
Abstract
Staphylococcal surface protein sasX is a colonization mediating virulence factor in ST239 methicillin-resistant Staphylococcus aureus (MRSA) strains, which potentially contribute to its successful establishment. We aimed to study the presence and dissemination of sasX in clinical MRSA isolates and among MRSA carriers. A total of 450 nonduplicate clinical MRSA isolates recovered from blood cultures between 2013 and 2017 were included in this study. In addition, 93 nasal swabs were collected from patients receiving hemodialysis, after obtaining consent and screening for MRSA colonization. sasX polymerase chain reaction and sequencing were carried out for all isolates. Multilocus sequence typing was performed for all sasX-positive isolates. Of the tested clinical MRSA isolates, 11% (n = 48) were positive for sasX gene. Among hemodialysis patients, 26% (n = 24) were characterized as MRSA carriers. However, all MRSA strains isolated from nasal swab were negative for sasX gene. Overall, we observed 10% (11% in clinical MRSA isolates and 0% in MRSA carriers) of sasX-positive MRSA in this study. ST239 and ST368 were the predominant sasX carrying MRSA lineages. The majority of sasX carrying MRSA strains were characterized as Staphylococcus epidermidis surface protein I (sesI; 71%), a sasX homolog native to S. epidermidis. This study highlights the dissemination of sasX/sesI to ST368 (CC8), ST3324 (CC8), ST772 (CC1), and ST22 (CC22). The presence of S. epidermidis-specific invasive factor sesI in clinical MRSA strains provides evidence for horizontal transfer between these closely related species.
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA)-associated infections are a major concern and a global source of morbidity and mortality. Intravascular devices and hemodialysis are the major risk factors for the acquisition MRSA in hospitals. The hospital-acquired MRSA (HA-MRSA) strain ST239, which harbors staphylococcal cassette chromosome mec (SCCmec) type III lineage, has been reported with multiple epidemics and hospital outbreaks across the world.1,2
Recent literature reveals that the pathogenic success of the ST239-SCCmec III lineage is due to sasX gene, which codes for a cell wall-associated surface protein. 1 This prophage-mediated virulence determinant (sasX) is crucial for the colonization, immune evasion, and subsequent invasion of S. aureus. Thus, adding high potential for dissemination enhanced virulence and bacterial fitness. In addition, sasX has shown high similarity to ϕSPβ-encoded Staphylococcus epidermidis surface protein I (sesI), a marker of invasion for S. epidermidis RP62A. 3
This study is proposed to (1) determine the presence of sasX among MRSA isolates recovered from blood cultures, (2) determine the dissemination of prophage-mediated sasX to other lineages, (3) do a variant analysis of the sasX gene, (4) investigate the frequency of Panton–Valentine leukocidin (PVL) among the sasX-positive MRSA strains, (5) determine the resistance profile of sasX harboring MRSA lineages and (6) determine the nasal colonization of sasX carrying MRSA strains.
Materials and Methods
Strain collection
A total of 450 nonduplicate MRSA clinical isolates recovered from blood cultures between 2013 and 2017 were included in this study. The study was conducted at a 2,600-bedded tertiary care centre, Christian Medical College, Vellore, India. In addition, 93 nasal swabs were collected in the year 2017 (January to December) from patients receiving hemodialysis, who attended the nephrology unit at this hospital, after obtaining consent and screening for MRSA colonization. This study was approved by the Institutional Review Board (IRB No. 10683 dated June 2017) of Christian Medical College, Vellore. Identification of S. aureus was carried out using colony morphology, Gram staining, the catalase test, and the tube coagulase test. 4 Methicillin resistance in S. aureus was assessed using cefoxitin disk diffusion (DD) testing. 5 A standard questionnaire was used to collect information of the timing of culture, health care risk factors, and patient comorbidities. Data obtained from clinical MRSA isolates and carrier MRSA strains were analyzed individually.
