
Abstract
Streptococcus pneumoniae isolates (2,614) were collected from patients at 135 U.S. Medical Centers during 2014. Isolates were evaluated for multidrug resistance to penicillin, ceftriaxone, erythromycin, tetracycline, trimethoprim–sulfamethoxazole, and levofloxacin. A single isolate (853008) demonstrated a ceftaroline nonsusceptible minimal inhibitory concentration (MIC) value, and it was subjected to molecular characterization. Ceftaroline (MIC50/90, ≤0.015/0.12 μg/ml) was eightfold more potent than ceftriaxone (MIC50/90, ≤0.06/1 μg/ml) against all isolates. For multidrug-resistant (MDR) isolates (28.8% of tested strains), ceftaroline (MIC50/90, 0.06/0.25 μg/ml; 99.9% susceptible) was the most active agent tested, being eightfold more active than ceftriaxone (MIC50/90, 0.25/2 μg/ml; 81.5% susceptible at MIC, ≤1 μg/ml) and 16-fold more active than penicillin (MIC50/90, 0.25/4 μg/ml; 78.5% susceptible at MIC, ≤2 μg/ml). Isolate 853008 was a single locus variant of sequence type 377 and serotype 35B. It had multiple substitutions in the penicillin-binding proteins (PBPs), mainly PBP2x, when compared with reference sequences from the R6 strain. Isolate 853008 showed 31 amino acid alterations in MurM. The in vitro data presented here confirm that ceftaroline potency against S. pneumoniae to be higher than other β-lactams, including against those isolates demonstrating ceftriaxone nonsusceptible and MDR phenotypes.
Introduction
C
Seroprevalence studies in the United States conducted during 2011–2012 found that serotypes 19A and 35B were the most prevalent serotypes recovered from infected patients. 7 Importantly, serotypes 19A and 35B comprised the majority of S. pneumoniae isolates with decreased susceptibility to penicillin, ceftriaxone, and other agents employed in the treatment of CABP.2,5 Significant declines in penicillin-resistant S. pneumoniae (PR-SP) and MDR-SP have been attributed to the efficacy of PCV13 against serotype 19A; however, proportional increases in replacement serotypes that have PR-SP or MDR-SP phenotypes (e.g., 35B, 23A, 23B, and 15B) have prevented a more substantial decline in pneumococcal resistance rates.2,5
Given these concerns, there is a need for continued assessment of new and established antibacterial agents for activity against emerging drug-resistant subsets of S. pneumoniae from clinically infected patients. 8 Ceftaroline fosamil is a parenteral prodrug that is hydrolyzed in vivo to release the active agent ceftaroline.9,10 Ceftaroline displays broad-spectrum in vitro activity against S. pneumoniae, including PR-SP and MDR-SP isolates, Staphylococcus aureus, including methicillin-resistant (MRSA) isolates, and Enterobacteriaceae that do not produce an extended-spectrum β-lactamase.2,4,8,11–14
The superior activity of ceftaroline against isolates with elevated minimal inhibitory concentrations (MICs) to other β-lactams has been attributed to its affinity for altered penicillin-binding protein targets (PBP-1A, -2B, and -2X) associated with β-lactam resistance in S. pneumoniae.15,16 Ceftaroline fosamil is approved by the U.S. Food and Drug Administration and the European Medicines Agency for the treatment of CABP and acute bacterial skin and skin structure infection (ABSSSI) in adults and children 2 months of age and older, including ABSSSI caused by MRSA.9,10,17,18
The Assessing Worldwide Antimicrobial Resistance Evaluation (AWARE) Program has monitored ceftaroline activity against bacterial organisms in U.S. medical centers since 2008.4,11,12,14,19,20 The aim of this report is to describe the activity of ceftaroline and comparator agents against S. pneumoniae, including MDR isolates, collected from U.S. medical centers participating in the AWARE Program in 2014. Moreover, an analysis of the amino acid sequences of PBPs and MurM from a single isolate exhibiting a nonsusceptible (NS) ceftaroline MIC result is presented.
