
Abstract
In an era of increasing drug resistance and limited numbers of antimicrobials in the drug production pipeline, healthcare-associated infections represent a growing public health threat. When therapeutic options are limited, clinicians often resort to using antimicrobial combinations that produce a synergistic effect on the target pathogen. Novel antibiotics are therefore welcome in the daily practice of medicine. For example, ceftaroline is a broad-spectrum cephalosporin active against a variety of bacteria, including methicillin-resistant Staphylococcus aureus, but with limited activity against enterococci, particularly Enterococcus faecium. In this study, we tested the efficacy of ceftaroline against clinical isolates of gram-positive bacteria (S. aureus, Enterococcus faecalis, and E. faecium) by the broth microdilution and E-test assays, and then evaluated the synergistic effect of ceftaroline and ampicillin using the E-test method. The time-kill assay was used to confirm the data on selected strains. This drug combination has been recently shown to be effective against E. faecalis and could offer the advantage of cost-effectiveness (compared to other synergistic associations) as well as good tolerability. The E-test was chosen because of its relative simplicity of use that makes it suitable for routine clinical laboratories as a quick tool to guide clinicians when confronted with difficult-to-treat infections that may require an empirical approach. Our results indicate the presence of a synergistic effect of ceftaroline and ampicillin on most of the strains used, especially E. faecium and E. faecalis. The fact that two of those Enterococcus strains were vancomycin resistant suggests that the possible use of this combination for combating the spread of vancomycin-resistant enterococci should be explored.
Introduction
A
Recently, the U.S. Food and Drug Administration (FDA) approved the use of ceftaroline, a cephalosporin antibacterial exhibiting a bactericidal activity against many gram-positive and -negative pathogens, for the treatment of acute bacterial skin and skin structure infections, as well as community-acquired bacterial pneumonia. 5 It is active in vitro against gram-positive cocci, including methicillin-resistant S. aureus (MRSA), and some vancomycin-resistant Enterococcus faecalis, but has poor activity against E. faecium. 6
A recent study used the time-kill assay to demonstrate the significant synergistic activity of ceftaroline plus ampicillin on seven strains of E. faecalis. 7 Indeed, the combination of two or more antimicrobial drugs during a treatment regimen is a useful approach to combating MDR infections. Ideally, synergy tests should be performed before starting any combined therapy, however the time-kill or chequerboard assays (the reference methods for studying synergistic activities) are time-consuming and cumbersome, therefore not manageable in a laboratory routine. The result is that synergy tests can be applied only in selected cases.
In this work, we used the E-test gradient diffusion method to evaluate the synergistic activity, on strains of MRSA, E. faecalis, and E. faecium, of a drug combination (ceftaroline and ampicillin) that has already been reported to be effective in vitro against E. faecalis. 7 The relative simplicity of use of the E-test method (compared to the above mentioned time kill or chequerboard assays) makes it a potential candidate for routine use in a diagnostic laboratory, providing the clinician with valuable information when critical decisions are needed.
Materials and Methods
Bacterial isolates
Seventy-seven clinical isolates obtained from patients treated at the “Lazzaro Spallanzani” National Institute for Infectious Diseases in Rome between September 2009 and October 2015 were selected for the study. The strains were grown from various sites: blood (30), wound (17), central venous catheter (CVC) (6), ascitic fluid (4), drainage fluid (5), hepatic fluid (2), pleural fluid (2), abscess (3), rectal swabs (3), synovial fluid (1), cerebrospinal fluid (2), urine (1), and pus (1). The number of isolates for each species was as follows: S. aureus, 30; Staphylococcus haemolyticus, 15; Staphylococcus lugdunensis, 4; E. faecium, 14; E. faecalis, 12; and Corynebacterium striatum, 2. Three of the Enterococcus strains were colonizers obtained from rectal swabs, included because of their vancomycin-resistant phenotype; all the other strains were from clinically relevant infections. Bacteria were identified to the species level using the Vitek 2 (bioMérieux) commercial system. Identification of all isolates was also confirmed by matrix-assisted laser desorption ionization–time of flight (MALDI-TOF) (Bruker Daltonics) analysis.
Antimicrobial susceptibility testing
Susceptibility testing was performed to characterize all strains included in the study, to determine their susceptible or resistant phenotype to aminoglycosides, oxacillin, vancomycin, or daptomycin, using the Vitek 2 system.
