
Abstract
Escherichia coli is one of the major causes of urinary tract infections in primary healthcare, and treatment is more complicated due to the increase in antibiotic resistance. Extended-spectrum β-lactamases are the most common mechanism of resistance against third-generation cephalosporin, and CTX-M-like are among the most prevalent. The aim of our work is to investigate the prevalence of blaCTX-M in isolates of E. coli obtained from samples of patients without previous known contact with the hospital. Ninety-four E. coli isolates with resistance to third-generation cephalosporin were collected between 2008 and 2013 in Guayaquil, Ecuador. Polymerase chain reaction, followed by sequencing, was performed to identify the type of blaCTX-M-Like. Enterobacterial repetitive intergenic consensus (ERIC)-PCR was carried out to determine the clonal relationship between isolates. These results show an increase in resistance to third-generation cephalosporin from 10.58% to 23.96%. CTX-M-15 was the most prevalent mechanism of resistance being that the isolates were not clonal. Overall, these results show an increase in antibiotic resistance in the community over time, suggesting that more precise antibiotic stewardship needs to be implemented to control the dissemination of antibiotic-resistant bacteria in this region.
Introduction
U
Urinary tract infection (UTI) is the most common bacterial infection, causing 150 million cases annually. 6 At least 40% of the female population and 12% of the male population will develop one episode of UTI during adulthood.7,8 Each episode causes an average of 6.1 days of morbidity and 0.4 days of rest, resulting in a great economic burden of $1.6 trillion per year for uncomplicated UTIs7,8. 9
Escherichia coli causes between 70% and 95% of community-based UTIs, 4 and the increased rates of resistance to drugs are forcing medical doctors to prescribe extended-spectrum antibiotics, such as third-generation cephalosporin (3GC), which was previously reserved for treatment of severe UTIs.7,10 Since the appearance of extended-spectrum β-lactamases (ESBLs), resistance to 3GC has increased to alarming percentages in some countries.11,12 ESBLs have been linked to mobile genetic elements, horizontal genetic transfer, and horizontal dissemination of epidemic clones such as E. coli ST 131, which carries CTX-M-15.12,13
Ecuador is not exempt from this global problem 14 ; however, there is little scientific literature regarding the prevalence of antibiotic resistance in community patients, as well as the type of ESBL, that is more predominant.1,15,16 We have found that CTX-M-15 is the most prevalent mechanism of resistance in Guayaquil. The diversity of strains carrying this genetic mode of resistance suggests its dissemination is not primarily due to clonal spread but rather due to horizontal gene transfer.
Materials and Methods
Selection of clinical isolates and patients
We included all E. coli strains with ESBL-positive phenotype and/or resistance to 3GC isolated from 2008 to 2013 at the Sosegar Clinical Laboratory in Guayaquil (Ecuador). The isolates were obtained from urine samples collected by midstream, catheters or suprapubic aspiration with bacterial colony count ≥105 CFU/ml and urinary sediment of ≥5 leukocytes per field.
Microbiological cultures
Five microliters of urine was inoculated on Cystine-Lactose-Electrolyte-Deficient (CLED) agar (Merck™) and MacConkey agar (BBL™) followed by incubation at 35°C for 16–18 hr in aerobic atmosphere. Bacterial identification was performed by conventional biochemical tests (oxidase test, Kligler iron test, lysine decarboxylation, urease, motility, indole production, and ornithine decarboxylation). 17
Antimicrobial susceptibility testing and ESBL detection
The Kirby–Bauer disk diffusion method was performed following the Clinical Laboratory Standards Institute (CLSI) (protocol document M02-A13). 18 Antibiotics tested were amoxicillin/Ac. clavulanic 20 μg (Amox/Clav), cefotaxime 30 μg (CTX), ceftazidime 30 μg (CAZ), imipenem 10 μg (IMP), meropenem 10 μg (MEM), gentamicin 10 μg (GN), amikacin 10 μg ciprofloxacin 5 μg (CIP), nitrofurantoin 300 μg (F), fosfomycin μg (P), and trimethoprim/sulfamethoxazole 1.25 μg/23.75 μg (SXT) (Bionalyse).
