
Abstract
Fluoroquinolones and ketolides are among the drugs of choice for the treatment of Haemophilus parainfluenzae infections. There has been a report of an emerging fluoroquinolone and telithromycin resistance in H. parainfluenzae isolates from the private sector of KwaZulu-Natal Province of South Africa that necessitates molecular investigation. The aim of this study is to characterize these resistance delineating mutations in genes commonly associated with reduced susceptibility. Ten H. parainfluenzae isolates retrieved from the sputum of 10 patients with H. parainfluenzae pneumonia were subjected to sensitivity testing by the disc diffusion and CLSI broth microdilution methods, polymerase chain reaction (PCR) and DNA sequencing of selected genes associated with resistance were carried out, while repetitive extragenic palindromic PCR (REP-PCR) was used to ascertain clonality. Fluoroquinolone resistance was attributed to the following amino acid substitutions: S84F, D88Y in GyrA, and S84Y/L, S138T, and M198 L change in ParC of the isolates. The plasmid-mediated quinolone resistance gene aac-(6′)-Ib-cr was detected for the first time in four isolates of H. parainfluenzae and D420 N change was observed in ParE in one isolate. Macrolide and ketolide resistance were ascribed to the resistance genes mef (A), msr (D), and erm (B) detected in the isolates. REP-PCR analysis showed that the isolates were not clonal. All the observed resistance mechanisms are first reports in Africa. There is an emerging fluoroquinolone and macrolide resistance in H. parainfluenzae in South Africa that is attributable to known/novel resistance mechanisms, necessitating the monitoring of this pathogen as a potential opportunistic pathogen in a country with a high HIV and AIDS prevalence.
Introduction
H
Although fluoroquinolone and macrolide resistance in H. parainfluenzae are uncommon, it has been increasingly reported globally. 5 The first report of fluoroquinolone resistance in H. parainfluenzae was in Japan in 2003 where a 3.4% resistance to fluoroquinolones was observed in 920 isolates of H. parainfluenzae collected over a period of 3 years from outpatients visiting 382 facilities across the country. 6 A Chinese study conducted from 2006 to 2008 also reported 9–24% resistance to various fluoroquinolones and 5.9–8.8% to various macrolides in H. parainfluenzae isolates collected from AECOPD patients. 1 Interestingly, a 10-year retrospective study in a German hospital reported 1.6% resistance to levofloxacin and no ciprofloxacin resistance in Haemophilus influenzae and H. parainfluenzae isolates implicated in pneumonia. 7
Molecular studies conducted in the United Kingdom (2003), Canada (2010), Spain (2011), Switzerland (2013), and Italy (2015) revealed that the resistance of H. parainfluenzae to fluoroquinolones was mediated by mutations in the quinolone resistance-determining region (QRDR) of DNA gyrase and topoisomerase IV genes.4,5,8–10 Plasmid-mediated quinolone resistance genes and efflux pumps have not been found to play significant roles in fluoroquinolone resistance in H. parainfluenzae isolates studied in Spain and Switzerland.4,5 Our earlier study last year revealed increasing fluoroquinolone and ketolide resistance in H. parainfluenzae but not in H. influenzae in the private sector of KwaZulu-Natal and Gauteng Provinces of South Africa. 11 This study therefore investigates some of the molecular mechanisms underlying the observed fluoroquinolone, macrolide, and ketolide resistance in a selected 10 out of 42 isolates collected over a period of 3 months, delineating mutations in common resistance genes.
Materials and Methods
Ethical considerations
Ethical clearance was received from Biomedical Research Ethics Committee of University of KwaZulu-Natal (BE473/14).
Study design
There has been a report of an emerging fluoroquinolone and telithromycin resistance in H. parainfluenzae isolates from the private sector of KwaZulu-Natal Province of South Africa that necessitates molecular investigation. 11 In response to this report, fluoroquinolone-resistant H. parainfluenzae isolates were collected from one private laboratory in Durban from April to June, 2015, and isolates exhibiting resistance to fluoroquinolones and the ketolide, telithromycin, were subjected to further analysis, specifically minimum inhibitory concentration (MIC) determinations, polymerase chain reaction (PCR), and DNA sequencing of common resistance genes, as well as repetitive extragenic palindromic PCR (REP-PCR) to determine clonality.