The activity of ceftaroline and ampicillin, used separately, was determined by the E-test method (Liofilchem Srl) for both drugs and all strains included in the study, while the broth microdilution assay was used for ceftaroline only.
The E-test minimal inhibitory concentration (MIC) was read on the printed scale at the point where the edge of the inhibition ellipse intercepted the side of the strip, following manufacturer's instructions. MIC results were interpreted according to the EUCAST breakpoint criteria. For S. aureus only, ampicillin MIC values were interpreted according to the Clinical and Laboratory Standards Institute (CLSI) since EUCAST does not provide interpretative criteria for this antibiotic. 8
The broth microdilution assay was performed using in-house 96-well broth microdilution panels according to CLSI guidelines.8,9 For these experiments, ceftaroline was supplied as laboratory-grade powder by Forest Laboratories, Inc. and reconstituted according to manufacturer's instructions. Plates were incubated at 37°C, and MICs were determined following incubation times of 24 hr. A ceftaroline susceptibility breakpoint of ≤1 mg/L has been established by CLSI for S. aureus and was applied in this study. No susceptibility breakpoints have been determined as yet for S. haemolyticus, S. lugdunensis, E. faecium, E. faecalis, and C. striatum.
Synergy testing
E-test assay
An inoculum equal to a 0.5 McFarland turbidity was prepared from each isolate, and 10 μl of the suspension was inoculated onto Mueller-Hinton agar plates. E-test strips were stored at −20°C until use. Determination of MICs by E-test was first performed for the two drugs separately and in duplicate, and the MICs were interpreted at the point of intersection between the inhibition zone and the E-test strip. For synergy testing, the two E-test strips were placed on the same culture plate in a cross formation, so that they intersected each other at their respective MICs with a 90° angle or at the highest concentration present on the E-test strip, when the MIC exceeded this value (e.g., E. faecium > 256 mg/L). The plates were then incubated at 37°C for 24 hr. The resulting MICs for the two drugs were read as previously described. 10 The Fractional Inhibitory Concentration Index (FICI) was calculated on the basis of the resulting zone of inhibition as follows: FICI = FIC A+FIC B, where FIC A is the MIC of the combination/MIC of drug A alone and FIC B is the MIC of the combination/MIC of drug B alone. The FICI was interpreted as follows: synergy: FICI ≤ 0.5; indifference: 0.5 < FICI ≤4; and antagonism: FICI > 4. 11
Time-kill assay
Tubes containing freshly prepared Mueller-Hinton broth supplemented with each drug alone or with the combination of both were inoculated with the selected isolates at a density of ∼106 CFU/ml in a final volume of 5 ml and incubated in a shaking bath at 37°C. Aliquots were removed at times 0, 4, 8, and 24 hr postinoculation and serially diluted in saline for determination of viable counts. A volume of each diluted sample (100 μl) was plated on Mueller-Hinton agar plates and bacterial counts were determined after an 18-hr incubation at 37°C. The antibiotic concentrations used in time-kill assays corresponded to 0.5, 1.0, and 2.0 times the MIC values of each antibiotic alone, as determined by the E-test method. Synergy was interpreted as ≥2 log10 decrease in CFU/ml obtained with the drug combination, compared to its most active component, and ≥2 log10 decrease in the CFU/ml count compared to the initial inoculums, at any time point. The bactericidal activity was defined as a ≥3 log10 CFU/ml reduction in the colony count relative to the initial inoculum. 12
Results
Comparison of ceftaroline MICs by broth microdilution and E-test
The in vitro activity of ceftaroline tested against 25 oxacillin-resistant and 5 oxacillin-susceptible S. aureus strains is shown in Table 1. As expected, ceftaroline demonstrated potent activity against S. aureus strains. We observed 100% and 92% susceptibility in oxacillin-resistant isolates using the E-test and the broth microdilution method, respectively, and 100% susceptibility in oxacillin-susceptible isolates by both methods. Ceftaroline also retained its potency against S. aureus strains with reduced susceptibility to aminoglycosides (data not shown). All the MRSA strains were susceptible to vancomycin and daptomycin (data not shown).
I, intermediate; S, sensitive.
Despite a tendency toward higher ceftaroline MICs by broth microdilution, the majority of differences were within one twofold dilution, which is within the accepted statistical error when comparing different methodologies. There were only 2/25 cases where an isolate was counted as intermediate by broth microdilution, but susceptible by E-test (Table 1, strains 51 and 55).
