
Abstract
Given that tigecycline-based combination therapy is recognized as a valuable option for the treatment of tigecycline-resistant Acinetobacter baumannii, we conducted this systematic review and meta-analysis to assess the overall evidence of its effectiveness. The synergy rate was defined as the primary outcome that was calculated separately for time-kill, Etest, and checkerboard microdilution methods. The secondary outcomes were bactericidal activity and the efficacy of combination treatment on the development of resistance. In total, 37 published papers and 16 conference proceedings were included. Nine classes consisting of 22 antibiotic types in combination with tigecycline against 1,159 A. baumannii strains were reported in the analysis. For the time-kill studies, combination therapy showed a synergy rate of 37.9% (95% confidence interval [CI], 30.7–46.5); the highest synergy rate was 67.4% (95% CI, 27.3–91.9) for tigecycline in combination with colistin. Moreover, combination with amikacin or colistin could efficiently inhibit the development of tigecycline resistance. Compared with checkerboard microdilution and Etest methods, time-kill studies always showed higher synergy rates. Altogether, these results suggest that the in vitro tigecycline-based combinations resulted in moderate synergy rates and that several combinations could suppress the resistance of A. baumannii to tigecycline, which should be further confirmed in animal models and clinical trials.
Introduction
A
Tigecycline, which was approved by the FDA in June 2005, is a novel intravenous glycylcycline antibiotic with broad-spectrum activities against many gram-positive bacteria, gram-negative bacteria, and anaerobes. 4 It is considered a last-resort antibiotic for the treatment of multidrug-resistant A. baumannii. 5 However, the incidence of tigecycline resistance in A. baumannii mainly associated with efflux pump overexpression has been increasingly reported.6–9 To reduce the emergence of resistant strains and improve clinical outcomes, tigecycline-based combination therapies are considered a practical strategy against multidrug-resistant A. baumannii. 10
In vitro combination studies can be considered a basic reference for clinical treatments. Although many in vitro experiments have been performed by using tigecycline in combination with other antibiotics against A. baumannii, no comprehensive meta-analysis study has yet been conducted. To provide guidelines for clinical rational drug use, we systematically searched and analyzed four mainstream databases and some conference proceedings to evaluate the in vitro synergistic activity of tigecycline in combination with other antibiotics against A. baumannii.
Methods
Literature search and selection criteria
A systematic literature search of PubMed, Embase, Medline, and Web of Science was conducted by two separate reviewers, without limits on the publication date, language, region, or publication status. Furthermore, the conference proceedings from the Infectious Diseases Society of America (IDSA), Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC), and European Congress of Clinical Microbiology and Infectious Diseases (ECCMID) for the years 2007–2014 were also reviewed. The search term strategy was as follows: (tigecycline OR glycylcycline OR tygacil) AND (Acinetobacter baumannii OR baumannii OR A. baumannii) AND (in vitro OR combination OR checkerboard OR time-kill OR Etest OR microdilution OR agar dilution OR susceptibility). To reduce the search bias, the related articles function was selected, and references from the target articles were also examined to identify articles potentially missing from the database searches.
All available in vitro synergy experiments involving tigecycline combinations were included in this article. Studies using more than two antibiotics or that marketed antibiotics not available globally were excluded.
Outcomes
The in vitro synergy effect on bacterial death or inhibition was the primary outcome. For time-kill tests, synergy was defined as a ≥2 log10 decrease in CFU/ml compared with that for treatment with the most efficient antibiotic alone, whereas antagonism was defined as a ≥2 log10 CFU/ml increase. For the checkerboard microdilution and Etest methods, synergy was defined by means of the fractional inhibitory concentration index (FICI): FICI = (MICAB/MICA) + (MICBA/MICB), where MICAB and MICBA are the minimum inhibitory concentrations (MICs) of drugs A and B tested in combination, and MICA and MICB are the MICs of drugs A and B tested alone. The FICI value was interpreted as follows: ≤0.5, synergy; 0.5–1, additive; 1–4, indifference; and >4, antagonism. The bactericidal effect was defined as a ≥3 log10 reduction in the number of colonies compared with the pretreatment counts. The in vitro bactericidal activity was the secondary outcome.
