
Abstract
Objective:
The objective was to characterize a group of clinical isolates of fluoroquinolone-resistant Haemophilus parainfluenzae collected in Northern Spain (March–December 2014).
Methods:
Twelve clinical isolates of H. parainfluenzae were studied by performing antimicrobial susceptibility testing and PCR amplification and nucleotide sequencing of the QRDR (quinolone resistance-determining region) of gyrA, parC, gyrB, and parE genes. Screening for plasmid-mediated quinolone resistance (PMQR) was also studied. Pulsed-field gel electrophoresis (PFGE) was used for molecular typing.
Results:
Antimicrobial susceptibility testing showed that all the isolates were resistant to the fluoroquinolones tested (ciprofloxacin, levofloxacin, norfloxacin, and moxifloxacin). Analysis of the QRDR demonstrated that all the isolates presented mutations in gyrA and parC. A Glu88Lys substitution in ParC is reported for the first time in H. parainfluenzae. No PMQR gene was detected. PFGE results showed that isolates were not clonally related.
Conclusion:
Multiple H. parainfluenzae fluoroquinolone-resistant isolates grouped in the same area in a short period of time showed diverse substitutions in QRDR of gyrA/parC and were not clonally related, indicating individual emergence. In addition, we described the first report of Glu88Lys substitution in ParC.
Introduction
H
Resistance to fluoroquinolones in this species is rare. It was reported for the first time in 2003 in clinical isolates from Japan. 4 Later studies noted only sporadic strains of fluoroquinolone-resistant H. parainfluenzae in Canada, Switzerland, and Spain.5–8 The molecular mechanisms underlying this resistance are similar to those reported for H. influenzae and other gram-negative bacteria.9,10 Genetic mutations that lead to amino acid substitutions in the QRDR (quinolone resistance-determining regions) of gyrA (Ser84 and Asp88) and parC (Ser84) have been associated with resistance in H. parainfluenzae.5–8
In other bacteria, plasmid-mediated quinolone resistance conferring low levels of quinolone resistance has been documented.11,12 In Haemophilus spp., this mechanism has been described in H. parasuis isolated in China, 13 although so far this mechanism has not been reported for H. parainfluenzae.
The objective of this study was to characterize 12 clinical strains of H. parainfluenzae with resistance to fluoroquinolones within a short period of time (March–December, 2014).
Materials and Methods
The strains were collected at the Joan XXIII Hospital, Tarragona (Spain), a community hospital with 380 beds that serves a population of 600,000 inhabitants. The isolates were recovered from respiratory tract (10 isolates) and skin/soft tissue (2 isolates) specimens of different patients. Only patients with compatible clinical findings of infection and H. parainfluenzae as the only microorganism recovered from the culture were included. The main characteristics of patients are listed in Table 1.
Community infection was defined as infection contracted outside of a healthcare setting. Nosocomial infection was defined as infection that appears 48 hours or more after hospital admission.
COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; F, female; FNAP, fine-needle aspiration puncture; HT, hypertension; LRI, lower respiratory infection; M, male.
The identification of H. parainfluenzae was performed by conventional methods (Gram stain, oxidase, catalase, and requirement of hemin and NAD growth factors) and confirmed by mass spectrometry (MALDI-TOF Bruker Daltonics, Germany).
Minimum inhibitory concentration (MIC) values of ciprofloxacin, levofloxacin, norfloxacin, and moxifloxacin were determined by E-test (bioMérieux, Spain) on Haemophilus Test Medium (HTM) (Oxoid Ltd., Spain) following Clinical and Laboratory Standards Institute (CLSI) guidelines. 14 Susceptibility to ampicillin, amoxicillin–clavulanic acid, cefuroxime, cefotaxime, meropenem, azithromycin, chloramphenicol, trimethoprim/sulfamethoxazole, and tetracycline were determined by disk diffusion on HTM agar according to CLSI guidelines. 14 H. influenzae ATCC 49247 served as quality control. To investigate the role of the mutations in the QRDR, the changes in gyrA, gyrB, parC, and parE genes were determined using specific primers, as described previously. 8 The genome of the fluoroquinolone-susceptible strain, H. parainfluenzae T3T1, was used for comparison (EMBL/GenBank, accession number FQ312002).
PCR of plasmid-mediated quinolone resistance genes (qnrA, qnrB, qnrC, qnrD, qnrS, aac(6’)-Ib-cr, qepA, and oqxAB) was performed using previously described primers. 12
Genetic relatedness was assessed using pulsed-field gel electrophoresis (PFGE) as reported previously. 15 In brief, the bacterial cells were harvested from a chocolate agar plates and suspended in Tris-ethylenediaminetetraacetic acid (EDTA) (100 mM Tris, 100 mM EDTA, pH 8) at a OD610 = 1.6. The plugs were prepared using an equal volume of molten low melting agarose and treated with 20 μl proteinase K (20 mg/ml) at 50°C before hardening. After that, the plug was treated with the lysis solution (50 mM EDTA, 50 mM Tris, and 1% sarcosyl, pH 8) and 25 μl proteinase K (20 mg/ml). After washing the block thoroughly with distilled water, the genomic DNA was digested with ApaI for 2 hours in a shaking water bath. The blocks were embedded in the wells of 1% agarose gel and electrophoresed at 6 V/cm and 14°C for 23 hours with a pulse time ramp of 1–15 seconds for 7 hours and 15–35 seconds for 16 hours with a CHEF-DR II System (Bio-Rad, Belgium).
