
Abstract
Fluoroquinolone (FQ) resistance in clinical isolates of Shigella species has been increasing reported in recent years. This study was carried out to find the mutations within the quinolone resistance-determining regions (QRDRs) and the prevalence of plasmid-mediated quinolone resistance (PMQR) determinants among the clinical isolates of Shigella sp. in Tehran, Iran. A total of 50 Shigella isolates were collected from five teaching therapeutic centers in Tehran, Iran and analyzed for antibiotic susceptibility over a period of 20 months from July 2015 to January 2017. The PCR and direct nucleotide sequencing were used for genetic alterations in the QRDRs. The PMQR genes were detected using PCR. The results revealed four types of mutations in the QRDR of gyrA: 20 (40%) had a S83L mutation, 1 (2%) had a S83A mutation, 2 (4%) had a D87G mutation, and 1 (2%) isolate had a D87Y mutation. Mutations were also found at codon N57D, D200N, and E210K in three isolates. Seven hospitalized children had qnrS determinants, and one isolates had the mutation S83A, while two isolates had double mutations at S83L and/or D87G (Ser83Leu and Asp-87Gly). The PMQR gene-positive isolates had the single replacement of serine with leucine. In hospitalized children, two isolates had two types of PMQR determinants (qnrS and qnrA) and (qnrS and qnrB) at once. The results of this study indicate that the emergence of strains with mutations in the QRDR regions and the capture of PMQR determinants in strains may lead to failure in therapy with FQ and the widespread emergence of strains with high-level FQ resistance.
Introduction
S
Increase in antimicrobial resistance to commonly used antibiotics including tetracycline (TET), sulfonamides, ampicillin (AMP), and trimethoprim/sulfamethoxazole among Shigella isolates has led to the conclusion that these agents are no longer recommended for empirical treatment. 3 For example, oral quinolone for proven or suspected Shigella infections is recommended by most authorities.1,3 Nalidoxic acid (NAL) and ciprofloxacin (CIP) are alternative medicines that have been highly effective, although many authorities are hesitant about their use in children.1,3 The quinolone-resistant Shigella isolates have emerged in various parts of the world, particularly in Africa and Asia.5,6 Fluoroquinolones (FQs) act by inhibiting both gyrase and topoisomerase IV, which eventually leads to cell death. 7 FQ resistance is commonly caused by mutations in the gyrA and parC genes and in the highly conserved quinolone resistance-determining regions (QRDRs); these mutations alter the DNA gyrase-binding sites of quinolone.3,7,8
FQ resistance is also mediated by a novel mechanism of plasmid-mediated quinolone resistance (PMQR), as defined by a series of tandem five amino acid repeats, which protects topoisomerase IV and DNA gyrase from the quinolone. There are five Qnr proteins: QnrA, QnrB, QnrC, QnrS, and QnrD. 9 Aminoglycoside N-acetyltransferase acts as a second PMQR mechanism to diminish CIP activity by adding an acetyl group to the CIP, which decreases its effect. 10 The QepA protein is considered to be a third PMQR mechanism because it causes FQs to be extruded from the cell. 11 PMQR gene-positive isolates are susceptible to quinolones and FQs, although studies have revealed that these isolates can lead to higher levels of FQ resistance. 12
Since PMQR determinants are transferable broad host range plasmids, they spread easily, between children in childcare facilities; they are also related to the expression of an extended-spectrum β-lactamase (ESBL) phenotype. 13 FQ treatment of Shigella infections from strains that carry quinolone resistance genes or have mutations in the QRDRs are more difficult to treat and may increase the risk of drug therapeutic failure.14,15 Therefore, continuous monitoring of FQ resistant Shigella isolates and genetic testing on select strains with the previously mentioned characteristics are essential. This study was carried out to find the mutations within the QRDRs and the prevalence of PMQR determinants among the clinical isolates of Shigella sp. in Tehran, Iran.
Materials and Methods
Bacterial strains
A total of 50 Shigella strains were isolated from 490 pediatric patients with diarrhea who were admitted to five teaching therapeutic centers in Tehran, Iran over a period of 20 months from July 2015 to January 2017. The samples were cultured on Shigella–Salmonella agar, xylose lysine deoxycholate, MacConkey agar, and Hektoen enteric agar (Difco Laboratories, Inc., Detroit). Individual isolates were surveyed using previously defined standard biochemical and serological tests. 16 All isolates were confirmed to be Shigella spp. using API 20E test strips (bioMérieux, France). Serogrouping of the Shigella isolates was performed using slide agglutination with specific antisera (Mast Group Ltd., Merseyside, United Kingdom). The confirmed Shigella isolates were kept in brain heart infusion broth with 40% glycerol at 70°C.
