
Abstract
Treatment of Acinetobacter baumannii has become a medical challenge because of the increasing incidence of multiresistant strains and a lack of viable treatment alternatives. This systematic review attempts to investigate the changes in resistance of A. baumannii to different classes of antibiotics in Iran, with emphasis on the antimicrobial activity of polymyxin B (PMB) and colistin (COL). Biomedical databases were searched for English-published articles evaluating microbiological activity of various antimicrobial agents, including PMB and COL. Then, the available data were extracted and analyzed. Thirty-one studies, published from 2009 to 2015, were identified which contain data for 3,018 A. baumannii clinical isolates. With the exception of polymyxins and tigecycline (TIG), there was a high rate of resistance to various groups of antibiotics, including carbapenems. The minimum inhibitory concentration (MIC) ranges for PMB and COL on A. baumannii isolates tested were 0.12–64 μg/ml and 0.001–128 μg/ml, respectively. Polymyxins showed adequate activity with no significant trends in the resistance rate during most of the study period. The incidence of resistance to TIG was estimated low from 2% to 38.4% among the majority of A. baumannii. The present systematic review of the published literatures revealed that multidrug-resistant (including carbapenem-resistant) strains of A. baumannii have increased in Iran. In these circumstances, the older antibiotics, such as COL or PMB, preferably in combination with other antimicrobials (rifampicin, meropenem), could be considered as the therapeutic solution against the healthcare-associated infections. Designing rational dosage regimens for patients to maximize the antimicrobial activity and minimize the emergence and prevalence of resistance is recommended.
Introduction
U
Currently, infections caused by A. baumannii have become difficult to manage. It is mainly due to the increasing number of strains exhibiting resistance to virtually all major classes of antibacterial agents. In the past years, multidrug-resistant A. baumannii (MDR-AB) isolates, which are defined as nonsusceptible to at least one agent in three or more antibiotic categories, have been distributed globally.5–8 In addition, extensively drug resistant (XDR) isolates that are nonsusceptible to at least one agent in all but two or fewer antibiotic categories, including carbapenems, are continually reported from different countries, including Iran.6,9–11
In these circumstances, polymyxins (colistin [COL] and polymyxin B [PMB]) and tigecycline (TIG) (the 9-t-butylglycylamido derivative of minocycline) remain as the major active antibacterial agents for treatment of life-threatening infections caused by MDR or XDR A. baumannii.12–14 Despite TIG being approved by US Food and Drug Administration (FDA) for complicated intra-abdominal and complicated skin and skin structure infections, a meta-analysis showed that this antibiotic was not better than the currently used antimicrobials. 15 In addition, FDA warnings about increased mortality associated with the drug have led physicians to recede from using it except in very limited conditions. 16 Consequently, many physicians have been forced to turn to polymyxins, the old drugs that were used clinically until around the year 1980, for treatment of widespread MDR bacilli. 17
Despite being yet considered to be rare, there are current reports on the clinical outcome of patients affected by infections arising from pandrug-resistant (PDR) A. baumannii. These suggest that the mortality rate is high because of the fact that the isolates were resistant to all classes of antibiotics used, including polymyxins.6,18–20 This situation gives emphasis to continuous regional evaluation of, and monitoring the antimicrobial susceptibility, and determining the changing trend in A. baumannii populations to provide helpful information to clinicians for better decision-making and better patient outcomes. In this regard, the present review was performed in a comprehensive manner to identify and evaluate the available data on in vitro antimicrobial activity of polymyxins (PMB and COL), as well as other classes of antibiotics, against A. baumannii isolates from Iranian patients. Specifically, we aimed to identify the resistance trends of isolates toward polymyxins during the study period.