Data extraction
Data were independently extracted by two authors, using a premade extraction form. For each study, the following information was extracted: (a) susceptibility to tigecycline, (b) testing methods, (c) total number of isolates tested, (d) the types of antibiotics, (e) publication year, and (f) the first author. The breakpoints for tigecycline were not identified by the Clinical and Laboratory Standards Institute (CLSI); susceptible and resistant were defined as follows: susceptible, suscepti resistant, ≥8 mg/L. 11
Statistical synthesis of data
The synergy rates with a 95% confidence interval (CI) were calculated separately for each test method, where the number of isolates tested was classified as the sample size, and the event was synergy. The results of each test method were divided by antibiotic type and resistance to tigecycline. Some studies performed multiple tests on the same antibiotic combinations and the same bacterial populations; we selected the most common drug concentration or bacterial load. All statistical synthesis was conducted with Comprehensive Meta-Analysis v.2.0 (Biostat, Inc., Englewood, NJ). We calculated event rates by both fixed- and random-effects models. Heterogeneity was assessed by I2; 0% suggests no observed heterogeneity, whereas larger values suggest that heterogeneity exists. We chose the fixed-effects model when substantial heterogeneity was not present; otherwise, the random-effects model was used (I2 > 50%).
Results
Our search strategy yielded 1,507 potentially relevant articles (Fig. 1). After our screening, 37 published studies and 16 conference proceedings satisfied the selection criteria. The characteristics of the included studies are described in Table 1. In total, 1,159 A. baumannii strains were tested, involving 28 Etests, 54 checkerboard microdilution tests, and 60 time-kill assays with 22 antibiotic types.