Antibiotic susceptibility testing
The FQs CIP and NAL were tested by Etest Method in accordance with the recommendations of the Clinical Laboratory Standards Institute. 17 The Kirby–Bauer disk diffusion method was used with the following antimicrobials: chloramphenicol 30 μg (CHL), ceftazidime 30 μg (CAZ) + clavulanic acid 10 μg (CLA), cefotaxime 30 μg (CTX) + CLA 10 μg, NAL 30 μg, CIP 5 μg, gentamicin 10 μg, TET 30 μg, AMP 20 μg, co-trimoxazole 5 μg (SXT), CTX 30 μg, CHL 10 μg, and CAZ 30 μg + ceftriaxone 30 μg (CRO) (Mast Group Ltd., Merseyside, United Kingdom). 17 The ESBL phenotype of the Shigella isolates was detected using the double-disk synergy test. Briefly, the test was performed using both CTX 30 μg and CAZ 30 μg alone and in combination with CLA. All ESBL-producing isolates were tested using the minimum inhibitory concentration (MIC) test for CTX, CRO, and CAZ with the Etest (AB Biodisk, Solna, Sweden). Escherichia coli ATCC 25922 and ATCC 35218, and were used as control strains.
PCR amplification
The genomic DNA of the Shigella isolates was extracted and applied to a template. PCR assays were carried out that argeted the QRDRs of the gyrA, gyrB, parC, and parE genes. 18 PCR was also used to investigate the PMQR determinants qnrS, qnrA, qnrB, aac(6′)-Ib-cr, and QepA, using the described primers listed in Table 1. The protocol followed for the PCR by the qnr gene was based on the method described by Wang et al. 19 All Shigella isolates were selected for these determinants. PCR amplifications were carried out using the methods described by Wang et al. 19 and Chen et al. 20 The primers and PCR amplifications of CTX-M15, integron class 1 (int1) and integron class 2 (intII) were carried out based on previously described studies.21–24
DNA sequence analysis
Prominent amino acid substitutions in the QRDRs of gyrA and parC from NAL-resistant Shigella isolates were compared with the sequence of a susceptible strain of S. sonnei [ARS 04283.1] for gyrA. The S. flexneri reference sequence WP_001281839.1 was used for the DNA topoisomerase IV subunit A [parC].
Analysis of data and sequence
The database software program SPSS (version 16.0; Armonk, New York) was used for the statistical analyses. Differences in FQ resistance rates and mutation frequencies were surveyed using the χ test, where p < 0.05 was considered statistically significant.
Results
Bacteria isolation and serotypes
Fifty children with culture-confirmed shigellosis were studied. S. sonnei was the frequently isolated serogroup 40 (80%), followed by S. flexneri 9 (18%) and S. dysenteriae 1 (2%); S. boydii was not isolated (p < 0.001). Table 2, shows the resistance groups based on their FQ resistance profiles. Data analysis revealed that 11 (22%) of the children who tested positive for one of the Shigella isolates were hospitalized; thus, 7 (17.5%) of the 40 with S. sonnei, 3 (33%) of the 9 with S. flexneri, and 1 (100%) with S. dysenteriae. The predominant Shigella isolates in both hospitalized and nonhospitalized children was S. sonnei.
PMQR, plasmid-mediated quinolone resistance; F, flexneri, S, sonnei; intI, integrin; QRDR, quinolone resistance-determining region; AMP, ampicillin; CTX, cefotaxime; CIP, ciprofloxacin; CAZ, ceftazidime; NA, nalidixic acid; CIP, ciprofloxacin; GM, gentamicin; CHL, chloramphenicol; SXT, co-trimoxazole; MIC, minimum inhibitory concentration; TET, tetracycline; N, none; P, positive.
