
Abstract
Antibiotic therapy for children infected with Helicobacter pylori is important. However, resistance to antibiotics is one of the main causes of treatment failure. This study was designed to evaluate the prevalence pattern of antibiotic resistance of H. pylori in Iranian children using a systematic review and meta-analysis of literature. A computerized search (until June 10, 2017) using related keywords in the national and international databases was performed. A total of 261 original articles on antibiotic resistance of H. pylori in Iranian children were collected. After screening for inclusion and exclusion criteria, six eligible articles were included in the meta-analysis. Resistance rates of H. pylori to different antibiotics were as follows: metronidazole: 71%, clarithromycin: 12.2%, amoxicillin: 20.4%, tetracycline: 8.4%, ampicillin: 21.4%, rifampin: 28.6%, furazolidone: 8.4%, ciprofloxacin: 16.2%, azithromycin: 19%, erythromycin: 15.3%, and nitrofurantoin: 0%. The prevalence of H. pylori resistance to metronidazole, amoxicillin, ampicillin, and rifampin among Iranian children was high. Therefore, a careful monitoring of antibiotic resistance to select the best treatment options and prevent treatment failure is required. Although resistance to some antibiotics such as clarithromycin, tetracycline, furazolidone, and ciprofloxacin was less prevalent, frequent consumption of these drugs in children should be controlled owing to their known adverse events.
Introduction
H
Based on age, race, ethnicity, and geographical region, the prevalence of H. pylori infection in Iran is very high, affecting about 90% of the adult population and more than 50% of children.8,9 Reports from Iran have shown that several factors are related to the prevalence of H. pylori infection in children, including low socioeconomic and sanitary status, and poor educational status.10,11
According to the recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition, the Canadian Helicobacter Study Group, and the Japanese Pediatric Helicobacter Study Group, a triple therapy using a proton pump inhibitor (PPI) and two antibiotics such as amoxicillin, clarithromycin, and metronidazole is the best regimen to eliminate H. pylori infection in children.12,13 Suggested treatment regimens for H. pylori eradication in Iranian children are triple, as the first-line therapy, and quadruple, as the second-line therapy. 12 However, due to the widespread use of antibiotics for the treatment of other infections, resistance to antibiotics is an important concern in the pediatric age group.12,13 In Iran, elimination rate of infection is low. 11 Therefore, periodic monitoring of the antibiotic susceptibility of H. pylori is essential to avoid treatment failure.
Hitherto, there has been limited information about antimicrobial susceptibility of pathogenic bacteria in Iranian children. The aim of this systematic review and meta-analysis was to determine the prevalence pattern of antibiotic resistance of H. pylori to antimicrobial agents used in the treatment of infections in Iranian children.
Materials and Methods
Search strategy
Based on the PRISMA (preferred reporting items for systematic review and meta-analyses) checklist, a comprehensive literature review was performed to find studies reporting the prevalence of antibiotic resistance of H. pylori in Iranian children. Until June 10, 2017, a full computerized search in PubMed, Scopus, Google Scholar, and ISI web of knowledge databases was conducted using relevant keywords to find published English-language articles. Selected MeSH terms were as follows: “antibiotic resistance” OR “drug resistance” AND “Helicobacter pylori” OR “H. pylori” AND “children” OR “pediatric” AND “Iran”. The same strategy was used in Persian databases, including the Scientific Information Database (www.sid.ir), Irandoc (www.irandoc.ac.ir), Iranmedex (iranmedex.ir), and Magiran (www.magiran.com). To avoid losing any additional data, we performed a complementary literature search of reference lists. Computerized searching was performed with the same terms by two authors to collect a complete list of articles and avoid any bias.