Polymyxins
Polymyxins belong to a class of antibiotics that were discovered in 1947. They are decapeptide antibiotics consisting of chemically different compounds (polymyxins A-E), of which PMB and polymyxin E (also known as COL) have been used in clinical practice.21–23 Polymyxins have been used for decades in topical formulations for eye and ear infections and also in intravenous formulations to prevent and treat patients with respiratory tract infections. However, these antibacterial agents were gradually abandoned in most parts of the world around the year 1980 because of the reports of serious toxic effects, mainly to the kidney and nervous system.17,24
Due to the growing epidemic of infections caused by MDR Gram-negative bacteria, such as A. baumannii, Klebsiella pneumoniae, and Pseudomonas aeruginosa, the use of intravenous polymyxins has resumed in several parts of the world. Actually, when the use of β-lactam, aminoglycoside, or fluoroquinolone is ineffective, the polymyxins, especially COL, serve as the final alternative treatment. 25
Polymyxins are secondary metabolite nonribosomal peptides produced by the soil bacteria, Paenibacillus polymyxa, which were formerly classified as Bacillus polymyxa. 23 Chemically, they are cationic cyclic decapeptides linked to a fatty acid chain through an α-amide linkage. 22 Both PMB and COL are rapid-acting bactericidal agents, with a detergent-like mechanism of action.23,24 Polymyxins bind to lipopolysaccharide (LPS) and phospholipid molecules in the outer membrane of Gram-negative bacteria, leading to permeability changes in the cell envelope, leakage of intracellular contents, and cell death. 25
Polymyxins have no activity against Gram-positive and anaerobic bacteria, but are active against most Gram-negative bacilli, including most clinically relevant Enterobacteriaceae and nonfermentative species.23,24 Among Enterobacteriaceae, Citrobacter spp., Enterobacter spp., Escherichia coli, Klebsiella spp., Salmonella spp., and Shigella spp., are usually susceptible.26,27 Acinetobacter spp. and P. aeruginosa are naturally susceptible to both PMB and COL.26,28,29 Stenotrophomonas maltophilia is usually susceptible, although some strains are resistant. 27 Previous studies have demonstrated that polymyxins are also active against Bordetella pertussis, Hemophilus influenzae, and Legionella pneumophila.30,31
Materials and Methods
Data sources
Biomedical databases, including Web of Science, PubMed, Scopus, Elton Bryson Stephens Company (EBSCO), Scientific Information Database (SID), and IranMedex, were searched for articles that evaluated the in vitro activity of antibacterial agents against A. baumannii isolates. It is noteworthy that in this review, the studies were chosen in which polymyxins were necessarily used for evaluation of isolates. The following key words were used: “Acinetobacter baumannii AND antimicrobial resistance AND Iran,” “multidrug resistant Acinetobacter baumannii AND Iran,” “extensively drug resistant Acinetobacter baumannii AND Iran,” and “pandrug resistant Acinetobacter baumannii AND Iran.” References of all included articles were reviewed to find more eligible articles. In general, any article providing data on the susceptibility of A. baumannii to the polymyxins along with other antimicrobials was selected to be used in this review.
Data extraction
Thirty-one English published studies were identified to be eligible for inclusion in this review. All included articles contained data on the in vitro susceptibility of antimicrobials, including PMB and COL to A. baumannii with clinically significant resistance (MDR, XDR, and PDR) in Iran. For each study, data were extracted in terms of publication year, study geographic location, study design, isolate number, anatomical sites of isolation, species identification methods, antimicrobial susceptibility testing methods, and resistance characteristics of isolates to antibiotics tested. In addition, reported MICs of both PMB and COL on isolates from relevant studies were extracted.
Statistics
Descriptive statistics and chi-square test were used by SPSS software version 18 (SPSS, Inc., Chicago, IL) to evaluate the changing trend of drug resistance over the time course of this study. A p-value <0.05 was defined as statistically significant.
Results
Characteristics of selected studies
The main characteristics of 31 selected articles are presented in Table 1. Articles were published from July 2009 to November to December 2015. Geographically, selected studies were conducted in the capital (16 times), west (2 times), south (1 study), south-west (6 times), north-west (1 study), north-east (1 study), central (2 times), capital and south (1 study), and capital, center, and south (1 study) of Iran (Fig. 1).