Epidemiological criteria for MRSA infection
The centre for disease control (CDC) epidemiological definition was used for classification of community-acquired (CA) and HA-MRSA infections. 6 Accordingly, MRSA infection can be considered as HA; when an MRSA recovered from cultures obtained >48 hours after hospital admission. An HA-invasive MRSA infection is when an MRSA is isolated from sterile site cultures, >48 hours after hospital admission. According to CDC definition, HA-MRSA and HA-invasive MRSA cases have been associated with the following health care risk factors in the previous 12 months: surgery, hospitalization, hemodialysis, history of MRSA infection or colonization, presence of an indwelling vascular catheters at the time of admission or a stay in a long-term care facility. In contrast, an infection is considered CA-MRSA, when an MRSA identified from cultures obtained in <48 hours of hospital admission and with no documented health care risk factors.
Antimicrobial susceptibility testing
Antimicrobial susceptibility testing was performed using the DD method, according to the Clinical and Laboratory Standard Institute (CLSI) guidelines. 7 All sasX-positive MRSA isolates (n = 48) and MRSA isolates (n = 24) from nasal swabs were tested against the following antibiotics: cefoxitin (30 μg), gentamicin (10 μg), erythromycin (15 μg), clindamycin (2 μg), tetracycline (30 μg), ciprofloxacin (5 μg), co-trimoxazole (1.25/23.75 μg), rifampicin (5 μg), linezolid (30 μg), and high-level mupirocin (200 μg). The broth microdilution (BMD) method was used to determine the minimum inhibitory concentration (MIC) of vancomycin. 8
Molecular characterization
Genomic DNA was extracted using QIAamp DNA Mini Kit (Qiagen, Germantown, MD) according to the manufacturer's instructions. Subsequently, all isolates were confirmed as MRSA using mecA polymerase chain reaction (PCR), as previously described. 9
Screening of sasX and PVL genes
All MRSA isolates were screened for the presence of sasX (522 bp) using the primers, sasX-f (5′-agaattagaagtacgtctaaatgc-3′) and sasX-r (5′-gctgattatgtaaatgactcaaatg-3′) as described by Li et al. 1 For the confirmation of the identity/variant, all sasX PCR products were sequenced using an ABI-prism 3500 genetic analyzer (Applied Biosystems). For the homology analysis, sasX allele of TW20 (accession No. FN433596), TOHH628 (accession No. LC036194), and S. epidermidis RP62A sesI gene (accession No. CP000029.1) were used as the reference sequence. Alignment of the retrieved sequences was performed using multiple-sequence alignment (MSA) supported by Clustal-W as applier in the BioEdit software, version 7.0.9.1. 10 Carriage of the PVL toxin gene was determined for all sasX-positive MRSA isolates by the amplification of nucleotide fragment of 433 bp located in the lukS and lukF operon using PCR as described earlier. 11
Molecular typing
SCCmec typing and multilocus sequence typing (MLST) was performed for all sasX-positive MRSA isolates. SCCmec types I, II, III, and V were determined by using multiplex PCR strategy.12,13 MRSA isolates were screened for SCCmec IV subtypes (a, b, c, d, g, and h) as described earlier. 14 Control strains for SCCmec types I, II, III, IV, and V were procured from the Biodefense and Emerging Infections (BEI) Research Resources Repository. MLST was performed as per Enright et al. 15 The allelic profile of each loci was identified through the comparison of obtained sequence with the known sequences deposited in S. aureus MLST database. a MRSA clones were defined using the nomenclature MLST-SCCmec type.
Parameters used for phylogenetic tree construction
The phylogenetic tree was constructed in MEGA 7. 16 The maximum likelihood method was based on the Tamura–Nei model. The gaps or missing data treatment was carried out with pairwise distance estimation (pairwise deletion option) with the bootstrap consensus of 100 replicants. Initial tree for the heuristic search was obtained by applying the neighbor-joining method to a matrix of pairwise distances estimated using the maximum composite likelihood approach.