Evaluation criteria
After title, abstract, and full text review, eligibility of the studies was determined based on inclusion and exclusion criteria. Three main inclusion criteria were as follows: (1) Persian- and English-language original articles, (2) articles presented as cross-sectional or cohort studies, and (3) articles that assessed primary antibiotic susceptibility patterns of H. pylori in Iranian children. Nonrelevant articles with the following characteristics were excluded: (1) assessment of antibiotic resistance of H. pylori in Iranian adults, (2) evaluation of the prevalence of H. pylori infection along with eradication therapies in Iranian children, (3) assessment of antibiotic resistance in other countries, (4) duplicate studies, (5) review articles, and (6) abstract of articles.
Data extraction
All required data are extracted and tabulated in Table 1. These include the following: (1) first author, (2) year, (3) area (city), (4) number of patients, (5) methods used for evaluation of antibiotic resistance, (6) sex, (7) age, (8) number of H. pylori strains, and (9) drug resistance of bacteria to various antibiotics.
AMO, amoxicillin; AMP, ampicillin; AZT, azithromycin; CIP, ciprofloxacin; CLA, clarithromycin; ERY, erythromycin; FRZ, furazolidone; MTZ, metronidazole; NA, not available.; NIT, nitrofurantoin; RIF, rifampin; TET, tetracycline.
Statistical analysis
All eligible information were pooled and analyzed based on random-effects model due to the potential heterogeneity. Cochrane Q-test (p < 0.05 was considered statistically significant) and I-squared (I2) index were used for evaluating heterogeneity of results. The possibility of publication bias was checked by funnel plots. Antibiotic resistance rate of H. pylori in Iranian children was expressed as percentage and 95% confidence intervals (95% CIs). In this meta-analysis, all statistical analyses were performed using Comprehensive Meta-Analysis (CMA) software version 2.2 (Biostat, Englewood, NJ).