Materials and Methods
Bacterial isolates
A total of 2,614 isolates of S. pneumoniae were collected from patients in 135 medical centers representing all nine U.S. Census Bureau divisions from January to December 2014 as part of the AWARE Program. Only isolates deemed clinically relevant by the submitting laboratory were included (one isolate per patient infectious episode). The isolates were from community-acquired respiratory tract infections (956 isolates; 36.6%), healthcare-associated bacterial pneumonia (HCABP; 945 isolates; 36.2%), bloodstream infections (BSIs; 525 isolates; 20.1%), skin and skin structure infections (66 isolates; 2.5%), and other infection types (122 isolates; 4.7%). Regarding age group, isolates were collected from patients ≤5 years old (448 isolates; 17.1%), 6–17 years old (211 isolates; 8.1%), 18–49 years old (485 isolates; 18.6%), 50–64 years old (668 isolates; 25.6%), and ≥65 years old (708 isolates; 27.1%), and the age was not reported for 94 patients (3.6%). Isolates were submitted to the central monitoring laboratory (JMI Laboratories, North Liberty, IA) for identification, susceptibility testing, and molecular characterization as needed.
Antimicrobial susceptibility testing
Broth microdilution tests were conducted at the central reference laboratory according to Clinical and Laboratory Standards Institute (CLSI) methods to determine the susceptibility to ceftaroline and comparator antimicrobial agents. 21 Validated MIC panels were manufactured by ThermoFisher Scientific (Cleveland, OH). S. pneumoniae isolates were tested in cation-adjusted Mueller–Hinton broth supplemented with 2.5% to 5% lysed horse blood according to CLSI document M07-A10. 21 The quality control strain of S. pneumoniae ATCC 49619 was tested concurrently with clinical isolates. Susceptibility determinations and quality assurance of MIC results were based on CLSI guidelines.21,22 The ceftaroline susceptibility breakpoint applied in this study was ≤0.5 μg/ml as published by CLSI (2016). 2
MDR status was determined based on NS to ≥2 classes of the following antimicrobial agents: penicillin (MIC, ≥4 μg/ml), ceftriaxone (MIC, ≥2 μg/ml), erythromycin (MIC, ≥0.5 μg/ml), levofloxacin (MIC, ≥4 μg/ml), tetracycline (MIC, ≥2 μg/ml), and trimethoprim–sulfamethoxazole (TMX; MIC, ≥1 μg/ml). Further susceptibility analyses were performed for S. pneumoniae isolates that tested as NS to ceftriaxone, penicillin, amoxicillin–clavulanate, erythromycin, and levofloxacin, respectively.
Next generation sequencing and target gene analysis
A single isolate (853008) demonstrating a ceftaroline MIC value of 1 μg/ml was subjected to next generation sequencing. Total genomic DNA was extracted using the fully automated Thermo Scientific™ KingFisher™ Flex Magnetic Particle Processor (Cleveland, OH). This material was used as the input sample for library construction. DNA libraries were prepared using the NexteraXT™ library construction protocol (Illumina, San Diego, CA) following the manufacturer's instructions and sequenced on a MiSeq Sequencer (JMI Laboratories). The assembled genome was utilized for extracting serotyping 23 and multilocus sequence typing (MLST) 24 information, and for analysis of the deduced amino acid sequences of MurM and PBPs compared with those of reference strain R6.
Results
The most frequently occurring NS phenotypic patterns are presented in Table 1 and were seen with erythromycin (45.8%), followed by MDR (28.8%), TMX (27.6%), amoxicillin–clavulanate (10.5%), ceftriaxone (5.3%), levofloxacin (1.6%), and penicillin (0.4% at MIC, ≥8 μg/ml [resistant parenteral, nonmeningitis breakpoint]; 6.3% at MIC, ≥4 μg/ml [intermediate parenteral, nonmeningitis breakpoint; Table 2]).
MDR, multidrug-resistant, defined as NS to ≥2 classes of the following antimicrobials: penicillin (≥4 μg/ml), ceftriaxone, erythromycin, levofloxacin, tetracycline, and trimethoprim–sulfamethoxazole.
MIC, minimal inhibitory concentration; NS, nonsusceptible.
% S = % susceptible and % R = % resistant according to CLSI criteria. 22
Using nonmeningitis breakpoints. 22
Using meningitis breakpoints. 22
Using oral breakpoints. 22
Using parenteral, nonmeningitis breakpoints. 22
Breakpoints from USA-FDA Package Insert. 37
CLSI, Clinical and Laboratory Standards Institute; FDA, Food and Drug Administration.
