
Abstract
Limited knowledge is available on regional distribution of antituberculosis (TB) drug resistance and on province-specific time-trends in TB drug susceptibility in China. To obtain the latest information about the dynamics of drug-resistant TB in Gansu province, we conducted a retrospective study and analyzed data on drug resistance among new TB cases diagnosed between June 2010 and May 2014 in Gansu, China. The data were collected from the only TB surveillance and treatment hospital in Gansu and, therefore, represented the epidemiology of TB in the province. The drug resistance was defined based on diagnostic drug susceptibility testing. Overall, 17.3% of TB new cases diagnosed during 2010 to 2014 in Gansu presented resistance to at least one anti-TB drug. And a total of 2.9% of new TB cases have multidrug resistance. The prevalence of multidrug-resistant TB in Gansu was found to resurge after 2013 (2.0%) after a steady decline between 2010 and 2012 (from 7.1% to 1.2%). The drug resistance patterns of TB and their revolution trends in Gansu differed from other regions of China. We report the first epidemiological description of drug-resistant TB in Gansu, which is distinct when compared to other regions. Our data demonstrate that the distribution of drug-resistant TB varies to a great extent among different geographic regions. And the results of our study greatly suggest that the implementation of individualized TB management and regimen policy based on the regional epidemiology of TB drug susceptibility is highly required.
Introduction
T
In addition, globally, the detected drug resistance represented only 41% of this global estimate, revealing a detection gap.1,2 Worldwide, 12% of estimated resistant cases from new and 58% from previously treated patients were tested for drug resistance in 2014, leaving the majority of estimated MDR-TB untested. A direct consequence of the detection gap is the spread of drug-resistant TB and a relative low rate of successful treatment—about 50% for MDR-TB globally.1,2 To ensure all patients diagnosed with TB start on a proper treatment, it is essential to reduce and eliminate the gap between detection and treatment of drug-resistant TB. The elimination of the detection gap is more challenging in China, where the number of MDR-TB cases detected was only 11% of the number of notified cases estimated to have multidrug resistance.1,2
Considering these facts, a better understanding of resistance profiles of TB is highly needed to design surveillance of drug-resistant TB, to improve the treatment outcome of MDR-TB, and to develop novel therapeutic regimens. However, it is yet unachieved in most countries, including China, mainly due to limited knowledge of regional susceptibility profiles of anti-TB drugs. In the current study, we describe in depth the resistance patterns among TB patients in Gansu. Our study provides the first epidemic description of drug-resistant TB in Gansu that is distinct to other regions in China. This datum serves as the basis for implementing the region-specific strategies to improve MDR-TB detection, to assess epidemiological trends, and to predict outbreaks of drug-resistant TB in Gansu.
Materials and Methods
Patient cohort and sample processing
The demographic and microbiological data for this study were retrospectively collected between June 2010 and May 2014 in the Pulmonary Hospital of Lanzhou, Infectious Disease Hospital of Gansu province. The hospital is the only official surveillance and clinical hospital for monitoring and treating TB, and an effort was made to access all available cases and data, hence, the data collected in this study exemplify the epidemiological state of TB during the study period in the province.
Patients enrolled in this study all presented respiratory symptoms when attended the TB clinic. At the first presentation, sputum samples, bronchoalveolar lavage, or body liquid were collected from the patient and subjected to routine Ziehl–Neelsen smear examination. TB was diagnosed based on the updated WHO guidelines for the programmatic management of drug-resistant TB. 11
Patients with concomitant HIV, hepatitis B virus (HBV), or hepatitis C virus (HCV) infections or oncological diseases were excluded from the study. In addition, subjects were excluded from this study if they have been treated before DST and the remaining subjects were included in the further analyses (Fig. 1).

Flowchart of TB cases selection. DST, drug susceptibility testing; MDR, multidrug-resistant tuberculosis; TB, tuberculosis; XDR, extensively drug-resistant tuberculosis.
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and the principles of Good Clinical Practice. As the study utilized the retrospectively collected surveillance data in anonymity, written informed consent was not required. The hospital ethical review board approved this study as it did not undertake primary research on human subjects.
Drug susceptibility test
The mycobacterial culture and DST was performed on Löwenstein–Jensen solid media following the WHO guidelines 4 and was determined by means of the proportion method on isolates from patients with suspected TB using BD BACTEC™ MGIT™ 960 Culture System (Becton Dickinson & Co., Franklin Lakes, NJ), following the manufacturer's instruction. The performance of culture and the concentrations of anti-TB drugs for the DST were same as described before.12,13 The isolates were designated either resistant or sensitive by comparing the growth of isolate in media containing anti-TB drugs with that in control media. Since 2014, Genotype MTBDR (Hain Lifescience, GmbH, Germany) was implemented in the hospital. All isolates from suspected TB patients were routinely subjected to Genotype MTBDR test before DST as well as for isoniazid (INH) and rifampicin (RFP) susceptibility.