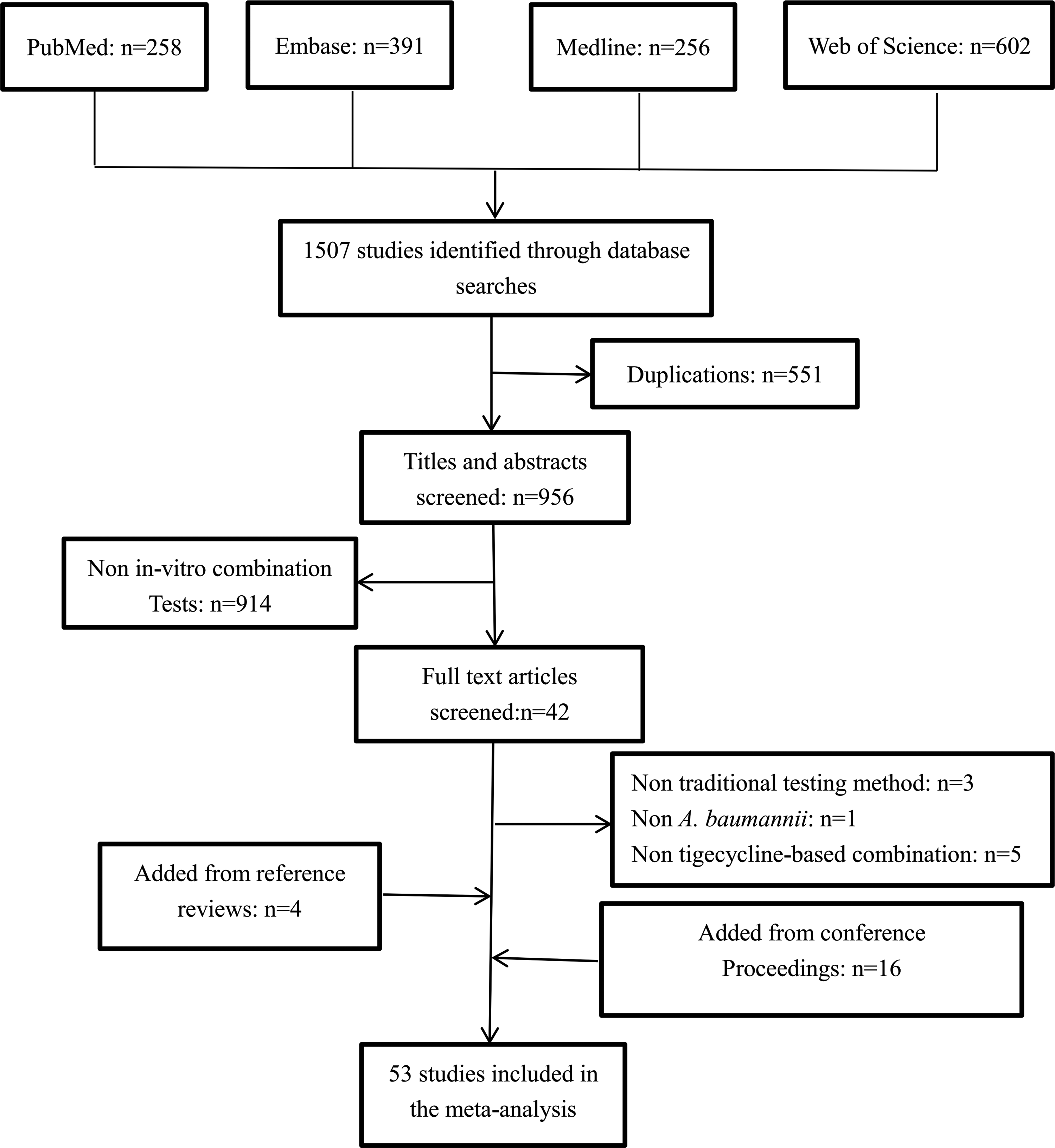
Flow diagram of literature selection.
Breakpoints for tigecycline were defined as follows: susceptible (S) ≤2 mg/L; 2 mg/L<intermediate (I) <8 mg/L; resistant (R) ≥8 mg.
b, bactericidality; ECCMID, European Congress of Clinical Microbiology and Infectious Diseases; FICI, fractional inhibitory concentration index; ICAAC, Interscience Conference on Antimicrobial Agents and Chemotherapy; IDSA, Infectious Diseases Society of America; PK/PD, pharmacokinetic/pharmacodynamic; Tks, time-kill synergy.
Synthesis of time-kill data
For tigecycline-carbapenem combinations (Fig. 2), 10 studies performed on 92 A. baumannii isolates yielded a synergy rate of 26.1% (95% CI, 12.9–45.7). None of the isolates showed antagonism. The bactericidal rate for the 49 isolates increased from 6.0% (95% CI, 1.9–17.0) for the most active single antibiotic to 36.2% (95% CI, 23.1–51.7) for the combination treatments. The heterogeneity (I2) was 56.7% for these studies. Doripenem displayed the lowest synergy rate of 7.2% (95% CI, 10.0–37.3). Meropenem and imipenem showed synergy rates of 32.5% (95% CI, 5.8–78.8) and 33.3% (95% CI, 14.3–59.8), respectively. However, it should be noted that the synergy data from doripenem and meropenem are not reliable because they were both only examined in two studies.
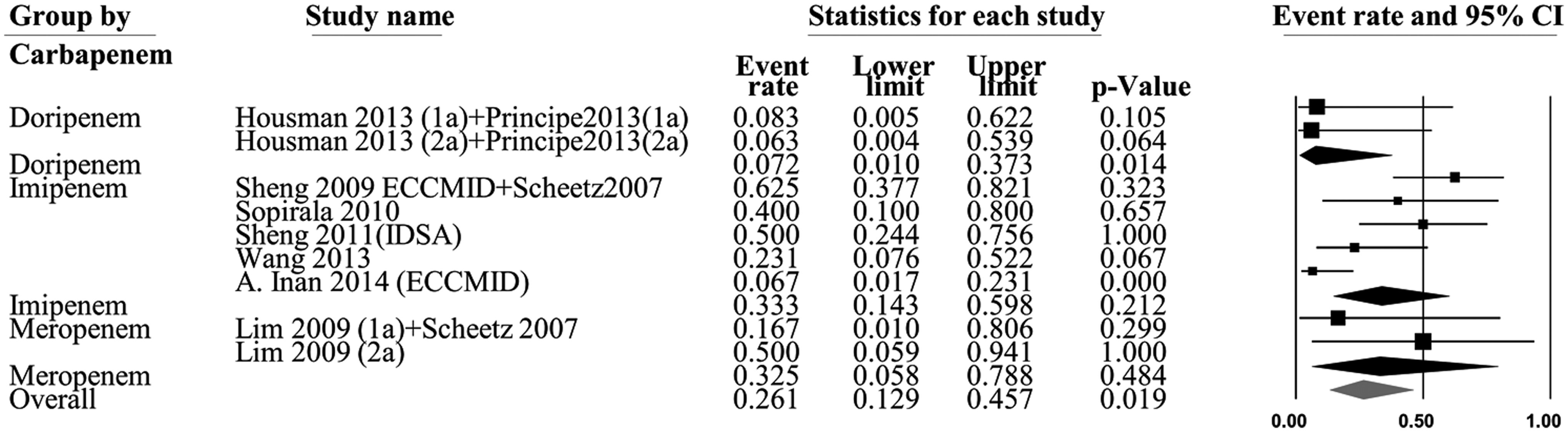
Forest plot of tigecycline–carbapenem combinations in time-kill assay. Subgroups according to antibiotic resistance profile and types of carbapenem are listed separately. CI, confidence interval.