ESBL was determined by using cefotaxime and ceftazidime disks (Bionalyse) located at a distance of 20–25 mm from center to center of the amoxicillin/clavulanic acid disk according to the protocol of the WHONET antimicrobial resistance network of Argentina. 19 Inhibition zones were interpreted according to CLSI M100-S16. 20 Intermediate category was considered as resistant for statistical analysis. E. coli ATCC 25922, E. coli ATCC 35218, and Pseudomonas aeruginosa ATCC27853 were used as quality strains.
Amplification of blaCTX-M and blaCTX-M-1 genes
DNA extraction was performed following the manufacturer's recommendations with the QIAamp DNA Mini Kit (Qiagen™). 21 Quality of DNA was assessed by analyzing the ratio of absorbance at 260/280 nm.
Amplification of the blaCTX-M gene was performed using primers previously described. 21 Master Mix was prepared as detailed below: Mg 2 + 1× free polymerase chain reaction (PCR) buffer, 1.5 mM magnesium chloride, 2.5 U Taq polymerase, 0.4 mM deoxynucleotide mixture, and 1 mM of each primer in a final volume of 25 μl. Amplifications were performed in a BioRad thermocycler starting with an initial denaturation at 95°C (30 sec), followed by 36 cycles of denaturation (30 sec at 95°C), hybridization (30 sec at 58°C), and extension (60 sec at 72°C), and finally an extension step of 72°C for 10 min. The PCR product was visualized on 1% agarose gel stained with Diamond™ Nucleic Acid Dye (Promega) and photographed with Gel Doc XR System (BioRad).
Confirmatory PCR was performed on all CTX-M-positive strains. Primers used for determination of CTX-M-1 were those described previously by Cartelle et al. 22 PCR was performed in a final volume of 50 μl with the following concentrations: Mg 2 + 1× free PCR buffer, 1.5 U Taq polymerase, 1.5 mM magnesium chloride, 0.25 mM deoxynucleotide mixture, 5 μM CTX-1-F and CTX −1-R, and 3 μl DNA. Amplification reactions were performed in the BioRad thermal cycler under the following conditions: initial denaturation at 95°C (30 sec) followed by 30 cycles of denaturation (94°C for 30 sec), hybridization (60°C for 30 sec), and extension (72°C for 60 sec) and a final extension step at 72°C (10 min). The amplicons were visualized by 1.5% agarose gel electrophoresis stained with Diamond Nucleic Acid Dye (Promega) and photographed with Gel Doc XR System (BioRad). A local strain of E. coli bla CTX-M-1 assigned by J. Zurita was used as a positive control (Zurita & Zurita Laboratories, Quito, Ecuador).
blaCTX-M-1 gene sequencing
Amplicons of CTX-M-1 were sequenced by Macrogen, Inc. Korea (www.macrogen.com/esp/service_sequ02.html). Purification of the PCR was performed following the manufacturer's instructions (BigDye® X-Terminator™ Purification Kit Protocol; Applied Biosystems). The sequences obtained were analyzed with the MEGA 6 program and compared with the sequences described in the “Basic Local Alignment Search Tool (BLAST)” database (https://blast.ncbi.nlm.nih.gov/Blast.cgi? PAGE_TYPE = BlastSearch). We included one isolate of each clonal type.