Results and Discussion
Resistance to fluoroquinolones in H. parainfluenzae is uncommon. Since it was first reported, it has been described only in occasional isolates. This study presents the characterization of 12 strains with fluoroquinolone resistance collected in a short period of time (March–December 2014) in the same hospital located in Tarragona, Spain. The strains showed elevated MIC values for all the fluoroquinolones tested and were clinically resistant according to CLSI. 14 The MICs of ciprofloxacin, levofloxacin, norfloxacin, and moxifloxacin are shown in Table 2. To note, five of them showed high-level resistance phenotype (Hpa1, Hpa2, Hpa3, Hpa9, and Hpa10; ciprofloxacin MIC ≥32 mg/L). The antimicrobial susceptibilities to other antibiotics are shown in Table 3.
CIP, ciprofloxacin; LEV, levofloxacin; MIC, minimum inhibitory concentration; MOX, moxifloxacin; NFX, norfloxacin.
AMC, amoxicillin–clavulanic acid; AMP, ampicillin; AZT, azithromycin; CHL, chloramphenicol; CTX, cefotaxime; CXM, cefuroxime; MPM, meropenem; SXT, trimethoprim–sulfamethoxazol; TET, tetracycline.
Fluoroquinolone resistance in H. parainfluenzae has been related to mutations in GyrA (Ser84 and Asp88) and ParC (Ser84).15–17 According to this, mutation analysis of QRDRs showed that all strains in this study carried changes at the same positions of GyrA (Ser84 and Asp88) and ParC (at Ser84). The amino acid substitutions found are shown in Table 1.
For GyrA, Ser84Phe was found in 10 strains and Ser84Tyr in two strains. Ser84Phe has been reported previously in H. parainfluenzae linked to resistance to fluoroquinolones, and Ser84Tyr has been detected in H. parasuis isolates.5,16–18 All strains showed the Asp88Tyr substitution also found frequently in quinolone-resistant Haemophilus spp. isolates, including H. parainfluenzae.5,10,16–19 Three strains showed an additional Lys130Arg change, which has not been reported previously and whose role in fluoroquinolone resistance has yet to be determined.
There was greater variation in ParC changes at Ser84, with Ser84Tyr, Ser84Phe, and Ser84Leu being detected in 5, 4, and 3 strains, respectively. All these substitutions have been reported by other authors in Haemophilus spp. isolates.5,9,16 Interestingly, Hpa1 harbored the Glu88Lys mutation, a ParC change not previously described in H. parainfluenzae. It is worth noting that this mutation has been linked to fluoroquinolone resistance in H. influenza and H. parasuis.9,10,18,19
All strains presented additional changes in ParC, such as Met198Leu and Ser138Thr, substitutions in equivalent positions have previously been reported in H. influenzae, although their involvement in quinolone resistance has not yet been established.10,16 As far as we know, the substitutions Val91Glu, Pro203Leu, and Ala205Val have not been described previously in Haemophilus spp.
Four strains showed substitutions in ParE, the change in Asp420Asn has been reported by other authors in H. influenzae and H. parainfluenzae, but Ala403Pro and Gly457Ala have not been detected before.10,17 GyrB modifications were not detected (Table 1).
Finding strains with similar mutation patterns but different susceptibility values would suggest the presence of additional resistance mechanisms and hence the presence of plasmid-mediated quinolone resistance was investigated. PCR of qnrA, qnrB, qnrC, qnrD, qnrS, aac(6’)-Ib-cr, qepA, and oqxAB was performed but none of these genes was detected. To our knowledge, only one study has reported such mechanisms present in Haemophilus spp., when qnr and aac(6’)-Ib-cr were detected in H. parasuis strains isolated from pigs. 13 In this study, none of the known plasmid-mediated mechanisms was implicated in fluoroquinolone resistance. It is possible that other mechanisms decreasing permeability or increasing efflux could contribute to the resistance; further studies would be needed in these isolates to confirm this hypothesis.
ApaI-PFGE typing was performed and the results showed that all isolates exhibited individual DNA patterns, indicating that all isolates were genetically distinct (Figure 1).