For tigecycline-rifampicin combinations (Fig. 3), nine studies examining 119 isolates yielded a synergy rate of 30.1% (95% CI, 12.1–57.5), whereas one isolate was antagonistic, with an antagonism rate of 6.2% (95% CI, 2.6–14.3). The rates of bactericidal activity for the 96 isolates increased from 1.5% (95% CI, 0.3–7.3) for the best single antibiotic to 24.3% (95% CI, 16.7–33.9) for the combination treatments. The heterogeneity (I2) for these studies was 65.8%.

Forest plot of tigecycline–rifampicin combinations in time-kill assay. Subgroups according to antibiotic resistance profile are listed separately.
For tigecycline–polymyxin combinations (Fig. 4), 15 studies examining 133 isolates yielded a synergy rate of 36.3% (95% CI, 22.6–52.6); no isolates were antagonistic. The bactericidal activity of the 200 isolates increased from 14.2% (95% CI, 6.3–28.9) for the single most active agent to 60.2 (95% CI, 40.0–77.4) for the combination treatments. The heterogeneity (I2) was 51.4%. The synergy rate of colistin was 67.4% (95% CI, 27.3–91.9), which was higher than that of polymyxin B (31.1% [95% CI, 18.8–46.8]). Regarding bactericidal activity, colistin was also more effective than polymyxin B.
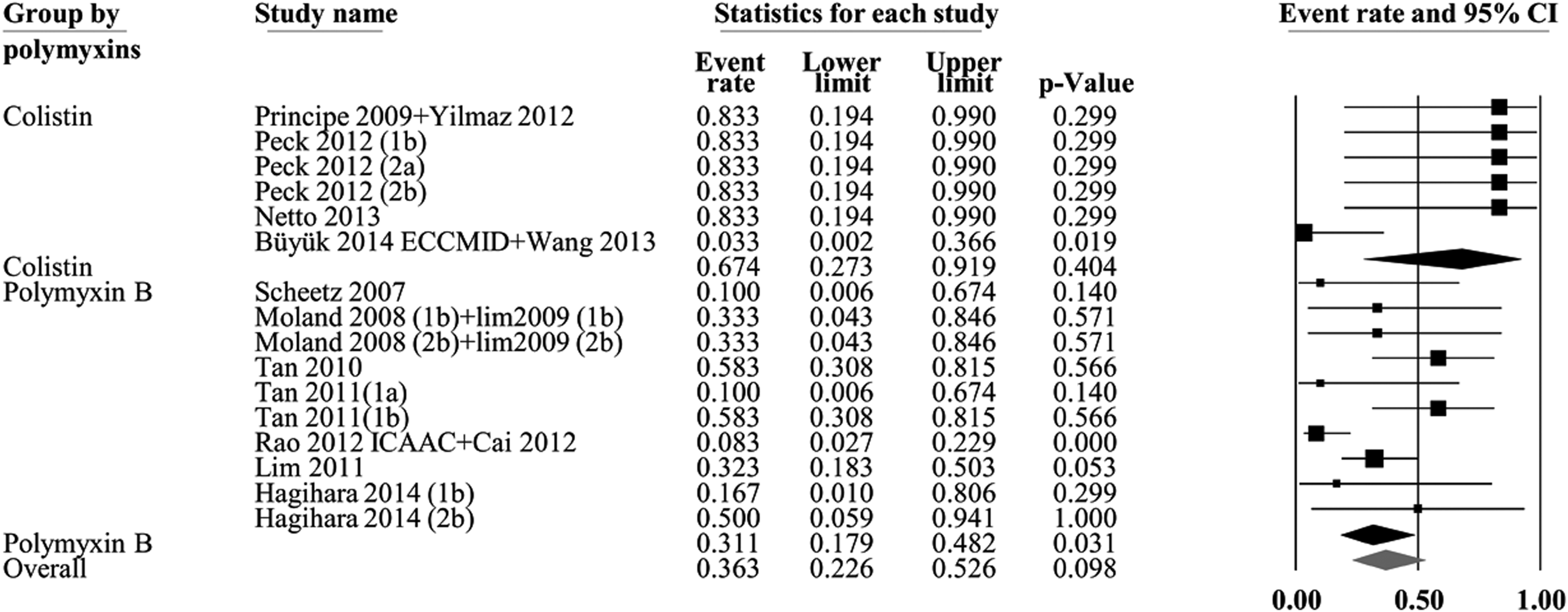
Forest plot of tigecycline–polymyxin combinations in time-kill assay. Subgroups according to antibiotic resistance profile and types of polymyxins are listed separately.