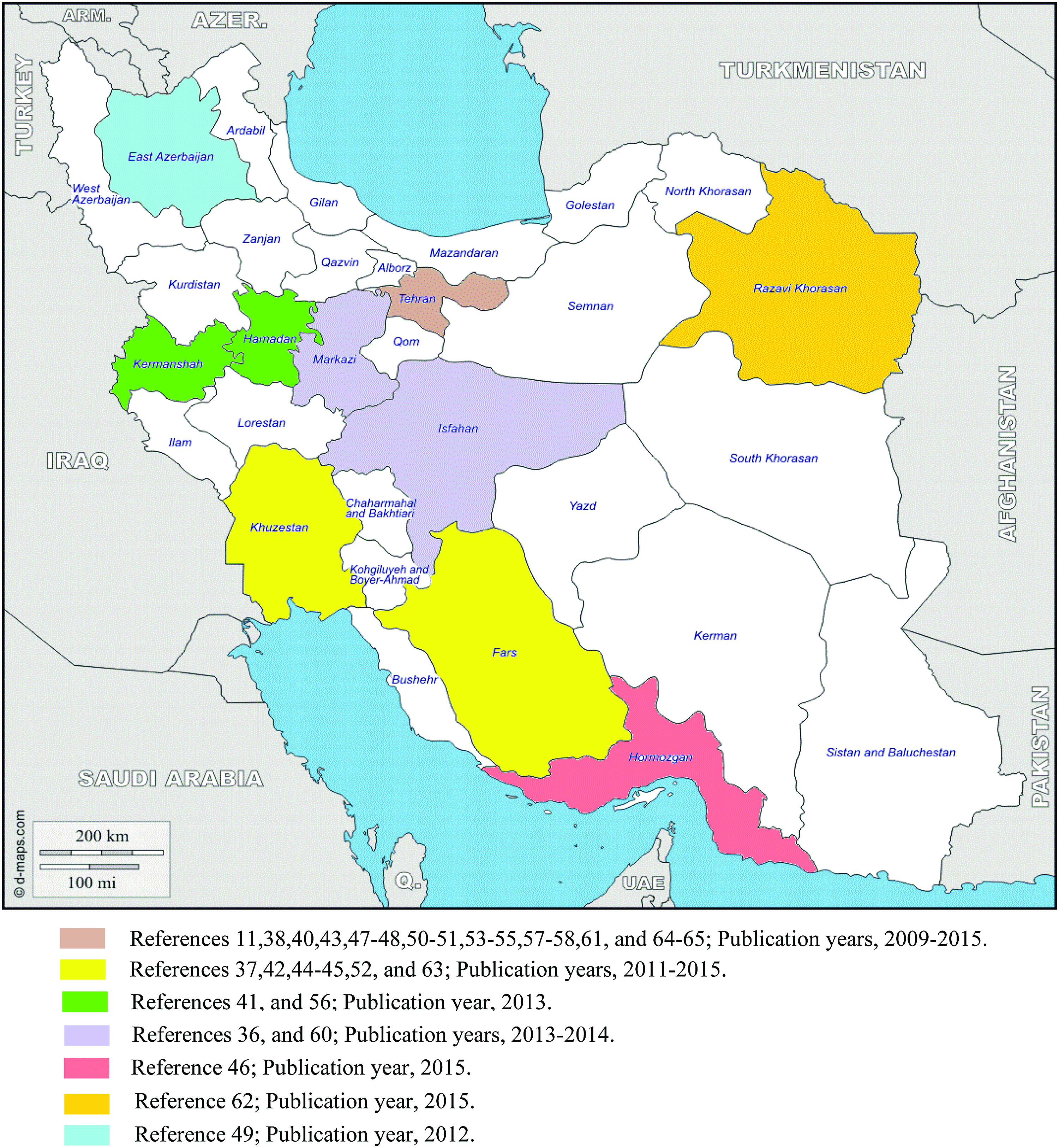
Geographical distribution of selected studies on the A. baumannii antimicrobial resistance in Iran. Geographical location of two multicenter studies, Bahador et al. 39 (publication year, 2013) and Najar Peerayeh et al. 59 (publication year, 2014), that were conducted in north, capital, and south and capital, and south, respectively, are not shown. Color images available online at www.liebertpub.com/mdr
The MIC values were determined by microbroth dilution method.