Results
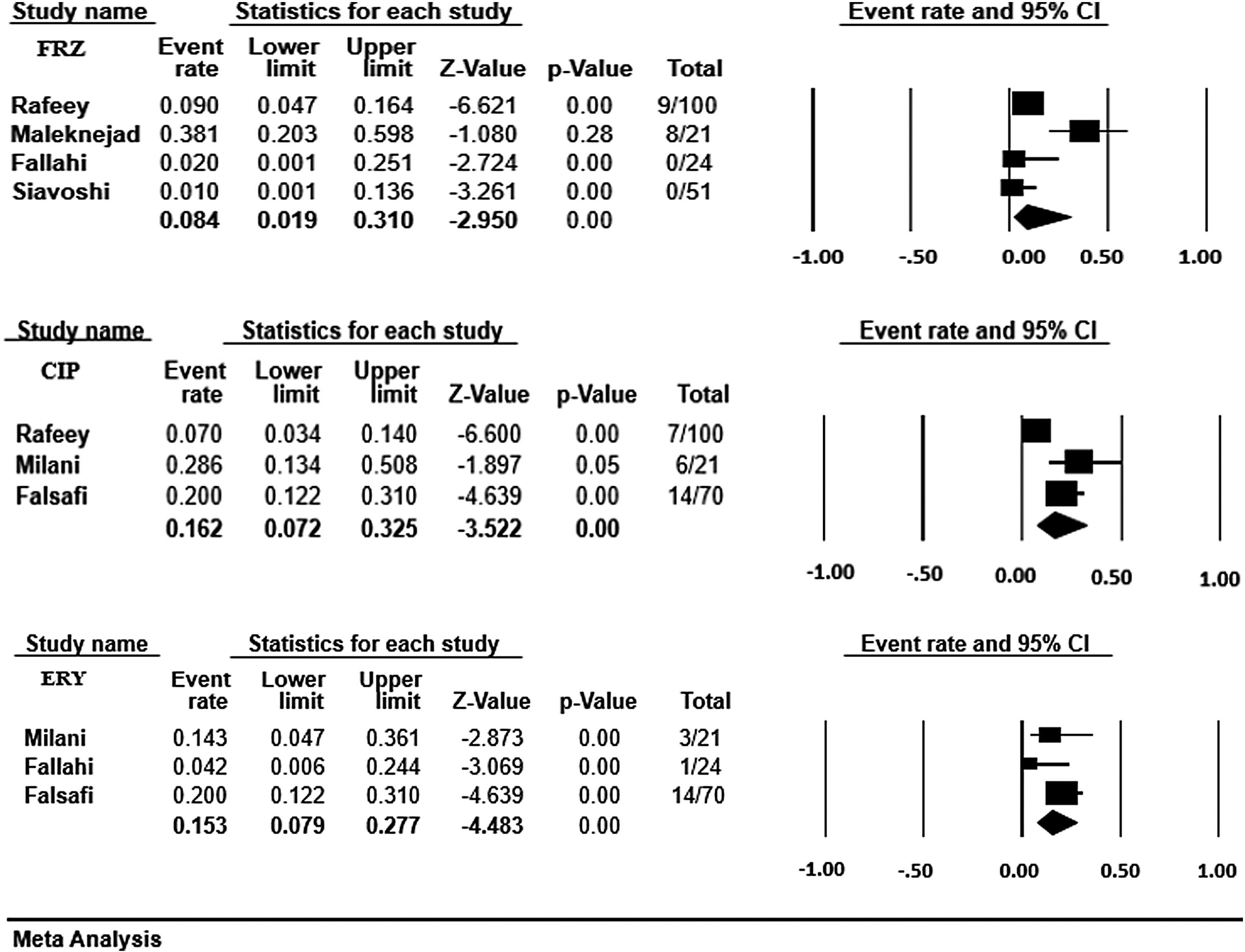
A total of 6 potentially relevant articles were selected from 261 original articles after a search in Iranian and international databanks on antibiotic resistance of H. pylori in Iranian children and based on process of study selection in Fig. 1. Table 1 shows profiles of included studies as summarized. The age range of patients was between 1.5 and 15 years. Among six included articles, the disk diffusion method was the most commonly used method to determine the susceptibility of H. pylori isolates from children in Iran to different antimicrobials, including metronidazole, clarithromycin, amoxicillin, tetracycline, ampicillin, rifampin, furazolidone, ciprofloxacin, azithromycin, erythromycin, and nitrofurantoin. Figure 2 presents the forest plot of the meta-analysis on antibiotic resistance of H. pylori in Iranian children. As shown in Fig. 2, resistance rates of H. pylori-infected children to different antibiotics are as follows: metronidazole: 71% (95% CI: 48.2–86.6), clarithromycin: 12.2% (95% CI: 7.3–19.6), amoxicillin: 20.4% (95% CI: 8.6–41.3), tetracycline: 8.4% (95% CI: 3.5–19), ampicillin: 21.4% (95% CI: 13.4–32.6), rifampin: 28.6% (95% CI: 13.4–50.8), furazolidone: 8.4% (95% CI: 1.9–31), ciprofloxacin: 16.2% (95% CI: 7.2–32.5), azithromycin: 19% (95% CI: 7.3–41.2), erythromycin: 15.3% (95% CI: 7.9–27.7), and nitrofurantoin: 0%. Heterogeneity of studies using the I2 index and Cochrane Q-test showed evidence of heterogeneity between studies (I2 = 89.6, p < 0.001). Therefore, we pooled data using random-effects model. As shown in Fig. 3, the funnel plot was used to identify the presence of publication bias. The asymmetry of the distribution of studies in the plot could be due to publication bias.