For tigecycline-amikacin combinations, four studies were performed on 16 isolates, yielding a synergy rate of 18.8% (95% CI, 1.9–73.6). No isolates were antagonistic. Rates of bactericidal activity for the three isolates increased from 12.5% (95% CI, 0.7–73.4) for treatments with the most active antibiotic by itself to 33.3% (95% CI, 4.3–84.6) for combination treatments. Heterogeneity (I2) was 53.2%.
Evaluations of the in vitro synergy of tigecycline in combination with other antibiotic classes were demonstrated in five studies. Two of them that included five strains evaluated the tigecycline-ampicillin/sulbactam combination, which showed no synergy. The tigecycline-cefoperazone/sulbactam combination was performed on four strains in one study and showed a high synergy rate of 50%. In addition, two studies tested tigecycline in combination with ciprofloxacin or levofloxacin, which showed negative synergistic activity.
When investigating tigecycline-resistant strains (16 studies on 180 strains), the overall synergy rate was 36.3% (95% CI, 22.1–53.4), which was lower than that of the susceptible strains (50.7% [95% CI, 36.4–64.8] in 18 studies involving 58 strains).
The antibiotics concentration ranges in the time-kill studies were as follows: tigecycline, 0.06–16 mg/L; imipenem, 4–256 mg/L; meropenem, 4–64 mg/L; doripenem, 4–16 mg/L; amikacin, 0.5–64 mg/L; polymyxin B, 0.25–20 mg/L; colistin, 0.25–128 mg/L; and ampicillin/sulbactam, 4/2–256/128 mg/L. On the other hand, clinically achievable antibiotics concentrations were 2 mg/L for polymyxin B, rifampicin, and tigecycline, which correspond to maximum intravenous doses of at least 1 million units of polymyxin B, 600 mg of rifampicin, and 100 mg of tigecycline administered every 12 hr.64–66 The concentration of imipenem was 32 mg/L, which represents the steady-state free peak concentration arising from 1 g (40-min infusion). 67 The meropenem concentration was 64 mg/L, simulating a steady-state free peak concentration arising from 2 g (3-hr infusion). 68 The doripenem concentration was 13 mg/L, corresponding to the steady-state free peak concentration arising from 1 g (4-hr infusion). 69 Notably, some of the antibiotics showing positive synergy had a higher concentration than serum or tissue drug concentrations. Specifically, there were three studies that reported clinically unavailable concentrations, with positive synergy among all 26 time-kill studies in this review.
Synthesis of checkerboard microdilution data
The tigecycline-carbapenem combinations were tested in 12 studies with 237 isolates, yielding a pooled synergy rate of 24.3% (95% CI, 15.3–36.3) (Fig. 5). Testing of tigecycline-meropenem combinations in one study examining 13 isolates yielded a synergy rate of 46.2% (95% CI, 22.4–71.8). Imipenem and doripenem showed synergy rates of 19.2% (95% CI, 10.4–32.7) and 10.8% (95% CI, 1.6–47.6), respectively. No isolates were antagonistic. The heterogeneity (I2) was 64.6%.