MIC breakpoints of ceftaroline for S. haemolyticus and S. lugdunensis are not available to date. We noticed a significant number of S. haemolyticus strains with MIC values >1 mg/L (6/15 by broth microdilution and 3/15 by E-test); conversely, ceftaroline was highly active against S. lugdunensis with MICs ≤0.5 mg/L for all isolates tested (Table 2).
Vancomycin-resistant E. faecium isolates.
CVC, central venous catheter.
Concerning enterococci, although there are no recognized susceptibility breakpoints for ceftaroline, we observed MIC50 values of 2 and 0.5 mg/L for E. faecalis by the microdilution and E-test methods, respectively; the MIC50 value observed for E. faecium on the other hand was 128 mg/L for the two methods, therefore considerably higher (Table 2), and this observation confirms the poor activity of ceftaroline against E. faecium. A 100% and 75% concordance between broth microdilution and E-test results was observed for E. faecium and E. faecalis, respectively.
Ceftaroline was also active against C. striatum with MIC values of 1 and 0.3 mg/L determined by broth microdilution and E-test, respectively.
Synergistic combination with ceftaroline
Experiments using the E-test method with ampicillin in combination with ceftaroline showed the presence of synergy in 9 oxacillin-resistant S. aureus (36.0%), 11 E. faecium (78.5%), and 7 E. faecalis (58.3%) strains (Table 3). Remarkably, synergistic effects for the ceftaroline–ampicillin combination were detected also in two vancomycin-resistant isolates (strain 90, E. faecium and strain 37, E. faecalis). No antagonistic interactions were observed.
Synergy: FICI ≤0.5; indifference: 0.5 < FICI ≤4; antagonism: FICI >4.
Presence of synergistic activity.
Vancomycin-resistant E. faecium isolates.
FICI, fractional inhibitory concentration index; MIC, minimal inhibitory concentration; R, resistant.
For three strains of E. faecalis (strains 5013, 4976, and 37) and three of E. faecium (strains 69, 75, and 90), the synergistic action of ampicillin and ceftaroline observed with the E-test was also studied by the time-kill kinetics method and the results are shown in Fig. 1. The presence of synergy was confirmed for all the six isolates tested (Fig. 1A–F), using three different concentrations of the two drugs (0.5 × , 1 × , and 2 × MIC). All three produced a synergistic effect on the strains on which the two antibiotics alone were active at relatively lower MICs (≤16 mg/L) (strains 5013, 4976, and 37). For the strains on which the two antibiotics displayed higher MICs (≥64 mg/L) (strains 69, 75, and 90), synergy was noted at 0.5 × MIC on all three, and at 1 × MIC only on one (strain 90). No effect was produced using the concentration of 2 × MIC on these strains (not shown). The quantitative changes in CFU/ml for synergistic interactions observed at 0.5 × and 1 × MIC are compared in Fig. 1G and 1H, respectively: the sub-MIC concentration proved to be the most effective, with the synergistic effect present after 4 hr of incubation for three strains (5013, 4976, and 69) and after 8 hr for the remaining three (Fig. 1G). At the same concentrations, the two drugs in combination showed bactericidal activity at 8 hr against the E. faecalis strains 4976 and 37, and at 24 hr on E. faecalis 5013. No bactericidal activity against E. faecium strains was noted, although the growth inhibition observed was very close to the established threshold value (Fig. 1D–F).