Enterobacterial repetitive intergenic consensus-PCR
Clonality assays were performed in all CTX-M-1-positive strains using previously described primers. 23 PCRs were performed in a final volume of 50 μl using the following final concentrations: Mg 2 + 1× free PCR buffer, 2.5 U Taq polymerase, 3 mM magnesium chloride, 400 μM deoxynucleotide mixture, ERIC1 and ERIC2 1 μM primers, and 200 ng DNA. Amplifications were performed in the BioRad thermocycler as detailed here: denaturation at 95°C for 10 min, followed by 30 cycles of denaturation (94°C for 1 min), hybridization (55°C for 1 min), and extension (72°C per 2 min) followed by a final extension step at 72°C for 16 min. The amplicons were visualized on a 1.5% agarose gel stained with Diamond Nucleic Acid Dye (Promega) and photographed with Gel Doc XR System (BioRad). Two clinical isolates of Serratia marcescens previously characterized by enterobacterial repetitive intergenic consensus (ERIC)-PCR were included as control strains for each electrophoretic gel. Data were analyzed utilizing BioNumerics software version 6.1 (Applied Biosystems), using the Dice coefficient to analyze similarities. Dendrogram was generated by unweighted pair-group method with average linkages algorithm (UPGMA—optimization parameter of 1.5% and 1.5% tolerance).
Statistical analysis
Statistical analysis was performed with EPI-INFO 7 (Centers for Disease Control and Prevention). Statistical significance was calculated with Pearson's chi square test to determine relationships between CTX-M-1 and resistance to the other groups of antibiotics (ciprofloxacin, amikacin, nitrofurantoin, fosfomycin, and trimethoprim/sulfamethoxazole), as well as age and sex of the patients. Values of p ≤ 0.05 were considered statistically significant.
Results
Selection of clinical isolates and patients
During the study period a total of 8,768 urine cultures were processed, and E. coli was identified in 76.80% (884) of the isolates. One hundred twenty-one (13.68%) E. coli strains that were resistant to 3GC were included in this research. The number of resistant E. coli isolates increased over the years, although the number of urine cultures processed decreased during the 6 years (2008: 1701 urine cultures; 2009: 1723; 2010:1528; 2011:1428; 2012:1158; 2013:1176) (Fig. 1).
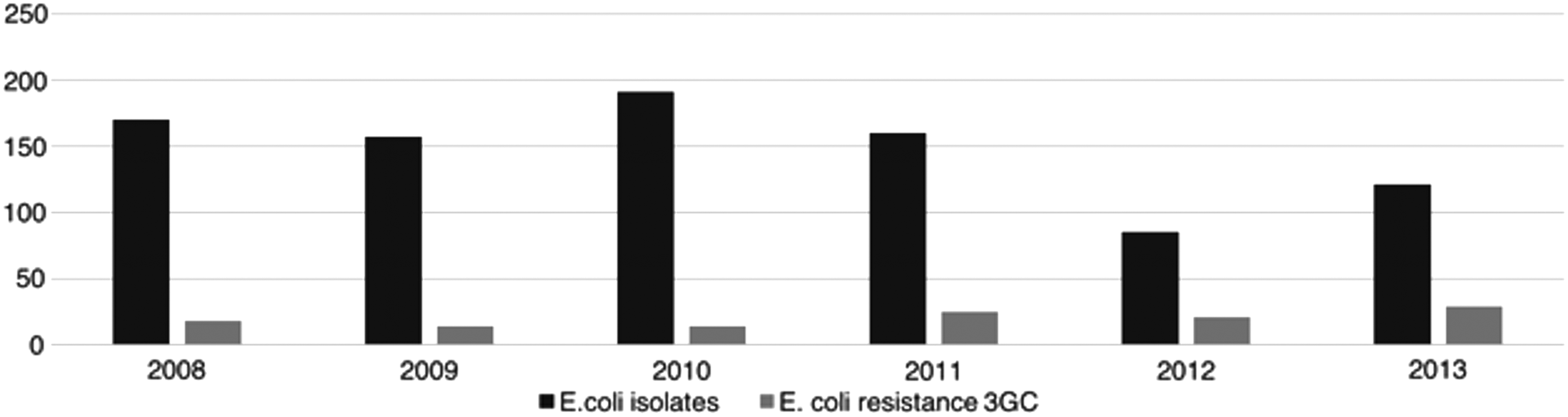
Distribution of Escherichia coli isolates, from 2008 to 2013, showing the increase of resistance to 3GC during the study years. 3GC, third-generation cephalosporin.