Forest plot of tigecycline–carbapenem combinations in checkerboard microdilution method. Subgroups according to antibiotic resistance profile and types of carbapenem are listed separately.
For tigecycline-polymyxins combinations, 385 isolates in 18 studies showed a pooled synergy rate of 12.5% (95% CI, 8.8–17.4) (Fig. 6). Polymyxin B and colistin individually showed synergy rates of 23.9% (95% CI, 12.3–41.2) and 10.1% (95% CI, 6.7–14.9), respectively. Three isolates were antagonistic, with a rate of 5.0% (95% CI, 2.8–8.7). The heterogeneity (I2) was 42.3%.
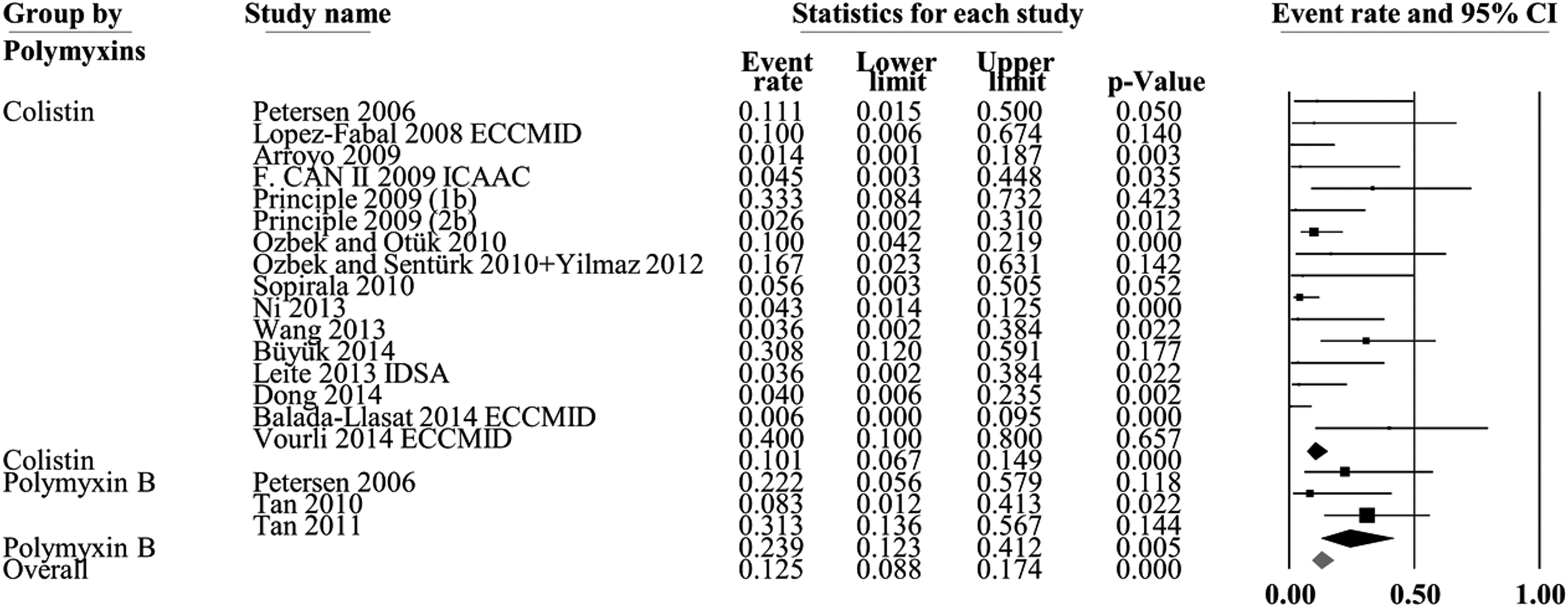
Forest plot of tigecycline–polymyxin combinations in checkerboard microdilution method. Subgroups according to antibiotic resistance profile and types of polymyxins are listed separately.
For tigecycline-rifampicin combinations (Fig. 7), seven studies with 181 isolates showed that the synergy rate was 19.5% (95% CI, 10.8–32.8). Two isolates were antagonistic, with a rate of 3.7% (95% CI, 1.5–8.5). The heterogeneity (I2) was 56.1%.