The DST results for the first-line drugs INH, RFP, ethambutol (EMB), and rifapentine (RFT), the second-line drugs protionamide (TH) and 4-aminosalicylic acid (PAS), and the injectable drug streptomycin (SM) were available for all enrolled patients between 2010 and 2014; for the fluoroquinolone drug levofloxacin (LFX) and injectable drug kanamycin (KM) between 2012 and 2014.
MDR-TB definitions
The different types of drug resistance were defined according to the international guideline. 4 Based on the results of DST, the TB strains were determined as monoresistance (MR) when they were resistant to one first-line anti-TB drug only; polyresistance (PR) when resistant to more than one first-line anti-TB drugs other than INH and RFP; MDR as they were resistant to both INH and RFP; or XDR as MDR with additional resistance to any fluoroquinolone and at least one of three second-line injectable drugs.
Data analysis and statistical analyses
The number of subjects sensitive or resistant to each individual drug in the nonselected population and selected subpopulations, such as new cases diagnosed in a specific year, were counted first. Then the incidences of different resistance patterns were calculated. The incidence is defined as the proportion of drug-resistant TB to all tested cases in a specific period. Statistical analyses were performed using SPSS (v21) software. The difference between incidences in percentages was observed by using chi-square test. Patient characteristics were analyzed using chi-square tests for categorical variables or ANOVA test for continuous variables. All reported p values were two-sided. Significant differences were considered in all cases when p < 0.05.
Results
Patient characteristics
The patient cohort was assembled as shown in Fig. 1. Between June 2010 and May 2014, a total of 3,100 patients with TB were clinically diagnosed in the Pulmonary Hospital of Lanzhou. Of these, 321 were excluded because only cerebrospinal fluid or pleural effusion from these patients was available. The remaining subjects (n = 2,779) were further enrolled in the study. The mean age of the enrolled patients was 41.21 (SD: 19.67), and 991 of them were female (35.7%). The data were further stratified by calendar years, which revealed a slightly different age distribution during the study period (p: 0.04) (Table 1). The enrolled patients in 2011 have a smaller female representation (27.4%; p < 0.001). Out of these cases, 1,666 were negative upon mycobacterial culture (60%) and 1,113 were positive (40%). The positive culture specimens were further used for DST analyses.
Drug susceptibility patterns of TB patients in Gansu