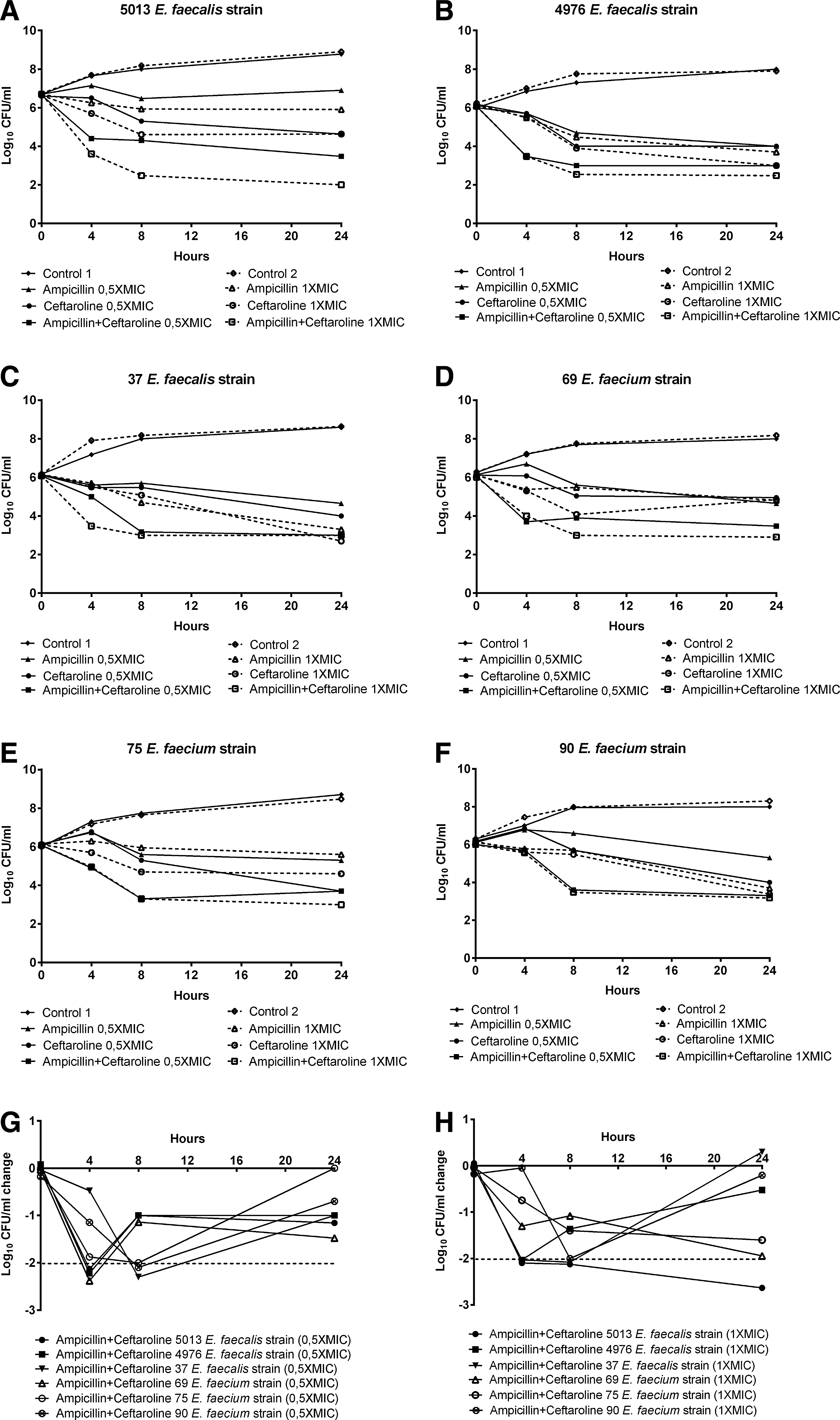
Time-kill kinetics for the ampicillin/ceftaroline combination at 0.5 × MIC (solid line) and 1.0 × MIC (dotted line).
Discussion
Antibiotic resistance is a major public health issue worldwide, affecting gram-positive as well as gram-negative bacteria. Staphylococci and enterococci in particular display continuously evolving resistance, with S. aureus and Enterococcus spp. consistently associated with high mortality rates. 13 In recent years, epidemiological data have highlighted the growing importance of enterococci, and most notably E. faecium, as nosocomial pathogens. 14 Optimal antimicrobial therapy for serious enterococcal infections requires the use of synergistic combinations of a cell wall-active agent such as a penicillin or a glycopeptide together with an aminoglycoside, which results in bactericidal activity against these organisms. Enterococci, however, have acquired aminoglycoside resistance genes that mediate production of aminoglycoside-modifying enzymes, able to counteract the synergistic bactericidal effect. 15 In addition to high-level aminoglycoside resistance, the rapid spread of vancomycin resistance often leaves clinicians with limited therapeutic options. If new and more effective drugs are not available, using a combination of two synergistic antibiotics is often a useful approach when confronted with antibiotic resistance, as is the case with Enterococcal endocarditis. 16
Ceftaroline is a broad-spectrum cephalosporin with bactericidal activity against gram-positive bacteria, including MRSA, vancomycin-intermediate and -resistant S. aureus, Staphylococcus epidermidis (both methicillin sensitive and resistant), and other coagulase-negative staphylococci that often cause opportunistic infections in critically ill patients, such as S. lugdunensis, Staphylococcus hominis, and S. haemolyticus.17–19 In vitro data also suggest that ceftaroline might be effective against vancomycin-resistant E. faecalis, but not E. faecium. 20 To date, literature data are available on the possible synergistic activity of ceftaroline with other antimicrobial agents: some studies reported success in treating MRSA bacteremia using ceftaroline in combination with daptomycin or vancomycin21,22; other studies described the successful use of daptomycin plus ceftaroline in a case of E. faecalis endocarditis.16,23 Recently, the time-kill assay was used to demonstrate that the combination of ampicillin and ceftaroline is synergistic against E. faecalis (the authors did not include E. faecium in their study) and is more active in vitro than ampicillin plus ceftriaxone. 7
In accordance with other studies,17–19 our results show a potent activity of ceftaroline alone against S. aureus, including MRSA strains, and a limited effect on enterococci, E. faecium in particular. Concordance values between 75% and 100% were observed between our broth microdilution and E-test results. Ceftaroline was also active against two strains of C. striatum. Although the significance and prevalence of C. striatum as a causative agent of disease are not well understood, this organism has been implicated in a variety of different infections, 24 and recent data showed its potential for developing resistance to daptomycin both in vivo and in vitro.25–27 As the possible role of C. striatum as an emerging MDR nosocomial pathogen has been suggested, 28 our finding could prompt further studies on the efficacy of ceftaroline also against this organism.