Forest plot of tigecycline–rifampicin combinations in checkerboard microdilution method. Subgroups according to antibiotic resistance profile are listed separately.
Six studies were conducted on 73 isolates for the tigecycline-amikacin combinations, which yielded a synergy rate of 22.2% (95% CI, 12.1–37.1). No isolates were antagonistic. The heterogeneity (I2) was 48.2%.
Five studies involving 185 isolates were treated with tigecycline–sulbactam combinations, yielding a synergy rate of 9.5% (95% CI, 6.0–14.8). Tigecycline-ampicillin/sulbactam combinations were tested in two studies with 33 isolates, yielding a synergy rate of 6.9% (95% CI, 1.7–23.8). The combinations of tigecycline and cefoperazone/sulbactam were tested in two studies with 110 isolates, yielding a synergy rate of 8.8% (95% CI, 0.3–73.3). The random-effects model was used in these studies owing to the high heterogeneity (I2 = 82.5%). Tigecycline-piperacillin/tazobactam combinations were tested in two studies with 33 strains, which yielded a synergy rate of 12.4% (95% CI, 3.9–32.8). Two studies involving 22 strains were treated with a combination of tigecycline-ciprofloxacin, and two studies that tested 30 strains with tigecycline-levofloxacin combinations showed synergy rates of 6.7% (95% CI, 1.3–27.2) and 30.6% (95% CI, 11.7–59.5), respectively. Several studies tested tigecycline in combination with moxifloxacin or ceftriaxone, and synergistic activity was found in 5/13 and 4/10 strains, respectively. No synergistic activity was observed for tigecycline combined with azithromycin, chloramphenicol, or erythromycin.
When investigating tigecycline-resistant strains (13 studies on 176 strains), the overall synergy rate was 21.0% (95% CI, 14.6–29.4), which was similar to that of the susceptible strains (24.2% [95% CI, 19.5–29.6], from 22 studies on 343 strains).
Synthesis of Etest data
Three studies with 39 isolates treated with tigecycline-carbapenem combinations yielded a synergy rate of 84.1% (95% CI, 18.5–99.2); the random-effects model was chosen for these studies owing to their high heterogeneity (I2 = 83.0%). Four studies on 100 isolates involving tigecycline-rifampicin combinations reported a synergy rate of 6.6% (95% CI, 2.6–15.7). Twelve studies with 293 isolates were tested with tigecycline-polymyxins combinations and resulted in a synergy rate of 8.1% (95% CI, 3.0–20.1); the random-effects model was used in these studies given their high heterogeneity (I2 = 87.7%). Two studies involving 21 isolates examined tigecycline-amikacin combinations, yielding a synergy rate of 6.9% (95% CI, 1.4–28.0). Synergistic activity of tigecycline in combination with gentamicin or ampicillin/sulbactam was shown in 17/42 and 1/17 strains, respectively. No synergy was observed for tigecycline-azithromycin combinations.
When investigating tigecycline-resistant strains (five studies involving 38 strains), the overall synergy rate was 16.1% (95% CI, 2.1–63.4), which was higher than that in the susceptible strains (2.4% [95% CI, 0.1–28.7], two studies involving 20 strains).
Combination effect on the development of antibiotic resistance
The effects of tigecycline-based combinations on antibiotic resistance were reported in three studies. Moland et al. demonstrated that tigecycline and amikacin alone could inhibit growth of a tigecycline-resistant isolate for 4 hr, then the inhibition was followed by regrowth; however, tigecycline in combination with amikacin could successfully suppress the emergence of resistant populations. 16 Ozbek and Sentürk. found that tigecycline in combination with colistin or levofloxacin delayed or prevented the emergence of resistance and showed synergistic interaction against A. baumannii. 25 Ni et al. observed that tigecycline-colistin and tigecycline-sulbactam combinations can reduce the mutant prevention concentrations of tigecycline, which means that the combination could effectively restrict the selection of antibiotic-resistant mutant strains. 48
Discussion
Tigecycline has played an important role in combating a variety of bacteria, especially A. baumannii, which ranks among the most deleterious nosocomial pathogens and is prevalent worldwide. Unfortunately, the incidence of tigecycline-resistant A. baumannii mainly associated with efflux pump overexpression has been increasingly reported over the past decade. Under such circumstances, tigecycline-based combinations are frequently in clinical use. This review demonstrated that the combination of tigecycline with other antibiotics can display different synergy effects against A. baumannii in vitro. Although these in vitro test results cannot be directly linked to clinical outcome owing to several factors such as the PK/PD property of the antibiotic, bacteria isolate, antibiotic concentration at the infection site, and potential differences in host immune interactions between in vivo and in vitro experiments, they still can be considered an indication of in vivo efficiency.