65.95% of the isolates corresponded with female patients, and the age was from 20 days to 88 years (mean 47.12 years old, standard deviation 26.67, median 51.5 years, and mode 10 years).
Antimicrobial susceptibility and confirmation of ESBL
Ninety-four strains of E. coli were included for confirmation and subsequent molecular study (27 strains were not stored and could not be further included in our study). Eighty-nine isolates (94.68%) presented ESBL-positive phenotype, and five were negative for ESBLs but were resistant to 3GC, which led us to also include them. Table 1 shows detailed information for each isolate, including laboratory code, isolate date, sex and age of patient, ESBL phenotype, and disk diffusion results (mm).
22 days old.
2 months.
6 months.
7 months old.
M, masculine; F, feminine; ND, no data; CTX, cefotaxime; CAZ, ceftazidime; FEP, cefepime; FOX, cefoxitin; ERT, ertapenem; AK, amikacin; GN, gentamicin; CIP, ciprofloxacin; TMS, trimethoprim/sulfamethoxazole; F, fosfomycin; ESBL, extended-spectrum β-lactamase.
Detection of the blaCTX-M gene and blaCTX-M-1
Seventy-four isolates (78.72%) resulted positive for CTX-M-like, 64 of which were positive for CTX-M-1 (Fig. 2). The results suggest that 10 of the strains could be included in another group of CTX-M, and that would explain the lack of amplification with the primers for the CTX-M-group 1. This indicates that there are other group/-s also present in the country, and more studies need to explore this further.
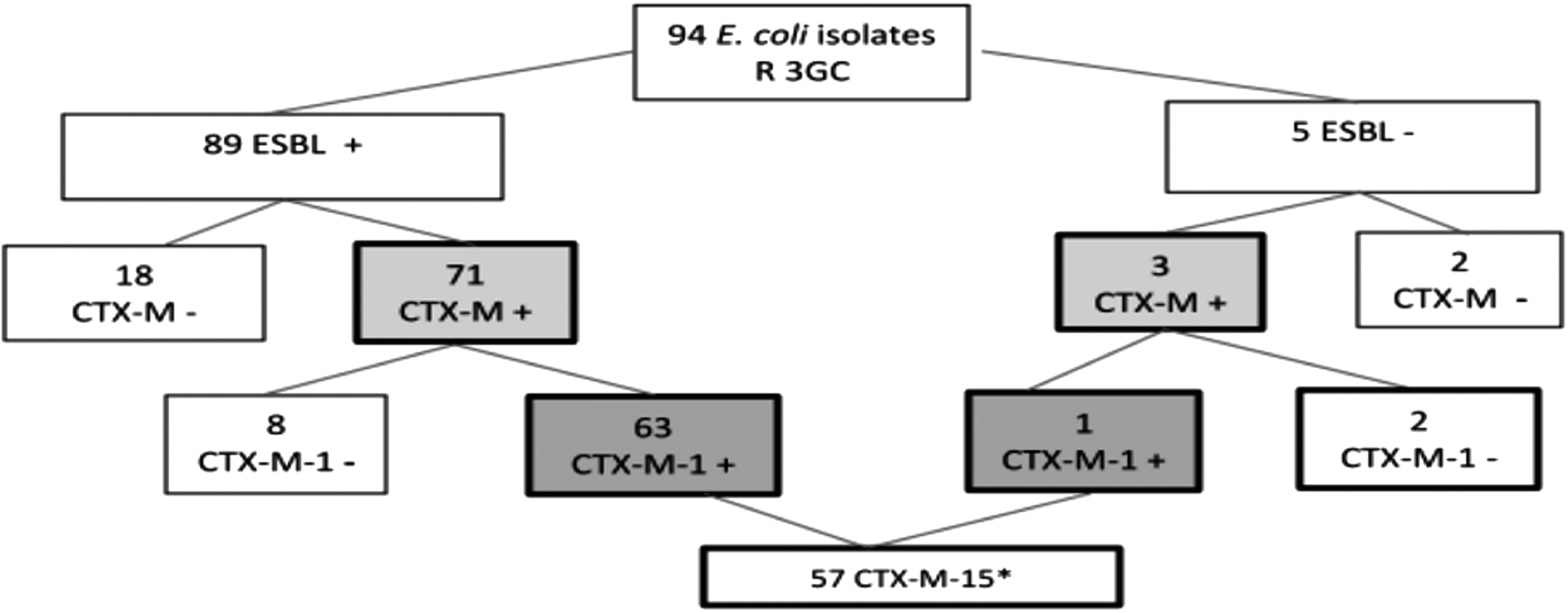
Schematic representation of the blaCTX-M and blaCTX-M-1 gene determination results. *Sequencing results from nonclonal ERIC-PCR isolates. +, positive; −, negative; ERIC-PCR, enterobacterial repetitive intergenic consensus-polymerase chain reaction; ESBL, extended-spectrum β-lactamases.