Drug resistance to the first-line drugs was found in 803 patients (28.9% of all enrolled subjects) (Table 2). We observed a peak of MR in 2013 (n = 114), composing 14.8% of tested subjects in that year (Fig. 2A). Conversely, the percentage of PR was continuously rising before 2013 and from 13.2% in 2010 to 19.3% in 2012. The incidence of PR had a steep decline in 2013 (11.3%) and then an increase again in 2014 (12.9%) (Fig. 2A).
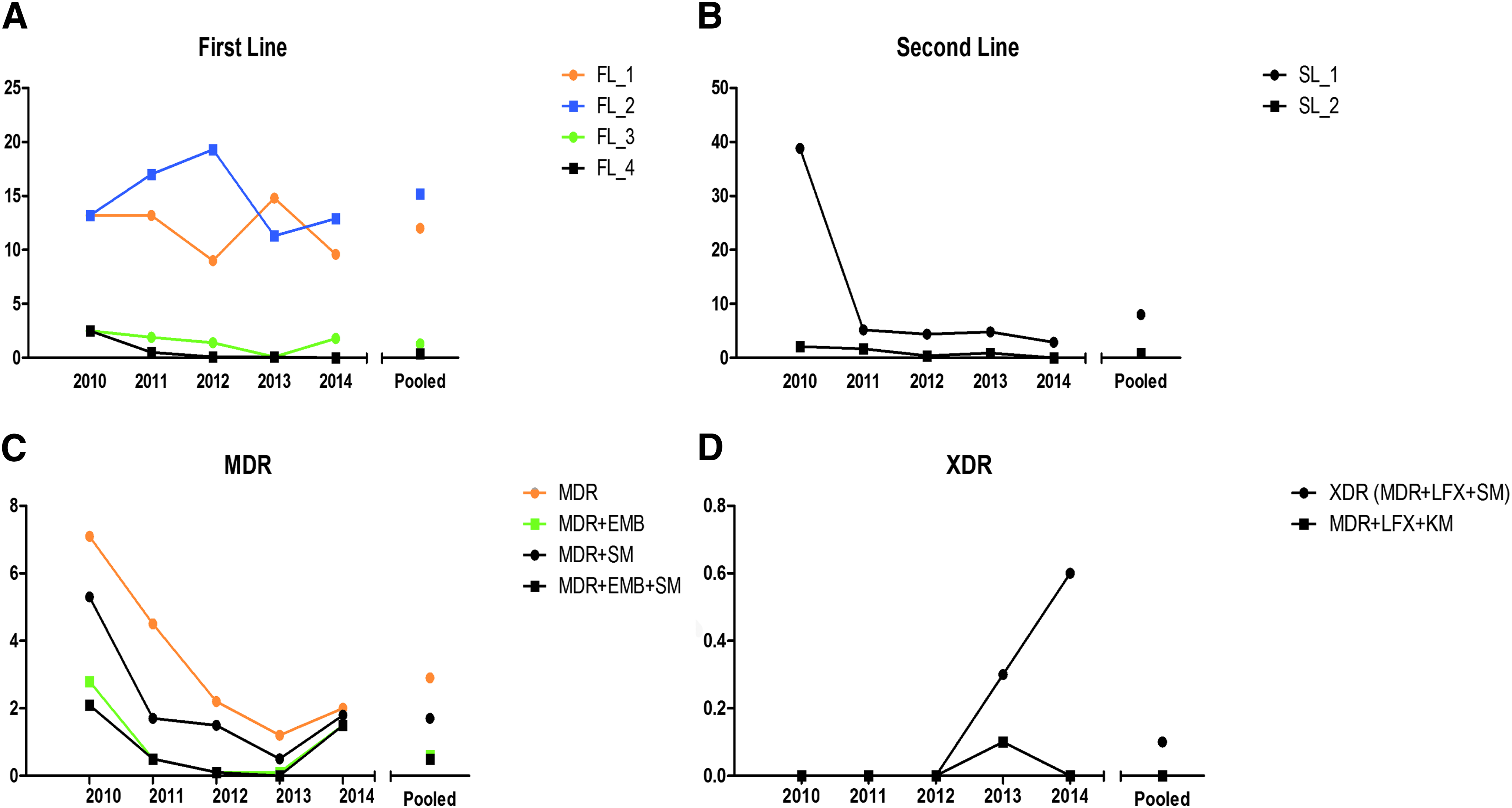
Distinct profiles of drug-resistant TB among new cases between 2010 and 2014 in Gansu, China. The incidence is defined as the proportion of drug-resistant TB to all tested cases in a specific period. We evaluated the incidences of TB subjects resistant to first-line drugs
EMB, ethambutol; INH, isoniazid; KM, kanamycin; PAS, 4-aminosalicylic acid; RFP, rifampicin; RFT, rifapentine; SM, streptomycin; TH, protionamide.
A total of 248 patients were resistant to the second-line drugs. Of these, 222 were resistant to a single drug and 22 to more than one second-line drug. In 2010, we found that 109 patients were resistant to one second-line drug, comprising 38.8% of tested subjects in that year. This percentage was sharply decreased to 5.2% in 2011 and more thereafter. The prevalence of resistance to more than one second-line drug remained low between 2010 and 2013 (0.1–2.1%) and was absent in 2014 (Fig. 2B).
The altered landscape of MDR-TB patients in Gansu
A total of 80 patients were identified as MDR-TB in a period of 5 years (2010–2014), corresponding to 2.9% of tested subjects. Remarkably, a steady decrease in incidence rate of MDR-TB among tested TB patients was observed between 2010 and 2013, from 7.1% to 1.2%. However, the incidence of MDR-TB between January and May 2014 was 2.0%, indicating an increasing trend in 2014 (Table 3 and Fig. 2C).
LFX, levofloxacin; MDR, multidrug-resistant; PR, polyresistance.
The evaluation of LFX and KM was implemented as a routine test since 2012. As a consequence, the susceptibility data of XDR were only available between 2012 and 2014. Within 3 years, we only detected one XDR-TB case, which was a case of MDR with additional resistance to LFX and KM (Table 3 and Fig. 2D).
In addition to these, we assessed other MDR patterns. MDR-TB subjects with additional resistance to EMB and/or SM showed the same pattern with a regress in 2014 as MDR-TB was demonstrated (Fig. 2C). MDR-TB with additional resistance to LFX and SM showed a steady increase from 0% to 0.6% since 2012 (Table 3 and Fig. 2D).
Discussion
In the current retrospective study, we investigated the 5-year epidemiology of drug-resistant TB in Gansu province. Our data defined a distinct TB resistance profile of Gansu. We observed a tendency of decreased prevalence for TB resistant to more than two first-line drugs as well as to second-line drugs. Most importantly, we found that resurgence of MDR-TB and extensive MDR-TB since 2013 after a steady decline between 2010 and 2012.