Culture, identification, and sensitivity of isolates
From April to June 2015, 42 fluoroquinolone-resistant clinical isolates (ciprofloxacin, levofloxacin, and moxifloxacin) from the sputum of different patients with pneumonia caused by H. parainfluenzae were processed at a private laboratory in EThekwini municipality of KwaZulu-Natal Province, South Africa, which serves different private hospitals. One isolate was retrieved per patient. These were subcultured on chocolate agar plates and incubated at 35–37°C in 5% CO2 for 24 hours. The collected samples were stored in trypticase soy broth with 10% glycerol and 40% horse serum at −85°C. 12 Identification was performed using NH Vitek cards and Vitek MS (Biomerieux, France). Susceptibility to ciprofloxacin, levofloxacin, moxifloxacin, ampicillin, cefuroxime, cefotaxime, meropenem, and telithromycin was performed using the disk diffusion method according to Clinical and Laboratory Standards Institute (CLSI) 2014 guidelines. 13 Nitrocefin test (three to four bacterial colonies were applied to filter paper impregnated with 25 μl of 500 μg/ml nitrocefin and a color change from yellow to red indicated the presence of beta lactamase) was used to detect beta lactamase production. MIC determination for nalidixic acid, ciprofloxacin, gatifloxacin, erythromycin, azithromycin, and telithromycin was carried out on the isolates that exhibited dual resistance to fluoroquinolones and the ketolide, telithromycin (eight isolates), using broth microdilution method according to the CLSI guidelines 13 with H. influenzae ATCC 49247 as reference strain control. In addition, a selected number of isolates that displayed resistance to only fluoroquinolones (ciprofloxacin, levofloxacin, and moxifloxacin) were also included in the analysis for comparison (two isolates). Molecular analysis was carried out on all the selected subsamples to investigate the mechanisms mediating their resistance phenotype.
DNA extraction and PCR amplification
Genomic extraction of an overnight culture of the bacteria was performed using ZR Fungal/Bacterial Miniprep™ (Zymo Research, USA) according to the manufacturer's instructions, while the purity and quantification of genomic DNA were confirmed with the Nanodrop™ 1000 spectrophotometer (Thermo Scientific, USA). Amplification and sequencing of the QRDRs of gyrA, gyrB, parC, and parE genes of H. parainfluenzae isolates were undertaken using T100™ Thermal cycler (Bio-Rad) using primers described elsewhere. 4 Amplification and sequencing of the plasmid-mediated quinolone-resistant genes qnrA, qepA, and aac-(6′)-Ib-cr were carried out using primers reported earlier.14,15 The L4, L22, and 23 s rRNA ribosomal proteins and common macrolide resistance genes erm (B) and mef (A) were also amplified as reported in earlier studies.16,17 The msr (D) gene was amplified using the primers MSRA1: TGCCTATATTCCCCAGTT and MSRA2: TTAATTTCCGCACCGACTA at an annealing temperature of 59°C (M. C. Roberts, University of Washington, Pers. Comm.). The position of the msr (D) in relation to the mef (A) gene was investigated using the MF4AR and ORF5Rev primers reported by Luna et al. 18
PCR was carried out using a 10 μl Phusion Flash High-Fidelity PCR master mix (Thermo Scientific, USA), 2 μl each of forward and reverse primers (10 μM), 50–80 ng of template DNA, and water to 20 μl. The cycle comprised a preliminary denaturation for 10 seconds at 98°C, followed by 35 cycles at 98°C for 1 second, then 54°C for 5 seconds, and 72°C for 15 seconds with a final stage of 72°C for 7 minutes for gyrA and parC genes. The same PCR conditions were used for the other genes, but with the following annealing temperatures: gyrB (58°C), parE (62°C), qnrA (62°C), 14 L22 (56°C), L4 (58°C), 23S rRNA (59°C), 16 qepA (68°C), 15 aac-(6′)-Ib-cr (68°C), and mef (A) (50°C), erm (B) (55°C), 17 and msr (D) (59°C). The PCR products were run on 1.5% agarose gel at 80 V for 1 hour and visualized under ultraviolet light using Bio-Rad ChemiDoc™ MP System (Bio-Rad, USA). The PCR amplicons were purified and sequenced by Inqaba Biotec™ South Africa, using Sanger dideoxy sequencing technology. Inspection of the chromatograms sequencing files was carried out using Chromas 2.4.3 (Technelysium). The sequences of both strands were aligned for comparison with the complete genome of the fluoroquinolone-susceptible isolate H. parainfluenzae T3T1 (accession no. FQ312002.1) and macrolide-susceptible H. influenzae Rd (accession no. NC_000907.1), or homologies were searched for in the National Center for Biotechnology Information (NCBI; National Institutes of Health) BLAST (Basic Local Alignment Search Tool) 2.2.31 server on GenBank database, release 209.0 (http://blast.ncbi.nlm.nih.gov/Blast.cgi), last accessed on 27th November, 2015.