The MIC values were determined by E-test method.
The IMP and MEM susceptibility of isolates evaluated by E-test method.
The RIF susceptibility evaluated by E-test method from 45 of 70 A. baumannii isolates.
The COL susceptibility evaluated by E-test method from 30 of 70 A. baumannii isolates.
Results obtained from 154 of 157 A. baumannii isolates.
BAL, bronchoalveolar lavage; BSAC, British Society for Antimicrobial Chemotherapy; COL, colistin; CSF, cerebrospinal fluid; ESBL, extended-spectrum β-lactamase; EUCAST, European Committee on Antimicrobial Susceptibility Testing; FDA, Food and Drug Administration; IMP, imipenem; MBL, metalo-β-lactamase; MDR, multidrug resistant; MEM, meropenem; MIC, minimum inhibitory concentration; ND, nondetermined; PDR, pandrug resistant; PMB, polymyxin B; RIF, rifampicin; TIG, tigecycline; XDR, extensively drug resistant.
Twenty-six, six, and four studies used disk agar diffusion, broth dilution, and E-test methods for antimicrobial susceptibility testing on A. baumannii, respectively. Disk agar diffusion was used in several studies in combination with either E-test (six times) or broth dilution (five times) method. Microbiological methods used for the evaluation of the Acinetobacter susceptibility were performed according to Clinical and Laboratory Standards Institute (CLSI) guidelines. 32 It is noteworthy that since no interpretive criteria have been approved for TIG and rifampicin (RIF) against Acinetobacter species, selected studies used the following adopted criteria: the US FDA breakpoints for Enterobacteriaceae (S: ≥19 mm, ≤2 μg/ml; I: 15–18 mm, 4 μg/ml; R: ≤14 mm, ≥8 μg/ml), 16 the European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoints for Enterobacteriaceae (S: ≥18 mm, ≤1 μg/ml; I: 15–17 mm, 2 μg/ml; R: <15 mm, >2 μg/ml), 33 the British Society for Antimicrobial Chemotherapy (BSAC) breakpoints for member of Enterobacteriaceae (S: ≥24 mm, ≤1 μg/ml; I: 20–23 mm, 2 μg/ml; R: ≤19 mm, >2 μg/ml) 34 or the Jones et al. criteria for Acinetobacter species (S: ≥16 mm, ≤2 μg/ml; I: 13–15 mm, 4 μg/ml; R: ≤12 mm, ≥8 μg/ml) for TIG, 35 and CLSI criteria using breakpoint suggested for Staphylococcus aureus (S: ≥20 mm, ≤1 μg/ml; I: 17–19 mm, 2 μg/ml; R: ≤16 mm, ≥4 μg/ml), 32 and EUCAST criteria for Staphylococcus spp. (S: ≥26 mm, ≤0.06 μg/ml; I: 23–25 mm, 0.125–0.25 μg/ml; R: <23 mm, >0.5 μg/ml) 32 for RIF.
Clinical samples and bacterial identification
A total of 3,018 A. baumannii clinical isolates were identified by the 31 selected studies conducted within the 8 years from the beginning of 2006 to early part of the year 2014. The isolates were recovered from patients admitted to distinct wards of Iranian teaching hospitals. The origin of isolates was various clinical specimens, such as blood, urine, burn wound, sputum, bronchial washing, cerebrospinal fluid (CSF), tracheal aspirate, ascites fluid, abscess drainage, pleural effusion, and catheter. In one study, isolates were collected from hospital sources, including ventilator tubing, suction catheter, patient's mattress, and barometer. 36
Some studies identified A. baumannii isolates using phenotypic methods, including conventional bacteriological and biochemical tests, API 20NE system, and Microgen kits. Others used polymerase chain reaction technique for blaOXA-51-like genes, gyrB gene, or 16S-23S ribosomal internal spacer (ITS) region to confirm the phenotypic characterization of A. baumannii.