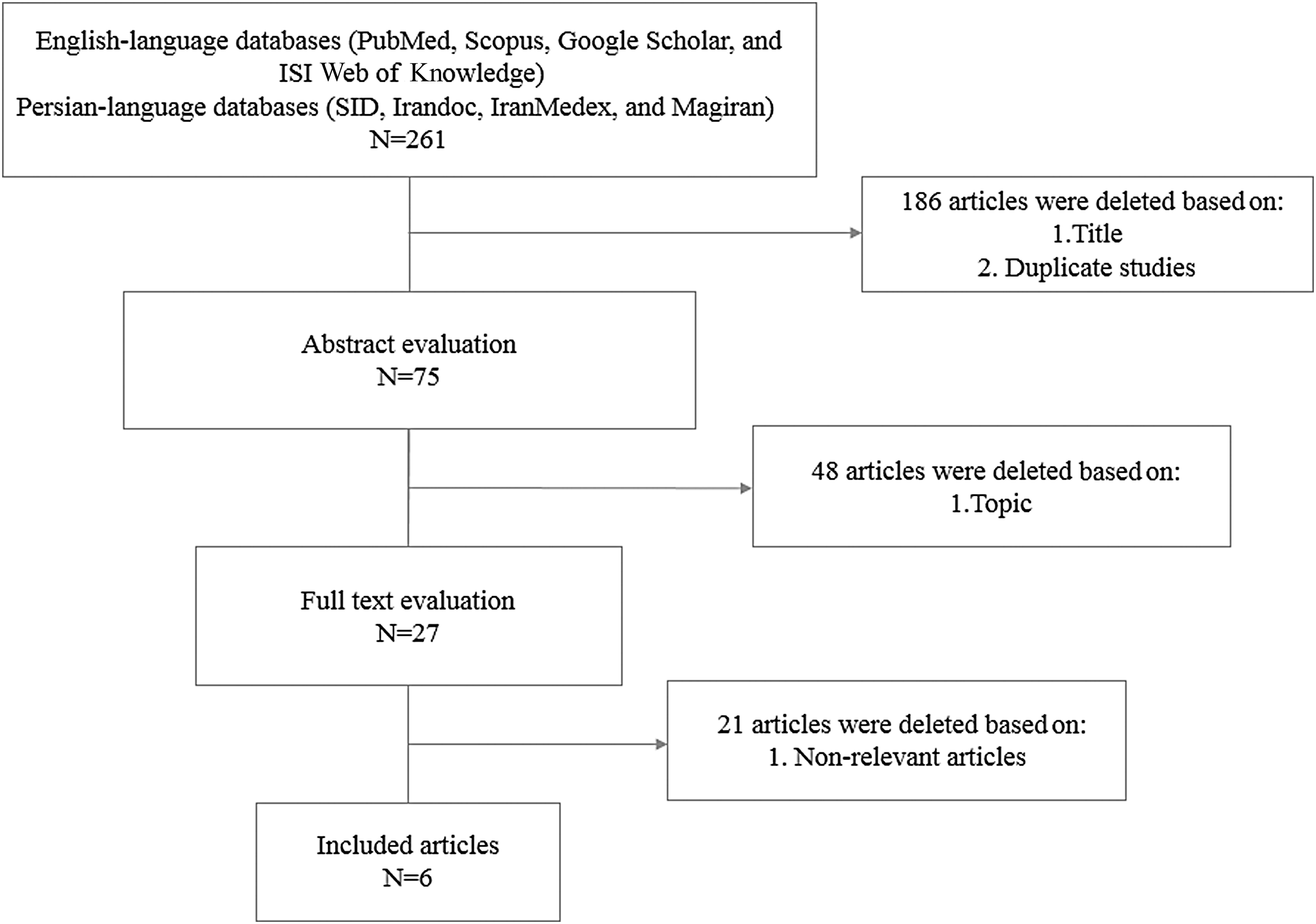
Literature review flowchart.

Forest plot of antibiotic resistance of Helicobacter pylori in Iranian children. CI, confidence interval; CIP, ciprofloxacin; ERY, erythromycin; FRZ, furazolidone.