Nucleotide sequence accession numbers
The nucleotide sequences reported in this article were submitted to GenBank and the following accession numbers were assigned: KT819624 (gyrA), KT873306 (gyrB), KT819625 and KT827740 (parC), KT827741 and KT873307 (parE), KT819626 [mef (A)], KT819627 [Aac-(6′)-Ib-cr], KT819628 [erm (B)], KT873308 (L4), KT873309 (L22), and KU180707 [msr (D)].
REP-PCR genomic profiling
Each 50 μl PCR mixture contained 1 μM each of the forward and reverse primers (REP1R-Dt and REP2-Dt), 5 200 μM of each dNTP (Thermo Scientific), 2.5 U of Supertherm polymerase (Separation Scientific), 1× reaction buffer, and 100–200 ng of template DNA. The PCR conditions comprised 7 minutes at 94°C followed by 32 cycles of 1 minute at 94°C, 1 minute at 40°C, and 8 minutes at 72°C with a final elongation of 16 minutes at 72°C. A negative control containing all reagents, except target DNA, was included with each batch. The PCR products were run on a 1.6% agarose gel (Seakem) in the TBE buffer. 19 Images were captured with the Bio-Rad ChemiDoc MP System (Bio-Rad) and analyzed with the BioNumerics software (Applied Maths). The Dice coefficient and unweighted pair group method with average linkages was used to generate the dendrogram with 1.0% tolerance and 0% optimization values.
Results
Susceptibility data of isolates
Forty-two fluoroquinolone-resistant H. parainfluenzae isolates were recovered from 42 patients with H. parainfluenzae pneumonia from different private hospitals at the private laboratory within the 3-month study period. All the 42 isolates were found to be susceptible to ampicillin, cefuroxime, cefotaxime, and meropenem according to the CLSI breakpoints for disc diffusion.
13
All the isolates also exhibited resistance to ciprofloxacin, levofloxacin, and moxifloxacin. Eight isolates (RK 21, RK 24, RK 25, RK 29, RK 33, RK 39, RK 40, and RK 41) were found resistant to both fluoroquinolones and the ketolide, telithromycin. These isolates were then subjected to MIC determinations and further molecular analysis. Two isolates (RK 26 and RK 34) from the remaining 34 isolates (resistant to only the fluoroquinolones) were included in the further analysis for comparison. None of the isolates was a beta lactamase producer when tested using nitrocefin. The susceptibility results by disc diffusion are displayed in Table 1, while
AMP, ampicillin; CXM, cefuroxime; CTX, cefotaxime; CIP, ciprofloxacin; LEV, levofloxacin; MOX, moxifloxacin; AMO-CLAV, amoxicillin–clavulanate; MEM, meropenem; TEL, telithromycin; S, susceptible; R, resistance.
All isolates were recovered from the sputum of patients with H. parainfluenzae pneumonia.
The Ala69Ser substitution was observed after comparison with Haemophilus influenzae Rd, but not with Haemophilus parainfluenzae T3T1.
NAL, nalidixic acid; GAT, gatifloxacin; ERY, erythromycin; AZM, azithromycin; PMQR, plasmid-mediated quinolone resistance gene; QRDR, quinolone resistance-determining regions; NC, no change; aac-(6), aac-(6′)-Ib-cr; NA, not ascertained; MIC, minimum inhibitory concentration.
Molecular analysis of the isolates
The following amino acid substitutions were found: S84F and D88Y in GyrA, S84Y, S138T, M198 L, and S84 L change in ParC, and D420 N in ParE. The plasmid-mediated quinolone resistance gene aac-(6′)-Ib-cr was detected for the first time in four isolates of H. parainfluenzae. Macrolide, azalides, and ketolide resistance genes, mef (A) and the msr (D) and erm (B) genes, as well as A69S substitution in L4 ribosomal protein were detected in the isolates. REP-PCR analysis showed that the isolates are not clonal. The results are summarized in Table 2. REP-PCR results are shown in Fig. 1.