Antimicrobial susceptibility of A. baumannii
With the exception of one study, 37 30 included studies assessed susceptibility patterns of A. baumannii isolates to different antibiotics. In general, data reported from these studies indicate that, with the exception of polymyxins and TIG, there was high rate of resistance to different classes of antibiotics, such as penicillins (ampicillin, piperacillin, mezlocillin, ticarcillin, and carbenicillin), penicillins/β-lactamase inhibitors (ampicillin/sulbactam, amoxicillin/clavulanic acid, piperacillin/tazobactam, and ticarcillin/clavulanic acid), cephalosporins (ceftazidime, cefotaxime, ceftriaxone, and cefepime), carbapenems (imipenem [IMP], meropenem [MEM], and doripenem), monobactams (aztreonam), aminoglycosides (gentamicin, amikacin, and tobramycin), fluoroquinolones (ciprofloxacin and ofloxacin), tetracyclines, trimethoprim/sulfamethoxazole, and RIF.
Susceptibility of A. baumannii to RIF
Regarding the susceptibility data on the RIF, as an agent with bactericidal activity against MDR-AB, it should be noted that seven studies reported 63–98.1% of a resistance rate among the 731 isolates tested.38–44 In one study, 39 all IMP- and COL-resistant A. baumannii isolates showed resistance to RIF (MIC, 2–64 μg/ml, MIC90, 16 μg/ml). Another study revealed a 24% increase in resistance rate of isolates with a rising trend of higher MIC ranges to RIF between 2006 and 2011 (70% vs. 94%, MIC, 0.1–60 μg/ml vs. 0.1–120 μg/ml). 38
Susceptibility of A. baumannii to carbapenems
There are 29 studies reporting data on the frequency of resistance to carbapenems among the A. baumannii isolates. Three studies reported low rates of resistance: 22.8% and 27.8% to the IMP and MEM, respectively, 45 and both the 29.8% and 30.4% against IMP.46,47 In an additional study, 38 30% of the isolates recovered in the year 2006 were resistant to IMP, while the percentage of resistance was increased to 48% in the year 2011. Furthermore, 25 remaining studies determined resistance rate as follows: (1) relatively high, ranging from 52.2% to 69.9% and 52.5% to 69% against IMP and MEM, respectively,11,39–40,48–54 and (2) high from 75% to 100% and 70.2% to 100% against IMP and MEM, respectively.11,36,39,41–44,46,50–64 Susceptibility to doripenem, a newer carbapenem, was evaluated by two studies in which 92% and 94% of corresponding isolates were resistant.40,44
Susceptibility of A. baumannii to the polymyxins
Of the 31 studies reviewed, 14, 4, and 13 studies reported data on susceptibility of A. baumannii isolates to the COL, PMB, and both COL and PMB, respectively. The resistance rate to polymyxins reported by the most relevant studies was low, ranging from 0% to 19% to COL11,36–47,49,50,52,53,55,56,58–63,65 and 0% to 16% to PMB.11,39,41,42,44,46,48–54,59,63,65
Figure 2 shows the trends of weighed mean resistance rates of A. baumannii to COL and PMB over the 8 years between 2006 and 2014. The mean resistance rate to both antibiotics during the years 2008 and 2012 shows a significant difference compared with the other years (p < 0.001). The mean percentages of resistance were as follows: 0% in 2006, 1.3% in 2007, 19% in 2008, 0% in 2009, 1.74% in 2010, 5.3% in 2011, 9.54% in 2012, and 2% in 2013 to COL, and 8.8% in 2006, 16% in 2008, 0% in 2009, 4.94% in 2010, 0.94% in 2011, 11.6% in 2012, and 0% in 2013 to PMB.