FQ susceptibility
Of the Shigella isolates, 22 (55%) S. sonnei, 7 (77.8%) S. flexneri, and 1 (100%) of the S. dysenteriae were resistant to NAL. For the S. flexneri isolates, 6 (85.7%) serotype 2a and 1 (14.3%) serotype 1a were resistant to NAL. Statistical analysis showed that the incidence of resistance differed considerably between NAL and CIP (Table 2). The overall rate of resistance to CIP was 10%, and most of the CIP-positive isolates belonged to S. sonnei. Out of 30 Shigella isolates that were resistant to NAL, 5 isolates showed CIP resistance (10%) at MIC >32 μg/ml and 5 isolates showed CIP resistance at 1 ≤ MIC ≤0.25 μg/ml, while the rest of the isolates showed CIP resistance at <0.25 μg/ml. Of the five CIP-positive isolates, two were associated with hospitalization, while all five were resistant to NAL at MIC >8 μg/ml. isolates numbers (INs) 250 and 302 from the five CIP-positive strains were resistant to extended-spectrum cephalosporins and had the CTX-M-15 gene. All CIP-resistant isolates were also resistant to SXT, NAL, AMP, and TET, and harbored the class 2 integron.
Mutations in gyrA, gyrB, parC, and parE
Mutations in the gyrA gene were identified in 20 (40%) of the isolates. There were three common types of mutations detected in the QRDR of gyrA: 20 isolates (40%) had S83L, while 3 (6%), INs 274, 302, and 250, had D87Y and D87G mutations. Mutation at codon 83 of gyrA, which leads to a serine substitution of the leucine residue (transition C to T), was the most common substitution in all of the Shigella isolates. In the Shigella