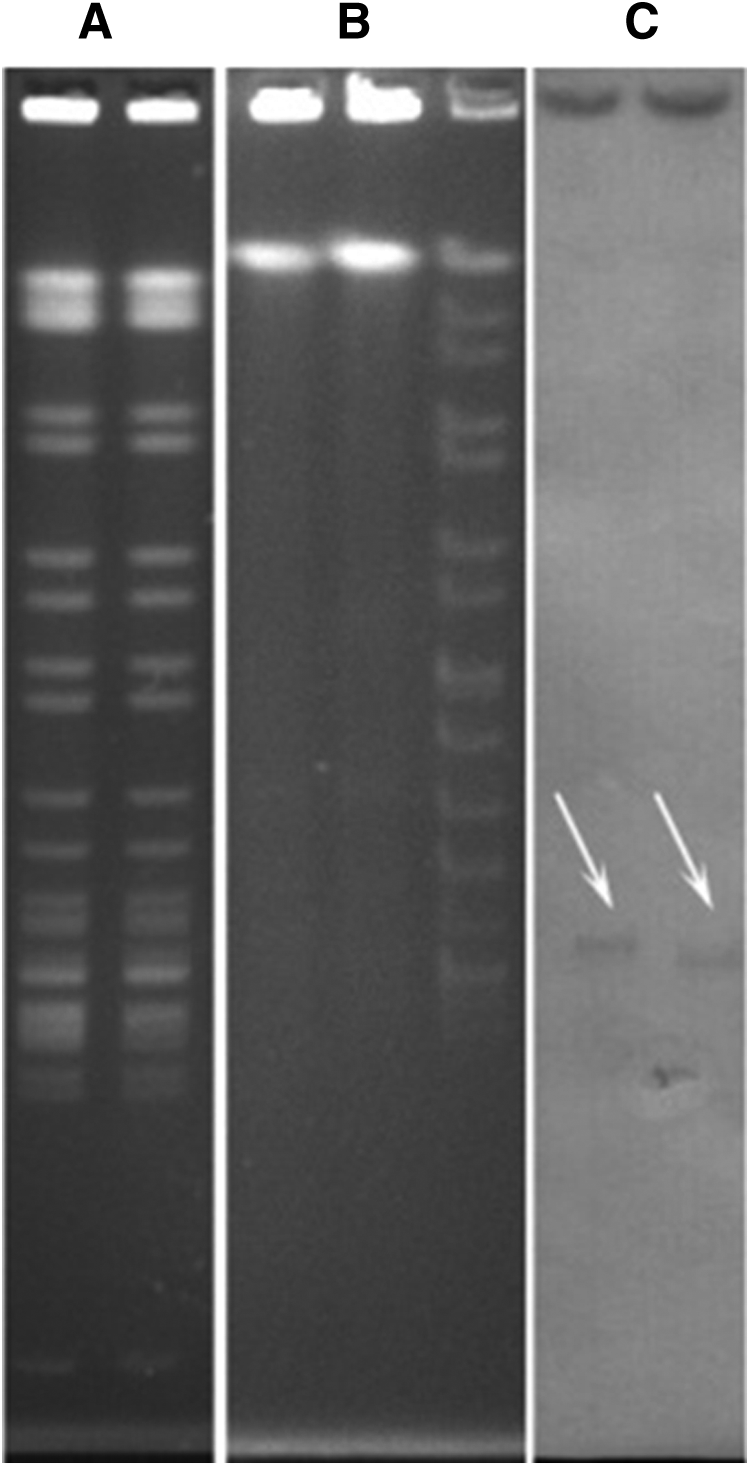
PFGE analysis of Raoultella planticola shows
In this report, we described a case of pneumonia caused by R. planticola in a 74-year-old man with a history of duodenal ulcer perforation and subtotal gastrectomy. The patient eventually recovered after receiving intravenous tigecycline and levofloxacin. After a thorough literature review, we found only 23 cases of R. planticola infections from 1984 to 2015 (Table 2). These included five cases of bacteremia,3,5–8 four cases of cholangitis,9–12 three cases of soft tissue infections,13–15 four cases of pneumonia,4–6,8 two cases of cholecystitis,16,17 three cases of cystitis,18–20 one case of pancreatitis, 21 and one case of conjunctivitis. 22 The ages of patients who developed a clinically relevant R. planticola infection ranged from 30 to 89 years. In addition, we found that patients in a large proportion of the reported cases had a history of recent trauma, namely surgery or invasive procedures (59.1%). Several patients also reported a history of tumors, recent chemotherapy, or immunosuppressive treatment (43.5%).
NA, not available.
In the current case, the elderly patient had a history of gastroduodenal ulcer perforation, gastrectomy, and use of broad-spectrum antimicrobials. This factor may have led to an imbalance of the intestinal flora, which facilitated the emergence of multidrug-resistant bacteria. Laboratory tests showed that both the sputum culture and stool culture were NDM-1 positive for R. planticola, which was confirmed by the PFGE assay. This finding suggested a scenario of possible intestinal colonization of R. planticola in this patient. His pneumonia might be attributed to bacterial translocation or aspiration, accompanied by risk factors such as previous gastrointestinal operation, older age, a feeding tube procedure, or treatment with histamine H-2 antagonists.
To the best of our knowledge, this is the second reported case of blaNDM-1 being detected in R. planticola. The first case was reported in a Klebsiella pneumoniae strain that caused a urinary tract infection in a Swedish patient who had travelled to New Delhi, India, in 2009. 23 The resistance gene NDM-1 can be produced by various pathogens and can be transmitted via a plasmid to other members of the same species or to different bacterial species. The NDM-1 gene has been previously described in E. coli, Enterobacter cloacae, Acinetobacter baumannii, and Citrobacter rodentium across several countries. One study reported that five NDM-1 carbapenemase-producing isolates were identified from 186 carbapenem-resistant Enterobacteriaceae isolates recovered from our hospital between January and September 2013. 24 NDM-1-producing pathogens are resistant to ∼200 kinds of antimicrobial agents. Antimicrobial susceptibility tests indicate that NDM-1 is somewhat sensitive to polymyxin and tigecycline, and that some strains are sensitive to aztreonam, gentamicin, or ciprofloxacin. It has been reported that polymyxin and tigecycline inhibit NDM-1 with ∼80–90% efficiency. 25 Current research and meta-analysis of randomized controlled trials have suggested the use of combination therapy for a curative effect, but the mortality rate is not superior to that observed when monotherapy is used. However, an observational study of carbapenem-resistant Klebsiella pneumoniae indicated that the use of combination therapy appears to be associated with improved survival in bacteremia due to KPC-producing K. pneumoniae. 26 The patient in the current case recovered after receiving a combination therapy of tigecycline and levofloxacin, confirming the results of the susceptibility tests and the effectiveness of combination therapy.
In conclusion, we present a case of blaNDM-1 in R. planticola, which was cured by treatment with tigecycline. R. planticola is a rare and possibly underestimated pathogen in terms of its pathogenicity, and with potential gain of the blaNDM-1 gene, it might produce “superbugs” that can pose a threat to public health. Early detection of this pathogen is, therefore, critical to the selection of effective therapies.
Footnotes
Acknowledgment
This work was supported by a special fund for medical and health program of Zhejiang Province (2010KYB045).
Disclosure Statement
No competing financial interests exist.