Our synergy test results showed that when used in combination with ampicillin, ceftaroline not only displayed synergistic activity against E. faecalis (58.3% of strains), which is in accordance with other studies, 7 but also against a high percentage of E. faecium (78.5%), showing its maximum effect at a concentration of 0.5 × MIC. This synergistic effect was noted also on a vancomycin-resistant E. faecium. This is to our knowledge the first description of this kind, and although this strain was a colonizer obtained from a rectal swab, and further studies would be necessary to assess the efficacy of ceftaroline in combination with ampicillin for treating VRE infection, we believe that this possibility should be explored.
Our study included 30 strains of S. aureus. Although we were well aware that the ampicillin/ceftaroline combination would not be the first choice to treat this pathogen, especially vancomycin and daptomycin-susceptible strains, in view of the ever-evolving resistance patterns of gram-positive bacteria, we were interested in exploring this approach also on our clinical isolates of MRSA. Synergy was observed in 9/25 strains (36%), and the underlying molecular mechanism could be similar to that proposed for other combinations of beta-lactam antibiotics, which involves the binding of the allosteric site of the Penicillin-Binding Protein 2a (PBP2a). 29
One limitation of this study is that it demonstrates only in vitro efficacy. Considering that the biological free peak concentrations for ceftaroline and ampicillin are 37 and 64 mg/L, respectively, 30 the synergistic activities observed for 5/14 (35.7%) E. faecium strains occur at concentrations that are physiologically unachievable (i.e., 48 to >256 for ceftaroline and 192 to >256 mg/L for ampicillin) for one or both of the drugs tested. The choice of this combination therapy would therefore not be appropriate for these strains; however, for the remaining 9/14 strains of E. faecium and most E. faecalis, this approach could be clinically viable and should be further explored.
The molecular mechanism that could explain the synergistic effect of ampicillin and ceftaroline on enterococci is the saturation effect of the complementary penicillin-binding protein (PBP). Ceftaroline avidly binds PBPs 2, 3, and 5 for which ampicillin has limited or no affinity; ampicillin on the other hand binds PBPs 4 and 5 providing total saturation. These complementary binding profiles lead to more complete inhibition of cell wall synthesis and synergistic killing than these agents alone. 31
The use of ampicillin in combination with ceftaroline appears promising because of its good tolerability and lower costs compared to other drug combinations used to treat troublesome enterococcal infections such as ampicillin and daptomycin.32,33 Although larger studies are needed to assess the cost-effectiveness of different treatment options, our observations suggest that ampicillin and ceftaroline could represent a valid choice for combating bacteria that often pose a challenge to the clinician. Furthermore, even though the E-test may require up to 3 days from subculture to definitive results, 34 it still represents a less resource- and time-consuming alternative to the time-kill or chequerboard methods for performing synergy testing, therefore more suitable for routine laboratories in case of difficult-to-treat, critically ill patients who do not respond to standard therapies.35–37 Clinical and laboratory personnel, however, should always bear in mind that in the absence of a thorough clinical validation of any drug combination, E-test results alone should be interpreted with caution.
Footnotes
Disclosure Statement
No competing financial interests exist.