Results
Epidemiology of clinical MRSA isolates
Overall, the prevalence of MRSA was 33% (n = 450) during the study period. Of the tested clinical MRSA (n = 450) isolates, 11% (n = 48) were positive for sasX gene and 66% (n = 298) carried PVL gene. Among the sasX-positive MRSA isolates, 52% (n = 25) were PVL positive. SCCmec typing showed that 71% (n = 34) of sasX-positive MRSA isolates carried SCCmec III, followed by 13% (n = 6) of SCCmec V, 6% (n = 3) of SCCmec IVc and 4% (n = 2) of SCCmec I. Remarkably, a combination of SCCmec III and V was observed in three sasX-positive isolates.
MLST analysis of sasX-positive MRSA strains revealed five different sequence types (ST); 48% (n = 23) of ST239, 35% (n = 17) of ST368, 13% (n = 6) of ST22, and one isolate each with ST772 and ST3324 (Fig. 1). The predominant lineage was 40% (n = 19) of ST239-SCCmec III followed by 27% (n = 13) of ST368-SCCmec III. Moreover, ST368 and ST3324 were single-locus variants (SLV) of ST239 at the loci tpi and pta, respectively. Notably, sasX-positive clones ST239 (n = 11), ST368 (n = 6) and all ST22 (n = 6) also carried the PVL gene.

A maximum likelihood phylogenetic tree was constructed for 48 sasX-positive MRSA isolates using concatenated sequences of 7 housekeeping genes included in this study. The tree was constructed in MEGA V.7.0 and edited with iTOL V.4.2.3. The tree was annotated with the year of isolation, health care- or community-acquired MRSA, sasX/sesI gene positivity, clonal complex, STs, SCCmec type, antimicrobial resistance profile, and PVL. MRSA, methicillin-resistant Staphylococcus aureus; PVL, Panton–Valentine leukocidin; SCCmec, staphylococcal cassette chromosome mec; sesI, Staphylococcus epidermidis surface protein I; STs, sequence types; SXT, trimethoprim–sulfamethoxazole. Color images are available online.
Nucleotide homology of sasX in clinical MRSA isolates
The sasX gene of the reference genome (TW20/TOHH628) exhibited 95.8% nucleotide/94.8% amino acid identity to S. epidermidis RP62A sesI gene. A phylogenetic tree was constructed, based on the homology between sasX and sesI, which were identified in the tested strains (Fig. 2). Among sasX-positive isolates, 29% (n = 14) of strains belonged to ST239 and ST368 showed 100% homology to the sasX gene of TW20 and TOHH628 at the nucleotide level. Notably, one sasX-positive isolate (B34962) showed deletion of seven nucleotides (AGCTCAG) at the position 309–315, which resulted in a truncated sasX protein. Whereas 71% (n = 34) of ST239, ST368, ST3324, ST22, and ST772 sasX-positive strains exhibited 100% homology at the nucleotide level to the sesI of S. epidermidis RP62A.