blaCTX-M-1 sequencing
By sequencing the amplicons obtained by PCR, we were able to identify the specific mechanism of resistance (n = 57). CTX-M-15 confers resistance to cefotaxime and ceftazidime and presents high rates of prevalence in Ecuador, indicating great dissemination of this variant in urinary isolates of E. coli.
ERIC-PCR
ERIC-PCR showed that the dissemination of this mechanism of resistance is not due to clonal expansion. A high degree of genetic heterogeneity was found between all blaCTX-M-1-positive isolates (n = 64). We found 57 clonal patterns, indicating that the dissemination of resistance might be due to horizontal gene transfer. Ten electrophoretic patterns were formed by two strains each, with 100% similarity. Four patterns agreed only in the year of isolation, while we could not find any relationship between the strains that composed the other patterns in the data studied (age, sex, and date of collection) (Fig. 3).
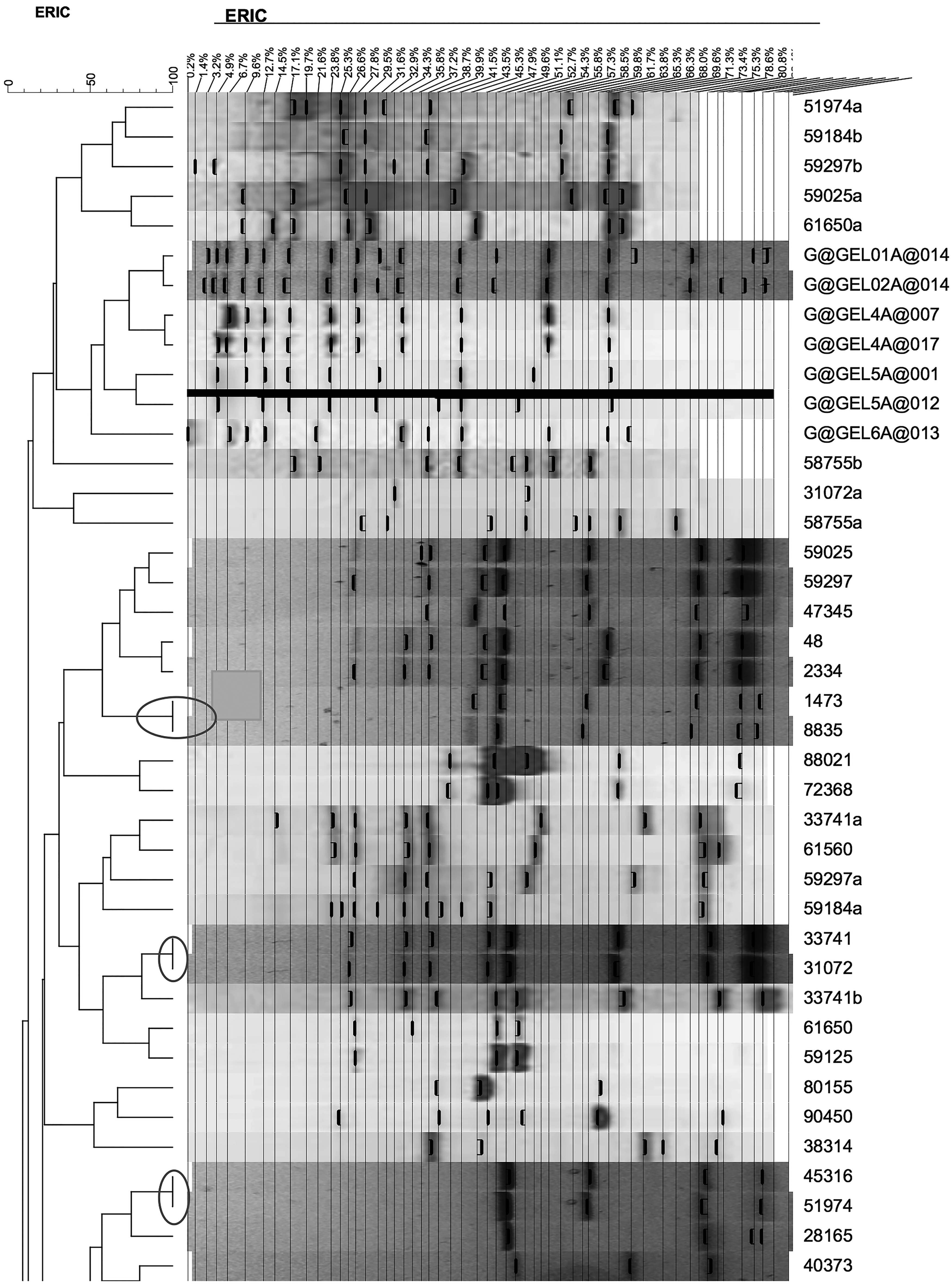
Dendrogram made from electrophoretic patterns obtained by ERIC-PCR showing a nonclonal dissemination of E. coli CTX-M positive.
Relationship between the presence of CTX-M-1, age, sex, and resistance to other groups of antibiotics
There was no association between the presence of CTX-M-1 group and any age group or sex (p = 0.96); however, statistical significance was confirmed between resistance to ciprofloxacin (p < 0.05) and CTX- M-1 group, as well as the sensitivity to amikacin and the presence of CTX-M-1 (p = 0.001). No significant p-values were found between CTX-M-1 group and nitrofurantoin, fosfomycin, or trimethoprim/sulfamethoxazole. Altogether, these results indicate that we did not find an association between resistance and patient, only with coresistance to ciprofloxacin.
Discussion
Our results showed a gradual increase in resistance to 3GC, similar to that reported in other countries where antibiotic consumption is not controlled. 24 The SMART study (Study for Monitoring Antimicrobial Resistance Trends) 11 performed in ten Latin American Countries (Argentina, Brazil, Chile, Colombia, Dominican Republic, Guatemala, Mexico, Panama, Peru, and Venezuela) showed that 12% of E. coli isolates harbored an ESBL in 2004, while from 2009 to 2010, an increase of 23% in resistance is reported. 11 Similarly, the TREND study (Tigecycline Evaluation and Surveillance Trial) performed in Argentina, Brazil, Chile, and Mexico between 2004 and 2006 reported a prevalence of 24% of resistance to 3GC in Latin America, but also describes an increase in resistance to 3GC during the years of study. 12 Similarly, in Europe and Asia-Pacific region, several authors report an increased resistance to cephalosporins in Enterobacteriaceae.24,25 Importantly, these studies do not discriminate between community- and hospital-acquired isolates, and neither type of infection allows us to know whether the resistance is higher in hospital or community settings; however, the overall increase in resistance is clear.