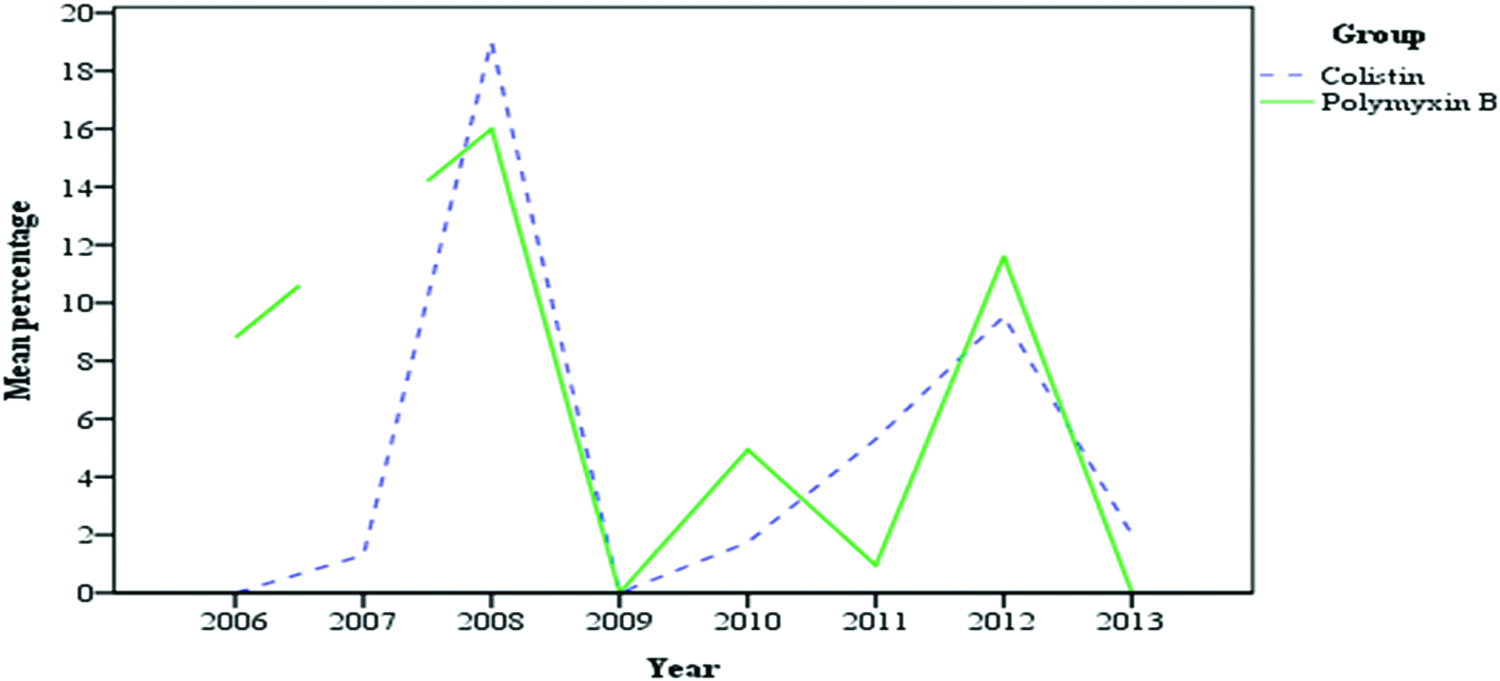
Trends of mean resistance rates of A. baumannii to polymyxins from the early 2006 to end of the year 2013. Color images available online at www.liebertpub.com/mdr
While only one study assessed the MIC value exclusively for PMB on A. baumannii isolates (MIC range, ≤0.5–64 μg/ml; MIC50, ≤0.5 μg/ml; MIC90, 2 μg/ml), 48 six studies determined the MIC only for COL ranging from 0.125 to 1 μg/ml (MIC50, 0.125 μg/ml, MIC90, 0.125 μg/ml), 47 0.04 to 8 μg/ml, 43 0.5 to 6 μg/ml, 60 0.25 to 128 μg/ml (MIC50, ≤1 μg/ml; MIC90, 2 μg/ml), 61 ≤1 to ≥64 μg/ml, 37 and 0.001 to 1 μg/ml (MIC50, 0.01 μg/ml; MIC90, 1 μg/ml) (in 2006) and 0.001 to 30 μg/ml (MIC50, 0.1 μg/ml; MIC90, 2 μg/ml) (in 2011). 38 In two additional studies, MIC of both COL and PMB ranged between <0.25 and 16 μg/ml (MIC90, 4 μg/ml) 39 and 0.12–0.5 μg/ml (MIC50, 0.25 μg/ml and MIC90, 0.5 μg/ml). 11
Regarding the susceptibility of carbapenem-resistant isolates to polymyxins, one study 39 noted that only 4.9% of IMP-resistant A. baumannii isolates were resistant to COL, and all isolates resistant to COL were also resistant to PMB and vice versa. Furthermore, another study found that 69% and 15.4% of COL-resistant isolates were MDR and XDR phenotype, respectively. 44
Susceptibility of A. baumannii to TIG
In 14 studies included in this review, susceptibility of 1,645 A. baumannii isolates to TIG was evaluated. With the exception of three studies, which reported 61.7%, 88%, and 98.4% resistance rate, according to FDA and EUCAST criteria, respectively,36,42,56 we generally found a low rate of resistance against TIG (from 2% to 38.4%) among isolates tested.38–41,44,46,48,50,58,59,63 One study reported that resistance to TIG among all 100 MDR-AB isolates increased from 0% in 2006 to 8% in 2011. 38 In one study, 39 all included IMP- and COL-resistant A. baumannii isolates were sensitive to TIG, and in another, 40 all COL-resistant isolates showed susceptibility to TIG and tobramycin.