isolates without mutations and in the single isolate with a Ser83 to leucine substitution, the CIP MICs were ≤1 μg/ml. The MIC in isolates with a single gyrA mutation (S83L) was lower than the MIC in isolates with a double gyrA mutation (S83L and D87G) (Fig. 1). None of the Shigella strains had any mutations in the QRDR regions of the gyrB or parE genes. All hospitalized patients who were infected with either S. sonnei or S. flexneri had a single mutation in the region of S83L. Single mutations in parC (S80I) were seen with the simultaneous presence of a gyrA mutation. All CIP-resistant isolates (MIC >32 μg/ml) had a detectable mutation in the QRDR of gyrA at positions 83 or 87 (S83L and/or D87G) and a single mutation in parC at position 80 except for one isolate (Fig. 2). One common mutation in IN 303 [GCG (S83A)], and common mutations [D87G] in INs 302 and 250 were found (Table 2). In the amino acid region of 87 GAC (Asp), amino acid substitutions D87G, D87Y were detected in 302 and 250, 274, respectively. Mutations were also found at codon N57D, D 200N, and E210K in INs 271, 251, and 306. The mutations at codon 91 [His (Glu)], and [Leu (Arg)] appear outside the QRDR region of parC in IN 265, and one common mutation [Pro (Ser)] in three isolates were detected. The presence of a number of mutations should be noted in positions N57D, and D210 N in IN 306, D87Y in IN 274 in gyrA, and IN 303 S83A, in outside and inside region of the QRDR domain in the gyrA gene, which is reported for the first time in Iran.
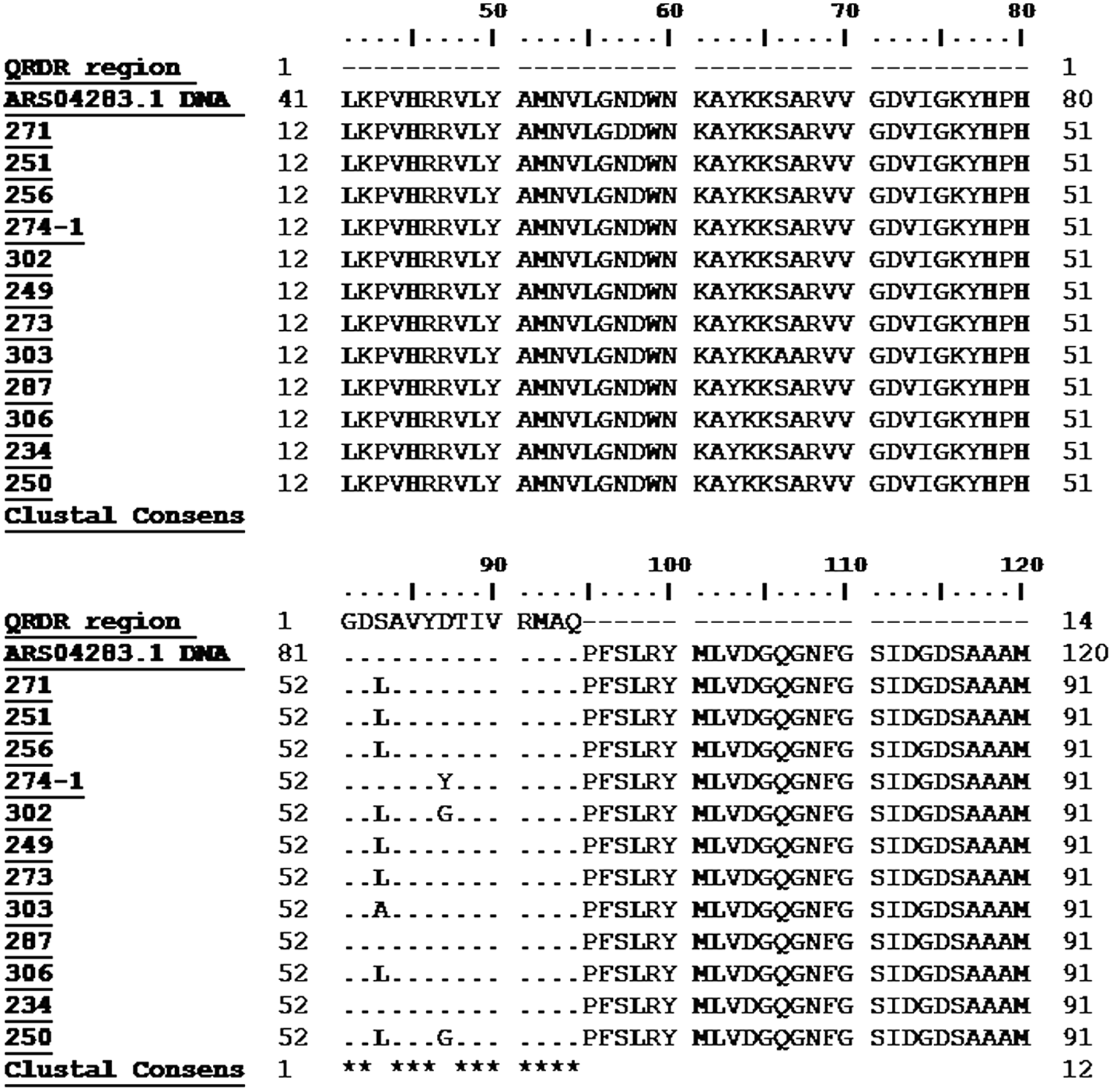