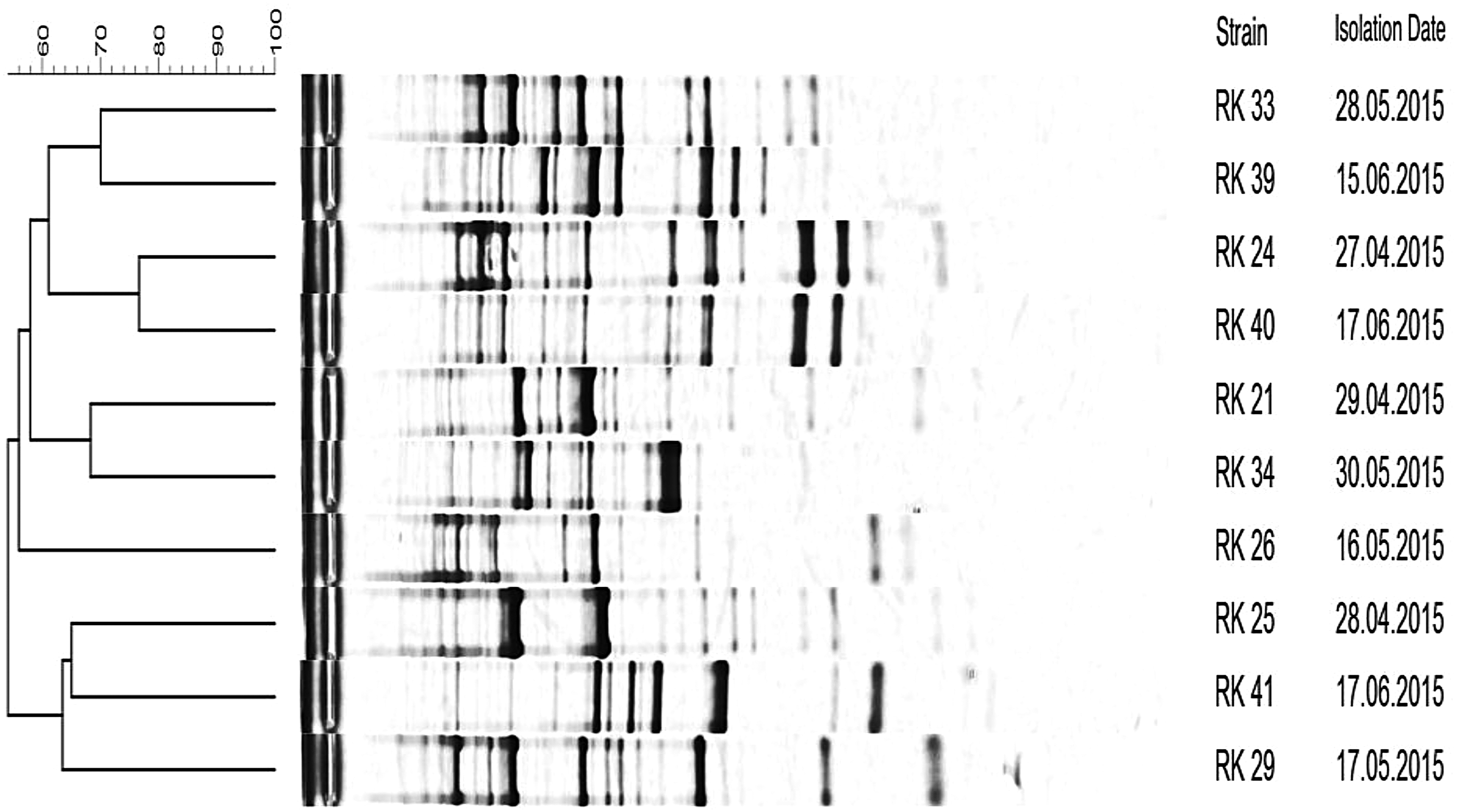
DNA fingerprints generated by REP-PCR amplification from 10 isolates of Haemophilus parainfluenzae. The dendrogram was constructed using the Bionumerics Fingerprint Analyst Software (Applied Maths). The degree of similarity (%) is shown on the scale. REP-PCR, repetitive extragenic palindromic polymerase chain reaction.