Ceftaroline was very active against the 2,614 isolates of S. pneumoniae (MIC50/90, ≤0.015/0.12 μg/ml): all but one isolate (>99.9% susceptible) was susceptible at the CLSI breakpoint of ≤0.5 μg/ml (Table 1). The ceftaroline-NS isolate (853008) was collected from a 1-year-old patient from Galveston, Texas, with an upper respiratory tract infection and was MDR with an MIC value of 1 μg/ml for ceftaroline, 8 μg/ml for penicillin and ceftriaxone, 8 μg/ml for erythromycin, >4 μg/ml for TMX, >8 μg/ml for amoxicillin–clavulanate, and 1 μg/ml for meropenem.
For the antimicrobial agents listed in Table 2, high rates of susceptibility were seen with ceftaroline (>99.9%), ceftriaxone (94.7% susceptible at the nonmeningitis breakpoint [≤1 μg/ml]), penicillin (93.7%, susceptible at the parenteral nonmeningitis breakpoint [≤2 μg/ml]), levofloxacin (98.4%), linezolid (100.0%), tigecycline (100.0%), and vancomycin (100.0%). Ceftaroline (MIC90, 0.12 μg/ml) was eightfold more potent than ceftriaxone (MIC90, 1 μg/ml), 16-fold more potent than penicillin (MIC90, 2 μg/ml), and 32-fold more potent than amoxicillin–clavulanate (MIC90, 4 μg/ml). Ceftaroline retained activity against all of the drug-resistant subsets, including 99.3% of ceftriaxone-NS isolates and 99.9% of MDR isolates (Table 2). Ceftaroline MIC values were slightly elevated for penicillin-resistant (MIC, ≥8 μg/ml) isolates (MIC50/90, 0.25/0.5 μg/ml; 90.0% susceptible).
Among isolates of MDR S. pneumoniae, susceptibilities to ceftriaxone (81.5%; MIC, ≤1 μg/ml [nonmeningitis breakpoint]), penicillin (78.5%; MIC, ≤2 μg/ml [parenteral nonmeningitis breakpoint]), amoxicillin–clavulanate (70.9%), erythromycin (2.3%), tetracycline (29.1%), and TMX (25.0%) were markedly reduced (Table 2). Levofloxacin (MIC50/90, 1/1 μg/ml; 96.3% susceptible) and ceftaroline (MIC50/90, 0.06/0.25 μg/ml; 99.9% susceptible) were the only agents with useful activity against MDR isolates.
The ceftaroline-NS isolate (853008) was serotype 35B and had an MLST profile (ST—18-12-4-44-14-77-91) that was a single-locus variant of ST377 (ST—18-12-4-44-14-77-93) or ST558 (ST—18-12-4-44-14-77-97). Figure 1 shows the PBP amino acid sequences of reference strain R6 and clinical isolate 853008. Numerous alterations were observed within the PBP1a transpeptidase domain of clinical isolate 853008 when compared with R6, including a T371A mutation within the active motif. However, the other two active motifs showed wild-type sequences. Similarly, a total of 26 modifications were detected within the PBP2b transpeptidase domain of 853008 compared with the reference strain. All STMK, SSN, and SVVK motifs were intact. There were also 41 alterations within the PBP2x transpeptidase domain of clinical isolate 853008 compared with reference strain. These mutations included T338A and M339F within the STMK motif. Other PBP2x motifs (SSN and KSG) within the subjected isolate were identical to R6. Other PBPs from isolate 853008 had a small number of amino acid changes relative to R6: PBP1b (N645T); PBP2a (T354I, S461A, V586I, and P656S); and PBP3 (I321T) (data not shown). MurM of isolate 853008 had 31 amino acid modifications compared with R6, and all substitutions were located within amino acids 6 to 131 (data not shown).