Nucleotide sequence of a gyrA region of the Shigella isolates, ARS04283.1: DNA gyrase subunit A [Shigella sonnei].
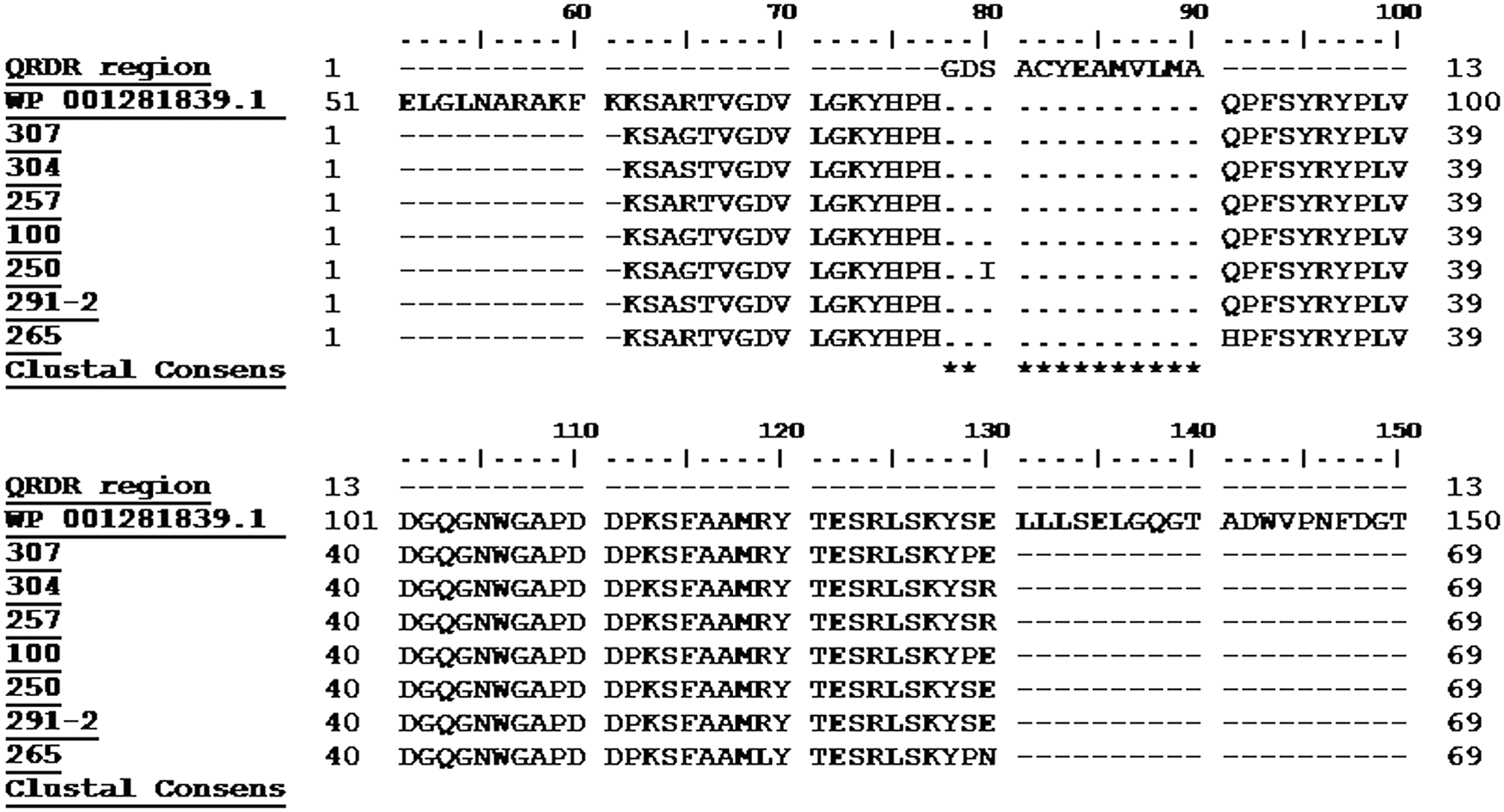
Nucleotide sequence of a parC region of the Shigella isolates, Reference Sequence Strain; WP_001281839.1 DNA topoisomerase IV subunit A [Shigella flexneri].
Characterization of qnr genes
Of the 50 Shigella isolates, 13 (26%) carried the PMQR determinants: 11 (22%) carried qnrS, 5 (10%) harbored only qnrB, and 3 (6%) carried qnrA determinants. All the 11 qnrS positive were resistant to NAL, and 5 were also resistant to CIP (Table 2). We found that the MDR isolates carried the qnrS, qnrA, qnrB, intII, intI, and blaCTX-M-15 genes. None of the isolates were positive for the aac(6′)-Ib-cr and QepA genes. All isolates, except for four, that were carrying the PMQR gene had a single replacement of serine with leucine. For the five CIP-positive strains, the isolates harboring the qnrS gene were resistant to NAL. In the hospitalized children, INs 306 and 303 had two types of PMQR determinants (qnrS and qnrB), but were sensitive to CIP (Table 2). Seven of the hospitalized children had qnrS determinants, and IN 303 had any mutation S83L. All four ESBL-producing isolates carried qnrS, although a single clinical isolate harbored qnrS and qnrA simultaneously. However, isolates numbers 250 and 302 had double mutations at S83L and/or D87G. It should be emphasized that clinical isolate harbored qnr genes, (qnrS and qnrA) and (qnrS and qnrB), simultaneously first reported in FQ-R Shigella strains in Iran.