For the time-kill assays, tigecycline-colistin combinations showed the highest synergy rate of 67.4% (95% CI, 27.3–91.9), which may be attributed to a mechanism involving permeability change in the electrostatic binding of colistin to the outer membrane of A. baumannii. However, for combinations of tigecycline and polymyxin B, a homolog of colistin, the synergy rate dropped to 31.1% (95% CI, 17.9–48.2), revealing that polymyxin B has worse synergistic activity owing to its attenuated effect on outer membrane permeability. As antibiotics that block bacterial protein synthesis, rifampicin and amikacin showed moderate synergy rates in combination with tigecycline owing to their cooperation at different steps of the protein synthesis process. Carbapenem, an inhibitor of the bacterial cell wall that acts by binding to penicillin-binding proteins, could result in increased uptake of tigecycline, which also demonstrated moderate synergy rates. Notably, the bactericidal activity shown in the combination tests (24.3–50.2) was considerably higher compared with that in monotherapy (1.5–14.2).
To further investigate the optimal treatment combination, we analyzed the overall data of tigecycline in combination with other antibiotics. The pooled synergy rate for tigecycline-carbapenem treatments was 26.8% (95% CI, 16.6–40.3), and the rate for tigecycline-colistin was 17.9% (95% CI, 12.2–25.3). For tigecycline-rifampicin and tigecycline-amikacin combinations, the pooled synergy rates were 18.3 (95% CI, 11.0–29.0) and 19.6% (95% CI, 11.5–31.4), respectively.
As shown in this review, the synergy rate for the time-kill method was generally higher than those obtained by checkerboard microdilution and Etest methods. This effect has also been reported in other studies. 70 Among three studies27,34,51 that have applied the three testing methods to the same strains, the time-kill method demonstrated synergy rates of 56%, 40%, and 64%, respectively. In contrast, the checkerboard microdilution method resulted in synergy rates of 8.3%, 17%, and 17.9%, respectively. For the Etest method, the synergy rates were 0%, 2%, and 20.5%, respectively. However, in one study, 49 the synergy rate resulting from the time-kill method was lower than that obtained by the checkerboard microdilution method. Nevertheless, discordance is reasonable given that these methods use different judgment standards. As clinically available methods, the checkerboard microdilution and Etest methods only provide an MIC value, whereas the time-kill method can also provide an evolution graph showing the interaction between bacteria and antibiotics. However, it is not yet known as to which method can better predict in vivo activity. Therefore, an optimal method with universal standardization would be highly beneficial.
The overall synergy rate of tigecycline-resistant strains was 24.7% (95% CI, 16.7–35.0), which was slightly lower than that of the sensitive strains (27.9% [95% CI, 23.2–33.1]). Some studies have demonstrated that the excessive expression of AdeFGH, AdeIJK, and AdeABC could lead to resistance of A. baumannii to tigecycline.71–73 Efflux pumps in the resistant strains could reduce the intracellular antibiotic concentration, thereby resulting in a lower synergy rate.
In summary, combination tests of tigecycline with various antibiotics showed moderate-to-high in vitro bactericidal activity and a moderate synergy rate against A. baumannii. Several antibiotics, such as amikacin, colistin, or sulbactam, combined with tigecycline could suppress the development of resistance. However, the in vitro environment is substantially different from the complex environment of the in vivo infection site; thus, the use of combination therapy as an alternative to treat A. baumannii should be verified by multicenter, randomized clinical trials.
Footnotes
Acknowledgments
This work was supported by funds from the National Natural Science Foundation of China (81403084), the Science and Technology Program of Guangzhou, China (201509010012), and Major Projects for Collaborative Innovation in Medical Health Care of Guangzhou (201508020253).
Disclosure Statement
No competing financial interests exist.