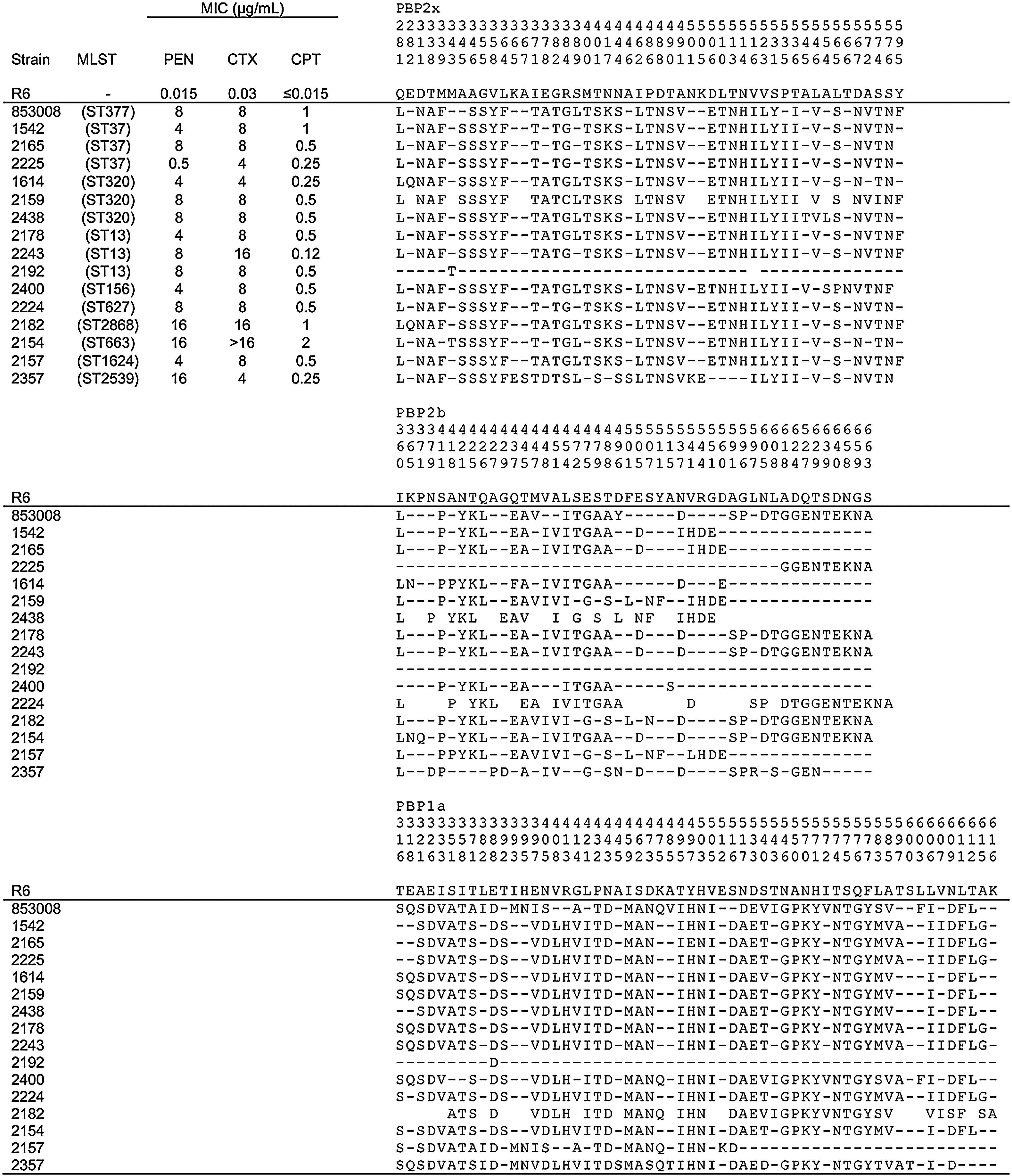
Deduced amino acid sequences of the transpeptidase portion of the PBP2x, PBP2b, and PBP1a proteins from reference strain R6 and clinical isolate 853008. Sequences and MIC results (personal communication) for 15 other clinical isolates were obtained from McGee et al. 16 Dashes indicate residues identical to those of R6. Amino acids are numbered vertically according to their positions in the protein. Adapted from McGee et al. 16 . PBP, penicillin-binding protein; MIC, minimal inhibitory concentration.
Discussion
The AWARE Surveillance Program provides contemporary and longitudinal information on the activity of ceftaroline and comparator antimicrobial agents against S. pneumoniae and other bacterial pathogens collected from episodes of CABP, HCABP, BSI, and other infection types in hospitalized patients since 2008.4,11 As seen in this analysis, the frequency of NS for ceftaroline against S. pneumoniae is extremely low (<0.1%) and has not changed over the time period from 2008 to the present (data not shown). The yearly frequency (2008–2014) of resistant phenotypes of S. pneumoniae observed in the AWARE Program is shown in Table 3 and depicts a steady decline in the rates of NS to ceftriaxone, penicillin, and TMX and a trend toward increasing NS to erythromycin and levofloxacin. The frequency of MDR-SP also shows a decline over time from a peak of 33.6% in 2011 to 28.8% in 2014 (Table 3). These data span the introduction of PCV13 and ceftaroline (in 2010), both of which may have had an influence on the pneumococcal resistance rate.