Discussion
Diarrhea caused by Shigella species is a major public health problem in developing countries, especially for children <5 years old. 4 FQ is the primary choice of treatment for MDR Shigella infections. Previous studies demonstrated that a high rate of FQ resistance is mostly due to QRDR alterations and PMQR determinant mechanisms. 4 This is the first study in Iran to investigate the genetic characterization of novel mutations in the QRDR region and outside it and the presence of two types of PMQR determinants. Our results indicated the seriousness of the problem associated with NAL-resistant Shigella spp. Thirty isolates showed resistance to NAL and most of the isolates had a mutation at codon 83 [TCG (Ser)]. In contrast, a low percentage (<5%) of the Shigella isolates demonstrated resistance to NAL in other countries, including Turkey (4.7%) 4 and the United States. 25 This difference in rate of resistance may be due to the strict rules for antimicrobial therapy prescription in different countries. Bhattacharya et al. reported that resistance to NAL by almost all isolates existed in India by 2006–2009. 26 Our findings are in contrast with previous studies in India in which Shigella resistance to CIP gradually increased up to 48% over a 5-year period between 2002 and 2007. 16 In this study, high number of NAL-resistant strains displayed the most common mutation in gyrA (Ser83Leu), with another mutation that was only observed in the CIP-resistant isolates at codon 87 of the gyrA region. There is satisfactory agreement between our results and the research findings by Ruiz et al. 27 who reported that a mutation in codon 83 of the gyrA played an important role in the acquisition of high-level NAL resistance in clinical isolates of Shigella. In this study, some of the CIP-resistant isolates showed double mutations in the QRDR of a subunit of gyrA (Ser83Leu and Asp87Gly). In contrast to our results, another report noted that mutations in gyrA and parC were essential to achieve a high level of FQ resistance. 18
Results of this study showed that the CIP MICs for all isolates with just a single gyrA mutation resulting in the substitution of serine (TCG) by leucine (TTG) were ≤1 μg/ml. Our findings is in agreement with previous reports that decreased susceptibility to CIP (MIC: 0.125–2 μg/ml) in S. sonnei strains is related to an alteration of Ser83 in gyrA [16]. Our results in contradiction with previous research 5 on the prevalence of qnrS. However, qnrS was the most prevalent PMQR determinant, and had a higher prevalence than was shown in previous studies.
Pu et al. 28 reported that 5 of 15 (34%) FQ-resistant isolates harbored the qnrS determinant; their serotypes were S. flexneri 1a, 2a, and 4c, which is in contrast with our results. Das et al. reported that qnrB was the most prevalent gene (93.7%), followed by qnrC (18.7%). 29 Cui et al. 30 performed a study in which 22% (n = 58) of the isolates contained the aac(6′)-Ib-cr gene and two isolates contained the qnrS gene. 29 Cui et al. 30 performed a study in which 58 (22%) of isolates contained the aac(6′)-Ib-cr gene, and 3% isolates contained the qnrS gene. In Iran, Ranjbar et al. 3 found that, of the 23 quinolone-resistant isolates, 4 (17.4%) contained the qnrS gene. In the present study, all PMQR-positive Shigella isolates were positive for class 2 integrons. The five Shigella isolates that were CIP-resistant were also resistant to at least four other antibiotic agents, and were positive for qnrS and for class 2 integrons. This raises the possibility that these genes had a significant correlation among the Shigella isolates. Liu et al. 31 showed that 58.3% of the PMQR-positive isolates were also positive for the blaCTX-M gene, and that 50% of the aac(6′)-Ib-cr-positive isolates harbored class 1 or class 2 integrons, which agreed with our data. Four ESBL-producing S. sonnei isolates possessed the CTX-M-15 gene; two of the isolates were CIP-resistant and harbored the qnrS gene. Our results agree with several studies from different countries, such as India, 32 Germany, 33 Spain, 34 The Netherlands, 35 and Denmark, 36 all of which mentioned or elaborated on the relationship of the blaCTX-M-15 with qnr determinants and other ESBLs. 40 In a study by Xiong et al., 37 more than half of the PMQR determinants were associated with bla genes, especially blaCTX-M-14. Remarkably, in our research, we found that INs 303 and 302 harbored both the qnrS and qnrB genes and IN 392 harbored both the qnrA and qnrB determinants. Similar studies on Shigella isolates 28 and E. coli isolates 38 reported that the isolates carried the aac(6′)-Ib-cr and qnrA genes. 39
Conclusion
Treatment with FQ in patients contaminated with Shigella strains that carry quinolone resistance genes or that have chromosomal mutations that confer quinolone resistance may increase the risk of secondary diseases, long-course treatment (hospitalization), and drug therapeutic failure; it can also cause an increase in the quantity of organisms shed in the feces. To rectify this situation, in addition to limiting the administration of FQ in Iran to control the spread of resistance, it is essential to perform continuous monitoring and genetic testing to detect FQ-resistant Shigella strains. Therefore, FQ should not be the first-line treatment for these children patients since high failure rates are to be expected.
Footnotes
Acknowledgments
This work was supported by the Vice-Chancellor for Research grant (No. 30232) of Tehran University of Medical Sciences (TUMS) (Tehran, Iran). We thank the Children's Medical Centers–Bahman, Shariati, Valiasr, Imam Khomeini, and Mofid Hospitals–in Tehran for referring isolates and epidemiological and demographic data for use in this study.
Disclosure Statement
No competing financial interests exist.