Rates of UTI produced by E. coli in the community settings vary according to the country and time frame of the study. Kahlmeter et al. 26 reported a prevalence of ESBL of 4.8% in several European countries in 2014. Similarly, Mexico (2006–2007), Colombia (2011), and Peru (2012) have reported the presence of ESBL of 10.2, 12.52, and 12.3%, respectively,27–29 which is similar to that found in our study. Importantly, countries such as India register rates as high as 41.6%. 30
Uncontrolled and excessive consumption of antibiotics, self-medication, and unregulated use of antibiotics in animals for human consumption are key factors associated with the increased resistance observed in this study.31,32 It has been reported that poor handling of meat and vegetables is involved in the maintenance and propagation of multidrug-resistant strains, and it has been associated with dissemination of E. coli harboring CTX-M-like beta-lactamases.33,34
Twelve E. coli ESBL isolates belonged to patients younger than 5 years, which suggests the presence of risk factors in pediatric settings for contracting UTIs caused by E. coli carrying ESBL. 35 A limitation in our study was the absence of clinical data, which did not allow us to explore further conclusions. However, due to the low frequency of resistance to antibiotics in the pediatric settings, we can conclude that these patients had some risk factors such as renal pathology, which required hospitalization and increased the risk for colonization and subsequent infection by this microorganism.
The presence of the blaCTX-M gene was found to be 79%, matching that reported in a previous study in Ecuador. 36 Similarly, another study detected a prevalence of ∼64% in 140 E. coli isolates obtained from hospitalized patients, including clinical samples of different origins. 37 Our samples were from a community setting, not hospital-acquired infections, and demonstrate a surprisingly higher level of resistance than in the hospital isolates.
High prevalence of CTX-M-15-like resistance has been reported in E. coli from several studies conducted in the Latin American region,38–40 including Argentina. 41 In our study, we identified CTX-M-15-like in 77.02%% of the studied isolates, similar to what Zurita et al. 37 reported previously in Quito. This contrasts with the results of León in 2014, who reported CTX-M-28 as the most prevalent resistant mechanism (66%) in clinical isolates of various Enterobacteriaceae in Quito. 16
Menezes et al. 42 have warned about the possibility of erroneous identification between the CTX-M-28 and CTX-M-15 variants due to inadequate selection of the primers used, and in this study, we carefully chose primers to avoid misidentification of the CTX-M gene present.
In our study, we have found that CTX-M-like was significantly correlated with resistance to other antibiotics. Coresistance with other groups of antibiotics such as quinolones has been described previously, and this is attributed to the colocalization of CTX-M with the modifying enzyme of the aac (6′) -Ib-cr type in the same plasmid. 43 Coresistance with quinolones has also been observed in our study with a statistically significant result.
Clonal analysis revealed the presence of high genetic diversity between the studied isolates, suggesting that dissemination of the ESBL might be due to horizontal gene transfer. Mshana et al. 44 (2009) did not find a clonal pattern between the CTX-M-15 E. coli isolates analyzed, showing that dissemination of this CTX-M-like enzyme in the hospital unit was due to the horizontal dissemination of conjugative plasmid IncFI. Unfortunately, due to budget restriction, we could not perform restriction fragment length polymorphism studies in plasmids or multilocus sequence typing techniques that would allow us to better understand the dissemination route.
Conclusion
The prevalence of uropathogenic E. coli ESBL isolates increased over the 6 years of the study, being predominantly the CTX-M-15 type. The results of ERIC-PCR electrophoretic patterns demonstrated that the dispersion of this resistance mechanism is not clonal and that the resistance to 3GC by ESBL CTX-M type is associated with coresistance to ciprofloxacin. The data obtained indicate the need to implement national surveillance that allows monitoring of this mechanism of resistance in the urological isolates of the community due to the high frequency found.
Footnotes
Acknowledgments
The authors thank Jeanette Zurita, MD, for providing the strains used as controls and the National Institute of Public Health Research, Dr. Leopoldo Izquieta Pérez, Ecuador, for the use of laboratories. The authors also acknowledge Miss Lindsey Taylor Whitesides for her English editing. Funding: Funds for research were provided by the Sosegar Clinical Laboratory.
Disclosure Statement
No competing financial interests exist.