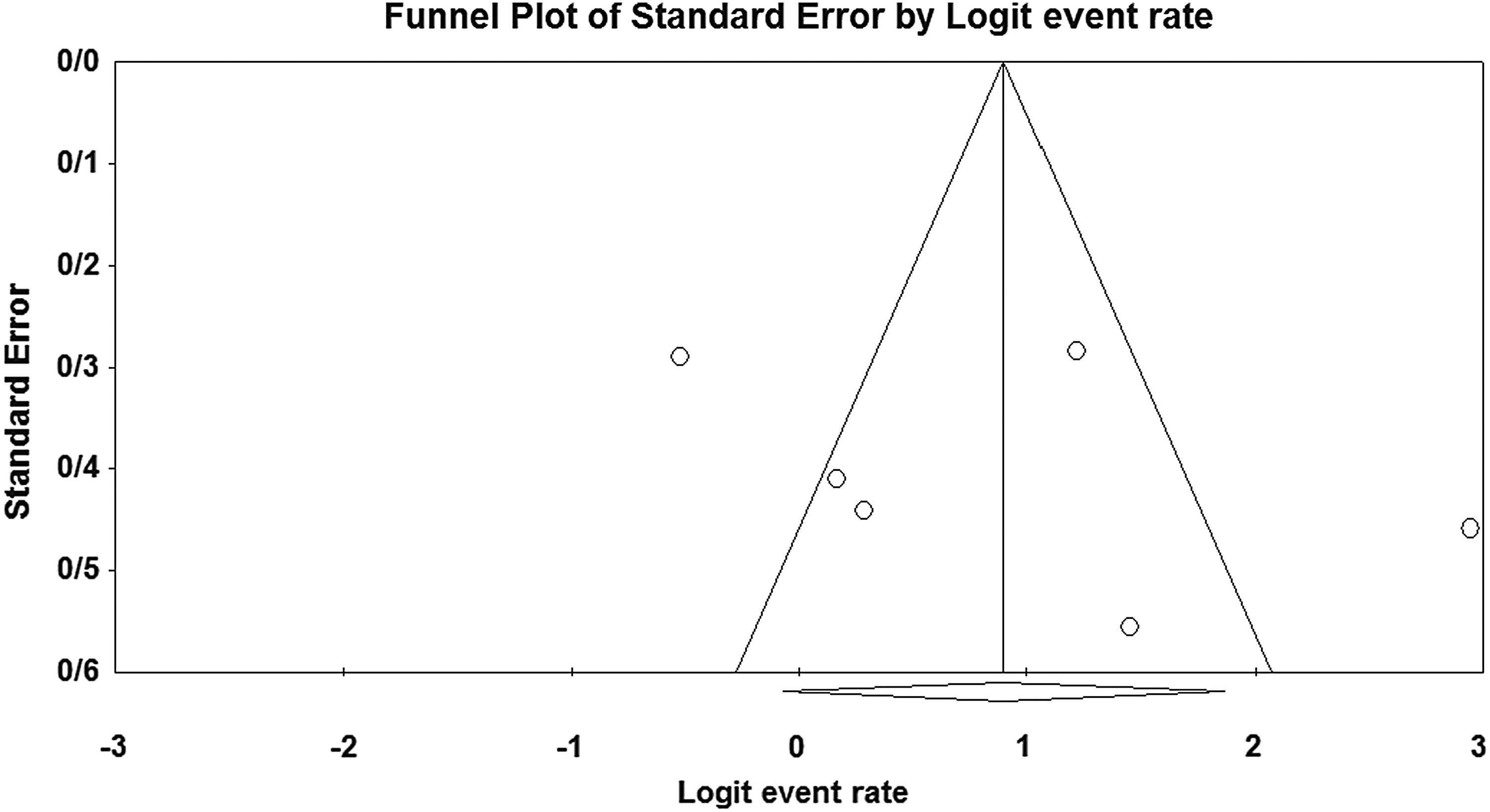
Funnel plot of the meta-analysis on resistance of H. pylori to metronidazole in Iranian children.