Discussion
Fluoroquinolone resistance mechanisms
As shown in Table 2, amino acid substitutions S84F and D88Y were detected in the topoisomerase II subunit A (GyrA) and S84Y, S84 L, S138T, and M198 L in topoisomerase IV subunit A (ParC) of the isolates. These amino acid substitutions, S84F, D88Y in GyrA, and S84F/L, S138T, and M198 L in ParC of H. parainfluenzae have been observed in earlier studies.4,5,8,10,20
Mutations at position 84 and 88 of GyrA and ParC have been shown to decrease fluoroquinolone binding to the enzyme-DNA complexes, thereby increasing the MICs of these antibiotics. High-level fluoroquinolone resistance is associated with mutations in both GyrA and ParC in most species of bacteria. Sequential mutations in these two drug targets have been shown to cause a corresponding increase in resistance levels. 21 These specific mutations at position 84 and 88 of GyrA and ParC have been observed in our study, which may explain the high fluoroquinolone MICs. These findings can also explain the susceptibility profile of isolate RK 33, which had only two mutations in ParC with consequently lower fluoroquinolone MICs than all the other isolates. Furthermore, the amino acid leucine replaced serine at position 84 of the ParC of isolate RK 33, while the rest of the isolates had tyrosine substituting serine. Substitution of serine by leucine might not have decreased the fluoroquinolone binding ability to the DNA-enzyme complex to the degree that tyrosine substitution might achieve. This postulated inability may also explain the slightly lower MICs observed with isolate RK 33. It will be interesting to establish the association between the novel S84 L substitution in ParC and fluoroquinolone resistance by site-directed mutagenesis.
The only report of fluoroquinolone resistance in H. parainfluenzae in South Africa including molecular analysis was of a single case study of one isolate collected from the Pretoria Academic Hospital in 2003. The study revealed substitutions in GyrA (S84 L) and no mutations in GyrB, ParC, and ParE. 9 The S84F substitution in GyrA and all the mutations in ParC protein found in our study are therefore the first to be reported in H. parainfluenzae in South Africa and indeed Africa. It is possible that the pathogen is progressively acquiring new mutations to resist the action of fluoroquinolones. The continuation of this trend may result in the ineffectiveness of fluoroquinolones in empirical treatment of AECOPD and other infections caused by H. parainfluenzae.
Mutations in the GyrB of the isolates were not detected, this observation being consistent with earlier studies.4,9 Investigations by Rodriguez-Martinez et al., in 2012, revealed D420 N and A451S amino acid substitution in the QRDR of ParE in fluoroquinolone resistance in H. parainfluenzae. 4 While D420 N mutation was detected in one isolate (RK 39) in our study, the A451S change was not observed; this D420 N mutation in ParE is also the first report in Africa. It has been suggested that mutations in QRDR of GyrB and ParE genes also result in a reduced affinity of fluoroquinolones to the enzyme-DNA complex, thereby increasing the MICs. 21 This must, however, be investigated.
The plasmid-mediated quinolone resistance genes qnrA and qepA were not present in any of the isolates, nonetheless; fluoroquinolone acetylating aminoglycoside acetyltransferase [aac-(6′)-Ib-cr] was detected in isolates RK 29, RK 39, RK 40, and RK 41. Although this gene was found in H. influenzae and H. parasuis to cause a low-level quinolone resistance leading to the selection of DNA gyrase and topoisomerase IV mutants,22,23 it has not been reported in the H. parainfluenzae species. The aac-(6′)-Ib-cr gene has been shown to be plasmid borne and acetylates ciprofloxacin at the amino nitrogen on its piperazinyl substituent. 24 It is originally an aminoglycoside-acetylating enzyme; however, W102R and D179Y substitutions confer quinolone-acetylating activity on the enzyme. 21 The aac-(6′)-Ib-cr genes found in our study possess these two mutations and are therefore implicated in the observed fluoroquinolone resistance. The presence of this gene in H. parainfluenzae raises the possibility of the bacterium acting as a reservoir of this plasmid for the transfer into H. influenzae, as occurs now with TEM beta-lactamases. 2
Macrolides and ketolide resistance mechanisms
Resistance to the macrolide and ketolides is mediated by similar mechanisms, namely, alterations in the 23S rRNA, L4 and L22 proteins, erm genes that code for methylases, and mef and msr efflux mechanisms,8,25 all of which were investigated in our study. All the 10 isolates exhibited A69S substitution in the L4 proteins when compared with macrolide- and ketolide-susceptible H. influenzae Rd L4 protein. A69S substitution has also been reported in H. influenzae 16 and H. parainfluenzae. 7 This substitution was not observed when the sequences were compared with the reference strain H. parainfluenzae T3T1. This mutation was also detected in the susceptible strains (RK 26 and RK 34), which may suggest that it is not involved in macrolide–ketolide resistance. It is therefore probable that the serine at this position is a signature of the H. parainfluenzae species rather than a mutation. No mutations were detected in the 23S rRNA and L22 ribosomal proteins of any of the isolates.