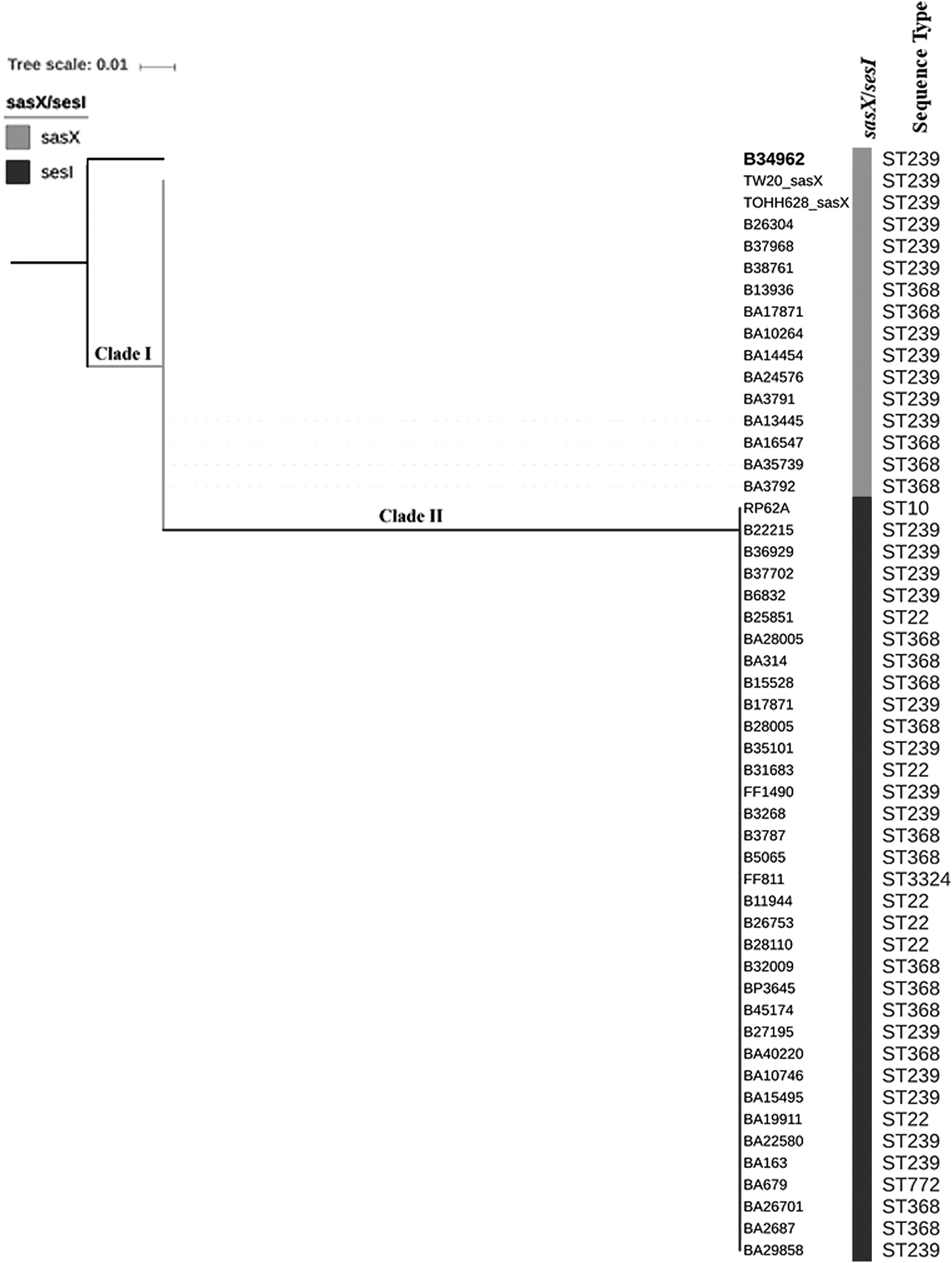
A maximum likelihood phylogenetic tree was constructed based on the nucleotide sequence homology of sasX (S. aureus) and sesI (Staphylococcus epidermidis) for all sasX-positive isolates using MEGA V.7.0. The clade I (gray) showed 100% homology to sasX of ST239 reference genome TW20 (accession No. FN433596) and TOHH628 (accession No. LC036194). Whereas clade II (black) showed 100% homology to the native sesI of S. epidermidis RP62A (accession No. CP000029.1). An isolate (B34962) showed deletion of seven nucleotides (AGCTCAG) at the position 309–315 in sasX gene (boldface).