Discussion
The prevalence of H. pylori infection among children and adults is different in different regions of Iran. A recent meta-analysis by Moosazadeh et al. in 2016 estimated the prevalence of H. pylori infection among Iranian children and adults as 42% and 62%, respectively. 18 In Iran, like other developing countries, the acquisition of infection happens in the first years of life. Therefore, an effective eradication therapy in H. pylori-infected children can dramatically prevent the burden of infection and associated complications in adulthood. However, resistance to antibiotics is always a major cause of treatment failure. 19
Metronidazole is a prodrug, which is activated by bacterial enzymes, resulting in the inhibition of DNA synthesis and cell death.1,20 Owing to its efficacy against protozoal and bacterial infections, cost-effectiveness, and acceptable safety, metronidazole has been recommended for the treatment of infections since 1962. 20 However, extensive use of this antibiotic in developing countries may be one of the major reasons for the emergence of metronidazole-resistant H. pylori strains. 1 According to this meta-analysis, the overall resistance rate of H. pylori-infected children to metronidazole in Iran was 71%. The resistance rate of H. pylori in Iranian children is higher than those reported in children from Italy (33%), Turkey (48.4%), Japan (14.8%), Bulgaria (16.2%), Portugal (16.5%), Croatia (10.1%), Spain (35.7%), Egypt (100%), French (36.7%), Poland (40%), Israel (31%), South Korea (27.3%), Polish (37%), Australia (43.5%), Belgium (17.4%), Austria (16%), Brazil (40.2%), and China (61.6%).21–38 Our study revealed that the prevalence of metronidazole resistance is increasing in Iranian children; therefore, it may reduce the efficacy of therapy in adulthood. Macrolide antibiotics, including azithromycin, clarithromycin, and erythromycin act by inhibiting protein synthesis and blocking the 50S ribosomal subunit. 3 Among macrolides, clarithromycin is frequently recommended for eradication of infections caused by H. pylori. In Iranian children, clarithromycin resistance rate of H. pylori was found to be 12.2%. This resistance rate is lower than those reported from Italy (26%), Turkey (30.1%), Japan (36.1%), Bulgaria (19%), Portugal (39.4%), Spain (54.6%), France (22.8%), Poland (28%), Israel (31%), South Korea (18.2%), Polish (19.3%), Austria (20%), Brazil (19.5%), China (84.9%), and Thailand (29.2%),21–25,27,29–33,36–39 but higher than those reported from Croatia (11.9%), Egypt (4%), Australia (8.7%), and Belgium (7.3%).26,28,34,35 Compared with clarithromycin and erythromycin resistance (15.3%), higher resistance to azithromycin (19%) was found. High resistance rate to azithromycin may be attributed to two well-known reasons: (1) cross-reactivity between macrolides; one macrolide-resistant strain becomes resistant to all others, and (2) azithromycin induces higher resistance in comparison with other macrolides. 35 In Iran, resistance rate of H. pylori strains to macrolide antibiotics is comparable to those reported from other developing countries, but it is lower than that reported from developed countries.28,32,39 It has been suggested that one reason for the high resistance rate of H. pylori to macrolides, especially in developed countries, is previous administration in the treatment of many infections, including skin and soft tissue infection, respiratory tract infection, acute otitis media, and community-acquired pneumonia. 31 Amoxicillin and ampicillin are two β-lactam antibiotics that act by interfering with the peptidoglycan synthesis. 40 According to the American College of Gastroenterology guideline, amoxicillin along with omeprazole and clarithromycin or metronidazole is first-line regimen for H. pylori eradication (clarithromycin-based triple therapy). 41 Due to the high resistance rate of other drugs, amoxicillin acts as an important anti-H. pylori antibiotic in children. 38 However, in Iranian children, amoxicillin resistance rate was also high (20.4%). It was higher than several Asian (0%)23,38 and European countries (0–0.9%),21,22,24,27,29,30,33,35,36 Australia (0%), 34 China (0%), 38 United States (4.4%), 42 and Brazil (10.4%). 37 A possible reason for the high amoxicillin resistance level in Iran is excessive use of the antibiotic in the treatment of many other infections, especially in children. As a result, such high amoxicillin resistance can be seen in other bacterial infections, including Salmonella spp., Shigella spp., and Campylobacter spp. infections. 14 We found only one report about resistance of H. pylori to ampicillin (21.4%) in Iranian children.