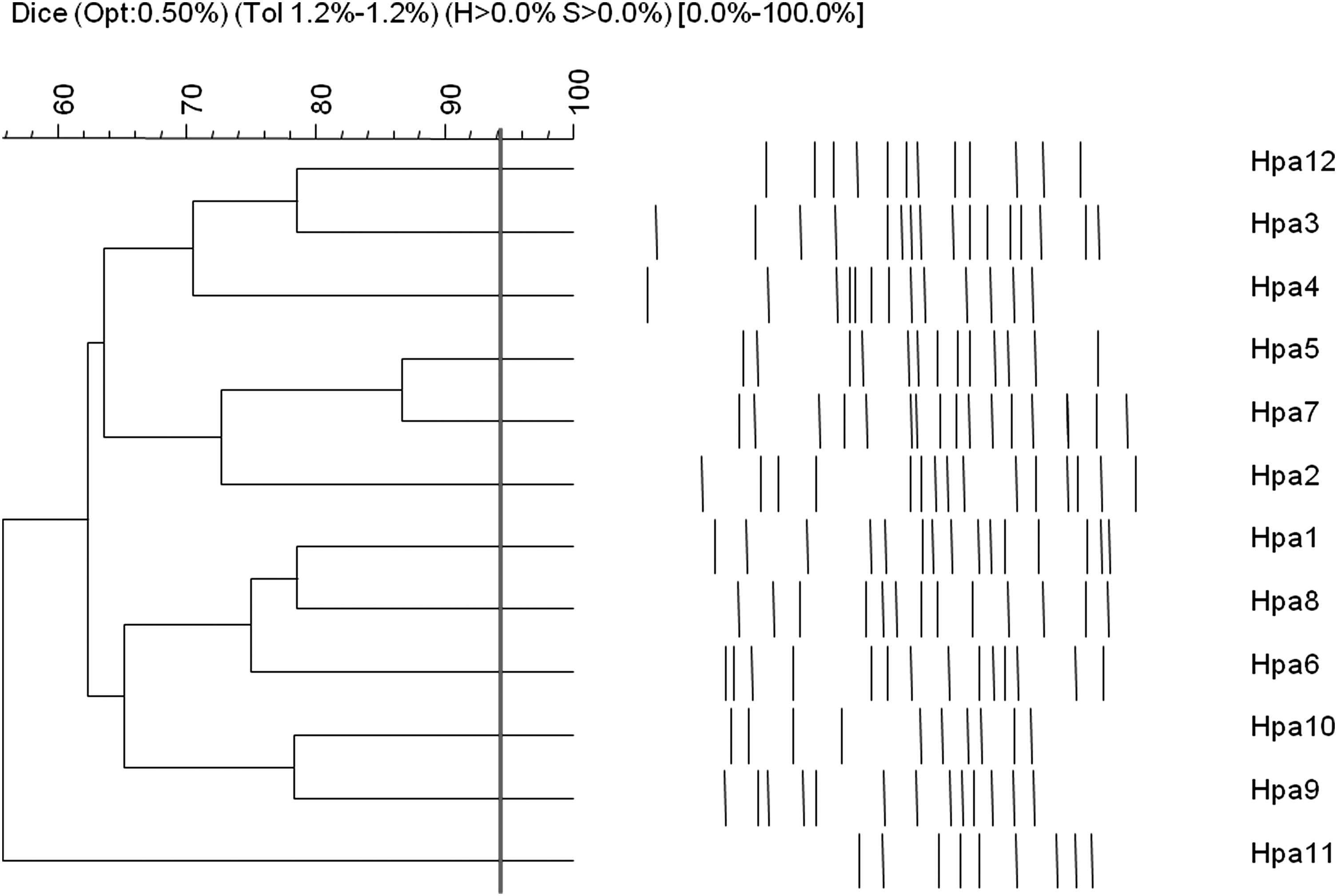
Dendrogram of the ApaI pulsed-field gel electrophoresis patterns of 12 H. parainfluenzae isolates. The vertical dark gray line indicates the 94% similarity level for purposes of comparison.
Despite the clonal spread that might be expected due to the presence of an uncommon phenotype in a group of strains collected in the same long-term care facility, PFGE results reflected high genetic diversity. The different patterns observed in the antimicrobial susceptibility assays also support the nonclonality of the isolates. No correlation was observed between PFGE and antibiotic resistance profile. The finding of nonclonal isolates indicates that the emergence of these strains is not related to the dissemination of a clone in the hospital, but arises individually in each patient in response to unknown factors. According to this, most of the infections were community acquired, which could explain the nonclonal nature of the isolates.
Another possibility that would explain the clustering of resistant isolates would be related to a possible genetic recombination in the QRDR region in a narrow ecological niche. This phenomenon would be similar to the ftsI gene mutations studied in H. influenzae and H. haemolyticus. 20 More studies will be needed to test this hypothesis in the QRDR of Haemophilus spp.
Fluoroquinolones are commonly used for the empirical treatment of various infections, and this selective pressure could promote the emergence of fluoroquinolone-resistant H. parainfluenzae strains. This, in addition to the increasing role of this pathogen in invasive infections, suggests the need for surveillance studies to discover how prevalent this phenotype is. In addition, fluoroquinolone resistance should be ruled out in clinical isolates of H. parainfluenzae.
Footnotes
Acknowledgments
Part of this study was presented at the European Congress of the Society of Microbiology and Infectious Diseases (25th ECCMID) held in Copenhagen from April 25–28, 2015. This work was partially supported by the Ministerio de Economía y Competitividad, Instituto de Salud Carlos III and cofinanced by European Development Regional Fund “A way to achieve Europe” ERDF, Spanish Network for the Research in Infectious Diseases (REIPI RD12/0015).
Disclosure Statement
No competing financial interests exist.