MIC ≥4 μg/ml.
AWARE, Assessing Worldwide Antimicrobial Resistance Evaluation; TMP-SMX, trimethoprim–sulfamethoxazole.
The clinical isolate 853008 was serotype 35B and showed an MLST profile (single variant of ST377 or ST558) associated with clonal complex 558. These isolates are also known as PMEN clone Utah35B-24 (ST377). 25 The prevalence of this clone has increased in the United States during the years after PCV7 and PCV13 implementation and these isolates are usually associated with decreased susceptibility to penicillin.26,27 The increased prevalence of isolates related to this clone was also reported in Canada. 28 The isolate 853008 exhibited multiple mutations in PBP1a, PBP2b, and PBP2x that are associated with increased MIC results to β-lactam agents, which are because of successive point mutations and/or mosaic structures within the PBPs, including conserved motifs. 29
The combination of several alterations drives the level of resistance; usually, modifications in PBP2b and PBP2x cause a low level of β-lactam resistance, whereas additional mutations in PBP1a are needed for high-level resistance, as was observed in the clinical isolate 853008. 30 This isolate showed alterations known to be relevant for β-lactam resistance, such as T338A, M339F, and M400T in PBP2x. 29 T338A and M339F are within the STMK motif of PBP2x and have been implicated in resistance to penicillin, whereas alterations at M400 were associated with resistance to cefotaxime. 31 Isolate 853008 also demonstrated several alterations within PBP2b, including T445A adjacent to the S442SN conserved motif and numerous alterations close to the following K614TG motif. Alterations near K614TG were proposed to be essential for high-level amoxicillin resistance, but have not previously been associated with resistance to extended-spectrum cephalosporins. 32 Similarly, changes in PBP1a at T371 (S370TMK motif) and within each position of the T574SQF motif have previously been associated with penicillin resistance, and all were observed within the PBP1a of isolate 853008. 16 Finally, it has also been previously documented that, in addition to alterations in PBP1a, PBP2b, and PBP2x, substitutions in MurM (between amino acids 1 and 131) are needed for high-level resistance to penicillin and cephalosporins in S. pneumoniae in some isolates. 33 Consistent with that finding, the MurM sequence from isolate 853008 investigated here had 92.4% identity to that of R6 and all amino acid alterations were located in the first third portion of the protein.
A previous study investigated the activity of ceftaroline against 120 S. pneumoniae clinical isolates. exhibiting cefotaxime MIC values ≥4 μg/ml. 16 This study reported ceftaroline MIC50 and MIC90 results of 0.5 and 0.5 μg/ml, respectively, and a select group of isolates (ceftaroline MIC, 0.12–2 μg/ml) had their PBP1a, PBP2b, and PBP2x genes sequenced (Fig. 1). The vast majority of these isolates shared numerous modifications in PBP1a, PBP2b, and PBP2x with isolate 853008. For PBP1a, these included T371A (S370TMK motif), P432T (close to the S428RN motif), I459M, S462A, D473N (surrounding the S466SN motif), and several alterations surrounding the T574SQ. These isolates also shared mutations in PBP2b at T445A (next to S442SN motif) and several alterations surrounding the K614TG motif, as well as T338A, M339F (at the S337TMK motif), M400T (next to the S395SN motif), and L546V (next to the K557SG motif) in PBP2x.