Discussion
The intrinsic and acquired antimicrobial resistance of A. baumannii, as well as its association with hospital and antimicrobial exposure and immunosuppressive patients, makes a selection of appropriate antimicrobial therapy simultaneously more difficult and more important. 66 For these reasons, A. baumannii is known today as a “highly successful pathogen” against the many therapeutic, cleaning, and disinfection measures, and its resistance problem has become a serious global challenge. 67 In this situation, antimicrobial resistance surveillance and applying effective infection control programs can help to eradicate A. baumannii strains in hospitals.
According to the results of this review, there is an alarming trend of increase in A. baumannii resistance against a broad spectrum of antimicrobials in Iran. In the recent study, Bahador and his colleagues in a 5-year period study have shown an 11–30% increase in frequency of MDR-AB isolates, which were resistant to different classes of antibiotics. 38 In particular, they found that while 30% of the isolates collected in the year 2006 showed resistance to IMP, carbapenem-resistant isolates rose to 48% in the year 2011. 38 Similarly, in our study, isolates collected between the years 2010 and 2014 had significantly higher weighted mean resistance to carbapenems than isolates recovered from 2006 to 2010 (82.76% vs. 61.2%, and 89.76% vs. 58.27% against IMP and MEM, respectively) (p-value was 0.045 and 0.05, respectively). Generally, these findings are consistent with studies from other countries10,68 and could be striking that carbapenems, which used to be the first available line antimicrobials, have been increasingly compromised and no longer constitute salvage therapy for life-threatening MDR-AB infections.