Epidemiology of MRSA carrier isolates
Of the 93 subjects, 26% (n = 24) were characterized as MRSA carriers, which was confirmed with mecA gene. All MRSA isolates from these carriers were negative for sasX gene. Similarly, all were negative for PVL, except two isolates (Fig. 3). SCCmec IV was the predominant type and was found in 54% (n = 13) of MRSA carriers, the second most common SCCmec type was 38% (n = 9) of SCCmec V. The distribution of ST among MRSA isolates from nasal swabs was as follows: 33% (n = 8) of ST22, 29% (n = 7) of ST772, 12% (n = 3) of ST6 and two isolates each with ST672, ST1037, and ST2371 (Fig. 3). Nucleotide analysis of MLST marker genes showed that ST1037 (arcC) and ST2371 (aroE) were SLV of ST22, the primary founder of CC22.

A maximum likelihood phylogenetic tree was constructed for 24 MRSA using concatenated sequences of 7 housekeeping genes that define STs. The tree was constructed in MEGA V.7.0 and edited with iTOL V.4.2.3. The tree was annotated with the following metadata that includes clonal complex, STs, SCCmec types, PVL, and antimicrobial resistance profile of MRSA isolated from the nasal swabs of hemodialysis patient. Color images are available online.
Antimicrobial susceptibility testing of clinical and carrier MRSA isolates
All sasX-positive clinical MRSA isolates (n = 48) were susceptible to vancomycin with an MIC of ≤1 μg/mL and linezolid. Isolates of different genetic lineages displayed different resistance profiles (Fig. 1). Two major group of strains stratified by MLST and SCCmec type, ST239 (n = 19) and ST368 (n = 13) carrying SCCmec III were included for antimicrobial resistance analysis. Whereas a small number of MRSA isolates belonging to other ST-SCCmec types exhibited variable resistance profiles. ST239-III and ST368-III were found to be multidrug-resistant (≥3 non-beta lactam antibiotic) and showed 100% resistance to gentamicin, erythromycin, tetracycline, and ciprofloxacin. ST368-III (69%) was less likely to be resistant to clindamycin than ST239-III (100%). Resistance to rifampicin was rarely seen in ST239/ST368 strains.
All MRSA strains isolated from carriers (n = 24) were susceptible to minocycline, rifampicin, high-level mupirocin, vancomycin (MIC, ≤1 μg/mL), and linezolid. The antimicrobial resistance profiles and genotypes of MRSA isolates from the nasal swabs of hemodialysis patient are shown in Fig. 3.
Clinical characteristics of MRSA patients and carriers
Among sasX-MRSA-infected patients (n = 48), 75% (n = 36) were men and 25% (n = 12) were women with a gender ratio of 3:1. The majority, 83% (n = 40), had HA-MRSA infection. Eight (17%) had ST239/ST368-SCCmec III-associated HA-MRSA infection after a burn injury. Fifteen (31%) of the patients died, of which six were infected with ST239-III MRSA and eight with ST368-III strains. Clinical investigation showed that 42% (n = 20), 15% (n = 7), and 21% (n = 10) of patients had a history of diabetic mellitus, chronic renal failure, and diabetic foot ulcer, respectively. Furthermore, 12 patients had a history of prior hospitalization in the past 6 months.
Among MRSA carriers, 19 were men and 5 were women with a median age of 43 years (range, 19–72 years). The most common indication for dialysis initiation was chronic kidney disease stage V in 23 out of 24 patients. Among these patients, 42% (n = 10) had a history of diabetes mellitus, but none of them were diagnosed with a diabetic foot ulcer.