The mef- (A), msr- (D), and erm- (B) acquired resistance genes may be the major contributors to telithromycin resistance as the isolates without these genes exhibited MICs of less than 64 mg/L. mef (A) gene encodes a macrolide efflux pump belonging to the major facilitator superfamily 3 and was detected in isolates RK 24 and RK 40. The detection of this efflux pump in H. parainfluenzae was reported previously in Switzerland. 5 The msr (D) gene encodes a macrolide and ketolide efflux pump that belongs to the ATP binding cassette superfamily. It usually coexists with the mef (A) gene on a transposon. 26 It was present in isolates in our study and was located downstream of the mef (A) gene as the open reading frame 5 of Tn1207.3 (accession no. AF227521), an observation consistent with other published works. 17
erm (B) gene was identified in isolate RK 33, the first report of this in H. parainfluenzae. This gene has been found to code for rRNA methylase that adds a methyl group to a single adenine in the 23S rRNA moiety. This methylation confers broad-spectrum resistance to macrolides, lincosamides, and streptogramin B antibiotics (MLSB), 26 as is evident in the high MICs of erythromycin and azithromycin observed with the isolate RK 33. The erm (B)-containing isolate RK 33 expressed high-level resistance to telithromycin which may not be entirely due to erm (B) gene. This is because the presence of an aryl group in telithromycin enhances its affinity for ribosomes, including those methylated by the erm (B) gene, and a consequently lower MIC. Hence, additional mechanisms may have contributed to the high MIC observed. erm (B) and mef (A) were previously identified in H. influenzae and H. parainfluenzae and can serve as reservoir to harbor and transfer these genes to H. influenzae. 27
As the isolates were collected within a period of 3 months from the EThekwini Municipality; REP-PCR was conducted to determine if they were genetically related. Results of the REP-PCR analysis (Fig. 1) revealed that the isolates were not identical, the highest similarity being 80% for isolates RK 40 and RK 24. This can be rationalized as the macrolide MICs for these isolates were identical, both possessing the mef (A) and msr (D) genes, and possibly the entire transposon. These isolates were recovered from two male patients from the same medical ward, but the 2-month difference in the isolation dates precludes patient-to-patient transfer. Further studies involving pulse-field gel electrophoresis or whole-genome sequencing are needed to confirm that the isolates are unrelated.
Conclusion
There is an emerging fluoroquinolone, macrolide, and ketolide resistance in H. parainfluenzae in South Africa. The fluoroquinolone resistance is mediated by amino acid substitutions S84F, D88Y in GyrA, and S84Y/L, S138T, and M198 L change in ParC, as well as the plasmid-mediated quinolone resistance gene aac-(6′)-Ib-cr in the isolates similar to other species. The role of the mutation D420 N in ParE remains unknown. Macrolide efflux pump genes mef (A), msr (D), and erm (B) mediated macrolide and ketolide resistance in the isolates. There is therefore the urgent need to monitor fluoroquinolone, macrolide, and ketolide resistance in H. parainfluenzae in South Africa to inform the empiric treatment of infections caused by H. parainfluenzae.
Footnotes
Acknowledgments
The authors are grateful to Lancet Laboratories, Durban, for providing retrospective data and isolates. Special thanks goes to Dr. Linda Bester of Biomedical Research Unit of UKZN Westville Campus, South Africa, for use of her laboratory for MIC determinations. This work was supported by the Mwalimu Nyerere African Union Scholarship Scheme, Addis Ababa, Ethiopia, and the College of Health Sciences of the University of Kwazulu-Natal, Durban, South Africa. None of the funders was involved in the study design, data collection, and analysis, decision to publish, or preparation of the article.
Disclosure Statement
Professor Essack is a member of the Global Respiratory Infection Partnership (GRIP) sponsored by Reckitt and Benckiser. All other authors have none to declare.