Tetracycline, a bacteriostatic drug, prevents protein synthesis through blocking the 30S ribosomal subunit. It was included in bismuth quadruple therapy regimen for eradication of H. pylori in the United States. 41 In H. pylori strains isolated from Iranian children, resistance rate to tetracycline remained negligible. In our study, one of the lowest H. pylori resistance rates belonged to tetracycline (8.4%), which is high compared with previous reports from European countries (0–2.7%), United States (0%), China (0%), Australia (0%), and Brazil (0%).34,37,38,42
H. pylori strains from Iranian children exhibited low resistance to furazolidone (8.4%) and tetracycline (8.4%). This low resistance rate is probably because they are not generally recommended for children due to some adverse events such as genotoxic and carcinogenic effects for furazolidone and tooth calcification for tetracycline. 37 However, in developing countries such as Iran, where there is a high resistance to metronidazole, furazolidone may be replaced for treatment of H. pylori infection. 37 Similar results in agreement with our study have been reported in Brazil (0%) and South Korea (6.1%).32,37 There has been no study on furazolidone resistance of H. pylori in children from United States and European countries owing to the restricted use for children. 37 For ciprofloxacin, the resistance rate was relatively high (16.2%). Ciprofloxacin is a fluoroquinolone antibiotic, which inhibits DNA synthesis by blocking the DNA gyrase and topoisomerase IV enzymes. 43 Ciprofloxacin is not commonly used for H. pylori eradication and used only in second-line regimens; moreover, this drug is contraindicated for children. Therefore, there is limited evidence on the resistance of H. pylori to ciprofloxacin.38,40,43 Ciprofloxacin resistance in children is low in comparison with adults. 35 However, in this survey, resistance rate was higher than those reported from Bulgaria (6.8%), Portugal (4.5%), Spain (1.8%), Egypt (2%), South Korea (15.2%), and Belgium (0.4%).24,25,27,28,32,35 High resistance to this antibiotic in Iran may be due to intrafamilial spread of quinolone-resistant strains from adults.25,38
There has been only one study on H. pylori resistance to rifampin and nitrofurantoin in Iranian children. According to our findings, H. pylori resistance to rifampin, an anti-Mycobacterium tuberculosis drug, in Iranian children is 28.6%. The resistance rates in children from Spain, Austria, and China were 0%, 0.9%, and 6.8%, respectively.27,36,38 Because nitrofurantoin is not used for the treatment of H. pylori, resistance rate was rare in Iran (0%). A similar finding consistent with our study has been reported in Bulgaria (0%). 24
Conclusion
Prevention of treatment failure and optimization of therapeutic drug regimens in children necessitates regular monitoring of drug resistance. The present systematic review and meta-analysis revealed high rates of H. pylori resistance to metronidazole, amoxicillin, ampicillin, and rifampin in Iranian children compared with other countries. This calls for an urgent attention to the pattern of antibiotic administration for pediatric infections in Iran. Although the prevalence of H. pylori resistance to clarithromycin, tetracycline, furazolidone, and ciprofloxacin in Iranian children was found to be low, the use of the three latter drugs is contraindicated in the pediatric group. According to the results of this study and the high resistance rate of H. pylori to main antibiotics used to treat infection, especially metronidazole, we recommend the use of clarithromycin-based triple therapy, containing clarithromycin, amoxicillin, and PPI, as first-line eradication treatment for Iranian children. In case of failure in treatment, other antibiotics with a low resistance rate, such as furazolidone and tetracycline, may be replaced.
Footnotes
Disclosure Statement
No competing financial interests exist.