Discussion
Since 1970s, ST239-SCCmec III has been the pandemic HA-MRSA lineage circulating in many countries. 17 In 2010, sasX was first identified in an ST239 strain, which caused an outbreak in a hospital intensive care unit in London. 18 Recently, Li et al. provided evidence for the functional role of sasX in promoting nasal colonization and invasion. 1 Subsequently, several studies have reported sasX in the ST239-SCCmec III lineage.16–21 Although, sasX is frequently associated with the ST239 lineage, dissemination to other STs has also been reported. 1 In addition, the sasX gene has showed 95% amino acid identity to sesI, a potential marker for invasion in S. epidermidis. 3
In this study, we attempted to investigate the presence of sasX in clinical MRSA strains and MRSA from carriers. Overall, we observed 10% (11% in clinical MRSA isolates and 0% in MRSA carriers) of sasX-positive MRSA isolates in this study. Similar to previous reports, ST239-SCCmec III was observed to be the predominant sasX carrying lineage in this study.19–21 For the first time, this study reported sasX in ST22 (13%) and ST772 lineages. In the literature, studies have reported the presence of sasX in other lineages, including ST5, ST45, and ST59 MRSA strains.1,18,20 These consolidated findings have marked sasX as a rapidly disseminating virulence determinant.
It was believed that sasX was acquired from coagulase negative S. aureus (CoNS) through ΦSPβ-like prophage. For a better understanding of this hypothesis, all isolates were investigated for sasX nucleotide homology. In addition, whole genome sequencing of ST239 strain (data not shown) was performed for the identification of ΦSPβ-like prophage. This whole genome analysis confirmed the presence of sesI on ΦSPβ-like prophage (accession No. MLQB00000000).
Nucleotide analysis of sasX gene revealed that the majority (71%) of strains showed 100% identity to sesI of S. epidermidis RP62A. De Backer et al. have previously reported a similar observation among Indian MRSA isolates (ST239 and ST368) carrying the sesI gene. 22 This evidence suggests that sasX was acquired from CoNS through ΦSPβ prophage. In addition to multidrug resistance, sasX acquisition promotes adaptive advantage and persistence of ST239-III/ST368-III lineages in hospital settings.1,2,22
In China, ST239-SCCmec III is the predominant HA-MRSA lineage. 23 In parallel to this endemicity, increasing frequency of sasX-positive MRSA (21% in 2003 to 39% in 2011) was reported in China. 1 However, a similar trend was not observed in this study. This could be due to the low prevalence of the ST239-SCCmec III lineage in India.24,25
Although, PVL is a genetic marker and a common virulence factor carried by CA-MRSA, 26 several studies have described PVL-positive HA-MRSA in their settings.24–29 Among HA-MRSA clones, PVL was also frequently reported in ST239 strains.30–33 Consistently, this study revealed the presence of PVL in ST239 and ST368 strains. This increasing incidence of PVL-positive HA-MRSA strains is of great concern and may potentially worsen MRSA infection.
Strong evidence suggests an association with S. aureus nasal colonization and infection. 34 Certainly, dialysis access significantly contributes to MRSA colonization. 35 MRSA colonization in hemodialysis patients has been linked with a 2.46-fold higher risk for all-cause mortality. 36 In this study, we evaluated MRSA colonization among hemodialysis patients and found 26% were nasal carriers. Studies have estimated the incidence of MRSA nasal to be between 1% and 27% in hemodialysis patient. 37 The rate substantially varies with the age, screening sites, and MRSA endemicity.
In this study, sasX harboring MRSA carriers were not observed. In contrast, a study from Malaysia has reported sasX carrying MRSA isolates from the nasal swabs of healthy individuals. 38 In this study, ST22-SCCmec IVd and ST772-SCCmecV were identified as the predominant MRSA lineage in carriers, which concurs with an earlier report from India. 39
Conclusion
In this study, 10% of sasX-positive MRSA strains were identified. Further confirming the predominance of sasX/sesI in ST239 and ST368 MRSA strains. Dissemination of sesI to other STs, including ST3324, ST22, and ST772, were observed among the tested isolates. The presence of MRSA harboring sasX/sesI and PVL highlights the potential risk for dissemination and increased virulence. This may impact the management of invasive MRSA infection. The most remarkable finding of this study was the acquisition of native sasX homolog, sesI from S. epidermidis. These aforementioned findings reflect the evolution and dynamics of sasX/sesI dissemination.