As the β-lactam resistance phenotypes, including those against third generation cephalosporins, are dependent on the accumulation of amino acid changes in PBPs, it can be speculated that the same association may be true for newer molecules, such as ceftobiprole and ceftaroline. In fact, a previous study associated higher MIC values for ceftobiprole (0.5–1 μg/ml) in S. pneumoniae with greater number of alterations in PBPs, more specifically in PBP2x. 34 These isolates with higher ceftobiprole MIC values showed the same alterations in the conserved motifs of PBP2x (i.e., T338A, M339F, I371T, R384G, and L546V) as those observed in isolate 853008 34 ; among all PBPs, PBP2x has been demonstrated to have the highest affinity for ceftaroline 15 and ceftobiprole. 35
However, in contrast to the mentioned hypothesis, McGee et al. 16 described an isolate (#2192) exhibiting elevated MIC values for penicillin (8 μg/ml), cefotaxime (8 μg/ml), and ceftaroline (0.5 μg/ml) with virtually no amino acid substitutions within PBP1a, PBP2b, and PBP2x (Fig. 1). This indicates that resistance mechanisms other than alterations in PBPs, such as mutations in MurM, may also be responsible for higher MIC results for penicillins and cephalosporins, including newer cephalosporins. In fact, it has been demonstrated that increases in the ceftaroline MIC values in S. aureus can also be because of substitutions in non-PBP genes. 36
In summary, ceftaroline was very active against S. pneumoniae from U.S. medical centers, including MDR isolates and isolates NS to ceftriaxone and other antimicrobial agents commonly used to treat CABP. Ceftaroline has consistently retained potency against isolates obtained after its introduction for clinical use in the United States. A single NS-ceftaroline MIC value was obtained from an S. pneumoniae isolate with serotype 35B, and other isolates associated with this serotype have been previously demonstrated to exhibit a decreased susceptibility to β-lactam agents, including penicillin and ceftriaxone. 2 This may suggest that β-lactam binding to the PBP target sites is intrinsically reduced in isolates from this serotype and fewer mutational steps may be needed to decrease β-lactam binding, even by more potent and newer cephalosporin agents. Importantly, however, the in vitro data presented here confirm that the potency of ceftaroline against S. pneumoniae is higher than that exhibited by other β-lactams, including against isolate subsets exhibiting ceftriaxone-NS and MDR phenotypes.
Footnotes
Acknowledgments
The authors thank all participants of the AWARE Program for providing bacterial isolates: Arkansas Children's Hospital (Little Rock, AR), Miller Children's Hospital (Long Beach, CA), University of Colorado Hospital (Aurora, CO), Sacred Heart Hospital (Pensacola, FL), Tampa General Hospital (Tampa, FL), Children's Healthcare of Atlanta (Atlanta, GA), Clinical Laboratories of Hawaii (Ewa Beach, HI), Iowa Methodist Medical Center (Des Moines, IA), Indiana University Health, Methodist Hospital (Indianapolis, IN), University of Louisville Hospital (Louisville, KY), University of Kentucky Hospital (Lexington, KY), VA Healthcare System of Boston (Boston, MA), Lahey Clinic (Burlington, MA), Henry Ford Health System (Detroit, MI), Childrens Mercy Hospital (Kansas City, MO), Alegent-Creighton Laboratory (Omaha, NE), Robert Wood Johnson Medical School (New Brunswick, NJ), Columbia Presbyterian Medical Center (New York, NY), University of Rochester Medical Center (Rochester, NY), New York Presbyterian Hospital (New York, NY), Summa Health System (Akron, OH), University of Texas Medical School (Houston, TX), UTMB Health (Galveston, TX), University of Utah Medical Center (Salt Lake City, UT), University of Virginia Health System (Charlottesville, VA), Fletcher Allen Health Care (Burlington, VT), University of Washington Medical Center (Seattle, WA), Seattle Children's Hospital (Seattle, WA), and Children's Hospital of Wisconsin (Milwaukee, WI). This study was supported by Allergan plc, Dublin, Ireland. Allergan was involved in the design and decision to present these results and JMI Laboratories received compensation fees for services in relation to preparing the article. Allergan had no involvement in the collection, analysis, and interpretation of data.
Disclosure Statement
JMI Laboratories, Inc. has received research and educational grants in 2014–2015 from Achaogen, Actavis, Actelion, American Proficiency Institute, AmpliPhi, Anacor, Astellas, AstraZeneca, Basilea, Bayer, BD, Cardeas, Cellceutix, CEM-102 Pharmaceuticals, Cempra, Cerexa, Cidara, Cormedix, Cubist, Debiopharm, Dipexium, Dong Wha, Durata, Enteris, Exela, Forest Research Institute, Furiex, Genentech, GSK, Helperby, ICPD, Janssen, Lannett, Longitude, Medpace, Meiji Seika Kasha, Melinta, Merck, Motif, Nabriva, Novartis, Paratek, Pfizer, Pocared, PTC Therapeutics, Rempex, Roche, Salvat, Scynexis, Seachaid, Shionogi, Tetraphase, The Medicines Co., Theravance, ThermoFisher, VenatoRX, Vertex, Wockhardt, Zavante, and some other corporations. Some JMI employees are advisors/consultants for Allergan, Astellas, Cubist, Pfizer, Cempra, and Theravance. In regard to speakers bureaus and stock options, none to declare.