In this systematic review, polymyxins showed adequate activity against A. baumannii isolates, so that 77–100% and 84–100% of isolates were susceptible to COL and PMB, respectively. With exception of the years 2008 and 2012, we found generally no significant change in the resistance of isolates to these antibiotics during the study period. High prevalence of resistance to these antibiotics can be attributed to the small number of studies during 2008, so that only a single study reported a high frequency of resistance to both COL and PMB (19% and 16%, respectively). In contrast, in light of the higher number of conducted studies in 2012, interstudy difference of resistance rate and collected isolates may justify the high prevalence of resistance to polymyxins, in comparison to other years studied. Comparable findings were obtained by Moradi et al., in which they found a low resistance rate to lipopeptides with no significant trends over the study period. 69 Nevertheless, it is of particular concern that the prolonged exposures to the polymyxins led to increase in MIC determinations, development of resistant strains and, consequently, no optimal activity of the drug in clinical practices; as was shown in the study by Bahador et al., the MIC range, MIC50, and MIC90 values increased 32-fold, 10-fold, and 2-fold for COL within the 5 years, respectively. 38
Unfortunately, resistance to polymyxins has been noted by a number of authors.18–20,26 Moreover, heteroresistance phenotype of A. baumannii, which was first described in 2006 by Li et al., is currently reported much higher than the resistance rate in carbapenem-resistant strains.70,71 Polymyxin heteroresistance in this organism is defined as an isolate with MIC ≤2 μg/ml in which detectable subpopulations are able to grow in the presence of >2 μg/ml.70,71 Unfortunately, there are scarce articles that investigated the rate of heteroresistance or resistant phenotypes after therapy by polymyxins in patients affected by A. baumannii. Only in the one case report of postneurosurgical meningitis, 72 authors described a COL-sensitive A. baumannii isolate that was changed to COL-resistant phenotype after the intravenous and intratracheal treatment of COL. They found that the isolate was COL-heteroresistant and was developed into completely resistant during therapy. Therefore, detection of polymyxin heteroresistance in the clinical isolates of A. baumannii strongly suggests that if inappropriate use of polymyxins be continued, there may be main potential for the rapid development of resistance and therapeutic failure. In this scenario, the use of this class of antibiotics in combination with various agents, preferably RIF or MEM, is suggested to be the only remaining strategy for a bactericidal benefit. Among the various combination regimens, the COL/RIF combination showed promising results in vitro, in vivo, and in the clinic for MDR-AB,73,74 whereas COL/carbapenems showed a good activity in few studies. 75 It is worth noting that although in the present review, the susceptibility rate to RIF of A. baumannii was estimated low, in vitro studies and experimental models of infection have shown an additive or synergistic effect for combination of RIF with other antibiotics, such as COL, carbapenems, and TIG.76–78
Along with polymyxins, TIG was found to have a good in vitro activity and in vivo effectiveness against MDR-AB.79,80 However, the emergence of the resistance has been observed during the treatment of infections caused by MDR Acinetobacter species81,82 and also identified in in vitro susceptibility studies.39,40 The current study indicated the incidence of resistance to TIG ranging from 2% to 38.4% among the majority of A. baumannii tested. Alarming higher resistance rates were also reported in some studies (61.7%, 88%, and 98.4%).36,42,56 Although susceptibility to TIG may vary with the testing method and the criteria for interpretation of test results, 83 development of resistance is particularly worrying and should be studied more, while this drug had not been introduced commercially in our country.
In conclusion, based on evidences obtained from this review, polymyxins and TIG have adequate in vitro activity against A. baumannii isolates. As mentioned above, since the clinical efficacy of TIG remains a matter of controversy, polymyxins, especially COL, could be used as the last resort for the treatment of infections resulted from MDR/XDR A. baumannii. Actually, these older antibiotics have revived in medical practice over the last decade against the severe hospital-acquired infections caused by carbapenem-resistant Gram-negative bacilli. The optimal use of polymyxin antibiotics and combination therapy with other antimicrobials, preferably RIF and MEM, has been suggested to maintain their effectiveness in the face of heterogeneous or homogenous resistance among such problematic bacteria. Finally, given the rapidly increased resistance rate of A. baumannii in hospital environments, better understanding of the antibiotic patterns and optimization of antimicrobial prescription strategies is essential to control the emergence of drug-resistant strains.
Authors' Contributions
A.A. designed the study and collected, analyzed, and interpreted the data and wrote the article; H.R.N. contributed to analyzing the results and reviewing the article. J.M. was involved in the interpretation of results and reviewing the article.
Footnotes
Disclosure Statement
No competing financial interests exist.