Since it was first described in early 1980's, 14 MDR has been a serious public health issue in many developing countries, including China. The treatment of MDR-TB is fairly difficult and expensive. For this reason, the knowledge of regional TB resistance profile is imperative for designing proper therapeutic strategies, development of novel drugs, and also for making public surveillance policy. Few studies have reported regional resistance status of anti-TB drugs, and these studies suggested spatial and temporal variations in anti-TB drug susceptibility.15–18 Our data demonstrated that the incidence of drug-resistant TB strains (17.3%) in Gansu is lower than that in other areas in China, which are ranging from 21.2% to 54.4% in the same period.7,13,15,19 Furthermore, the dynamics of the overall drug resistance in Gansu differs from other areas. We observed a declining trend in Gansu between 2010 and 2014 with an increase in 2013 (Table 3), while the prevalence of drug-resistant TB continuously increased in Beijing and remained stable in Shandong province during that period.7,13 It reflects the association between drug-resistant TB epidemic and population immigration, local socioeconomy. Beijing has the biggest population of immigrants in China, which consists of a large proportion of young nonresidents from distant rural regions where the TB incidence is high and poorly controlled. Shandong is one of the richest provinces of China, and its public health programs are well implemented. Compared with Beijing and Shandong, Gansu has a very small and stable population. Although it results in a low risk of spreading of drug-resistant TB, the slow economic development of Gansu retards the proper control of drug-resistant TB strains. As a consequence, a stable decline of the prevalence of drug-resistant TB has not been obtained
The overall rate of resistant TB strains to the first-line drugs in Gansu is 12% between 2010 and 2014, notably lower than that in Beijing (30.6–50.1% during 2006–2012) and in Shandong province (21.2% between 2007 and 2014).7,13 Despite the lower overall rate, the resistance patterns for individual first-line drugs diverge largely between four tested drugs. Compared to Beijing, the prevalence of resistant TB to all four first-line drugs is considerably lower in 2012, except for INH and EMB (Table 2). 13 Compared with Shandong, Gansu has a lower prevalence of cases with TB strains resistant to INH and EMB, however, prevalence of resistant strains to RFP in Gansu is over three times more frequent than that in Shandong. 7 The larger spread of RFP-resistant TB strains in Gansu might be attributed to distinct TB strains locally dominant in Gansu, which is to be investigated in the future by performing extensive genotyping and molecular characterization of all TB subjects.
Strikingly, the multidrug-resistant TB in Gansu is 2.1-fold (MDR-TB) and 14-fold (MDR+SM/EMB-TB) less prevalent compared with Beijing, while similar to other northern areas in China.13,19 When compared with Shandong, a divergent trend was noticed, similar to the situation of TB strains resistant to first-line drugs. Out of all TB patients, 2.9% and 0.6% patients were resistant to MDR-TB or MDR+EMB-TB, respectively, in Gansu, while these incidences in Shandong are 1.0% and 0.1%. 7 Nevertheless, the rate of MDR had a decrease between 2010 and 2013 in Gansu, contrasting to the trend of MDR-TB in other regions observed in the similar period.7,13,15,19 The resurgence of MDR-TB in Gansu during the first 5 months in 2014 might be explained by a more sensitive screening test used in 2014-Genotype MTBDR. Nevertheless, close surveillance is advocated to monitor the changing trend of MDR-TB in Gansu.
We noticed that in general TB patients in China tend to have less risk of developing MDR than European patients, as evidenced by the proportions of developed MDR-TB among new cases in China (overall 7.0%) and in 51 estimated European countries (15.7%).18,19 Nevertheless, the proportion of TB new cases with MDR varies largely within Europe, between western and eastern Europe (range 0–34.8%), suggesting global spatial variations in MDR-TB incidence.
In the current study, we assessed the prevalence of XDR between January 2013 and May 2014. Although the observation period is relatively short, the emergence of XDR urged the need for the routine test of susceptibility of LFX and injectable drugs, for example, KM, in specimens from confirmed MDR-TB patients. Moreover, new TB therapeutic regiments need to be developed to provide more treatment options for those patients.
By retrospectively analyzing the drug-resistant patterns of TB in Gansu during 2010 and 2014, we illustrate that the distinct profile of TB resistance is geographically impacted and dynamically changed. We point out that the implementation of individualized TB management and regimen policy based on the regional epidemiology of TB drug resistance is certainly urgent to achieve TB control and elimination.
Footnotes
Acknowledgments
This study was supported by Medical Scientific Development Foundation of Lanzhou, China, grant number LZWSKY2014-2-20. J.H. is supported by the Virgo consortium, funded by the Dutch government project number FES0908. The authors would give special thanks to Dr. Andre Boonstra for intensive discussion and manuscript emendation.
Disclosure Statement
The authors report no conflicts of interest in this work.