
Abstract
Tuberculosis (TB) is a major issue in global health and affects millions of people each year. Multidrug-resistant tuberculosis (MDR-TB) annually causes many deaths worldwide. Development of a way to diagnose and treat patients with MDR-TB can potentially reduce the incidence of the disease. The current study reviews the risk factors, pattern of progression, mechanism of resistance, and interaction between bacteria and the host immune system, which disrupts the immune response. It also targets the components of Mycobacterium tuberculosis (Mtb) and diagnosis and treatment options that could be available for clinical use in the near future. Mutations play an important role in development of MDR-TB and the selection of appropriate mutations can help to understand the type of resistance in patients to anti-TB drugs. In this way, they can be initially treated with proper and effective therapeutic choices, which can accelerate the course of treatment and improve patient health. Targeting the components and enzymes of Mtb is necessary for understanding bacterial survival and finding a way to destroy the pathogen and allow patients to recover faster and prevent the spread of disease, especially resistant strains.
Introduction
Tuberculosis (TB) is an important global health issue that causes millions of deaths annually. The World Health Organization reports that in 2017, 10 million new cases of TB were reported (5.8 million men, 3.2 million women, and 1.0 million children). About 1.3 million deaths were of HIV-negative individuals and 300,000 deaths were of HIV-positive individuals, for a total of 1.6 million. India, China, Indonesia, Philippines, Pakistan, Nigeria, Bangladesh, and South Africa were responsible for two-thirds of those stricken with the disease. The fastest decline in the population of TB patients over the last 5 years is in Europe, which reported a 5% decrease in new patients every year. 1
A multidrug regimen, prolonged treatment, and the prevalence of multidrug resistance are problems associated with TB. 2 It is estimated that 3.5% of new cases and 18% of previously treated cases involve multidrug-resistant tuberculosis (MDR-TB). Only 55% of patients diagnosed with MDR-TB have been treated successfully. With this in mind, the need for diagnosis and treatment of patients is urgent and drug sensitivity tests with wider coverage should be done for those diagnosed with TB. Some patients continue to treat themselves, but medical regimens are considered more effective and safer for these patients. 1 Therefore, there is an urgent need for effective therapeutic development to fight latent infection and MDR-TB. This article reviews the available scientific data in an effort to help develop new perspectives on preventing the spread of drug-resistant tuberculosis (DR-TB).
Risk Factors, Patient Management, and Resistance
Various risk factors make people exposed to Mycobacterium tuberculosis (Mtb) more susceptible and vulnerable and can cause problems in treating these patients. For instance, in treating patients, old age can be proposed as a deterrent agent, thus the success rate of treatment of elderly patients with MDR-TB is lower than that of younger patients and their mortality rate is higher. 3
The presence of illnesses such as HIV can make treatment more difficult. In HIV patients with a prior history of TB treatment, if it was not completely cured, exogenous Mtb infection may suppress the immune system and reactivate the prior infection. 4 In addition, the rate of resistance to anti-TB drugs in people with HIV is higher. 5 Therefore, HIV-positive patients with DR meningitis have severe clinical manifestations with high mortality rates. 6 Diabetes mellitus is also associated with DR-TB and high mortality rates.7,8 It increases the risk of rifampin (RIF) resistance in patients with diabetes. 9 In addition, patients who are underweight are more at risk for side effects and death, which highlights the importance of complementary diets along with anti-TB treatments, 10 whereas addiction to alcohol, smoking and drug addiction are not associated with the prevalence of drug resistance. 5
Generally, DR-TB is associated with an increased risk of death during treatment. 7 Therefore, testing second-line drugs at the onset of resistance can help identify patients requiring special treatment to prevent the risk of treatment failure and death. 11 For example, the increased prevalence of pyrazinamide resistance (PZAR) may indicate the importance of conventional drug susceptibility testing of pyrazinamide (PZA) and Mtb genotyping to identify, control, and prevent the growth of resistant organisms. 12
Spreading resistance can lead to exacerbation of the disease and increase in the rate of tissue damage. For instance, resistance to ethambutol causes chronic infection and loss of lung function and, with continued bacterial survival, TNF-α expression will increase the pathology of the lung. 13 Therefore, early diagnosis and reporting of adverse drug reactions can significantly reduce the spread of resistant strains and damage to tissue caused by resistance. 14
The hospital costs of DR-TB treatment, especially in patients with advanced resistance or treatment failure, are very high. 15 Thus, managing patients before the start of treatment by designing a good building with airflow, isolation, decontamination, and respiratory protection, especially for patients with extensively drug-resistant tuberculosis (XDR-TB) who did not have good treatment with conventional drugs, is essential. 16
Resistance Mechanisms
Mtb has two main mechanisms for intrinsic resistance: highly active β-lactamase and very low permeability of the outer membrane. In the cell wall, β-lactamase is linked to different enzymes. Inhibition of these enzymes can lead to cell death through various mechanisms by disturbing the balance of peptidoglycan metabolism. 17 Acquired resistance is also very common. Efflux pumps play a role in resistance to isoniazid (INH) by MDR strains, especially in strains without mutations in katG, inhA, and oxyR-ahpC. The difference in expression of some of the genes of these pumps in resistant and sensitive strains can be useful in the diagnosis and treatment of resistant strains. It should be noted that efflux pumps, without pumping out antitubercular drugs, regulate the intracellular level of nutrients and cofactors. 18
The prevalence of resistance in children is significant. A high percentage of resistance in children can be indicative of transmission from adults and should be given special attention. 19 In rifampin-resistant strains, CK-2 (casein kinase 2)-mediated phosphorylation of Hsp90β (heat shock protein 90β) is an important molecular mechanism that regulates the expression of P-gp (P-glycoprotein) because its expression is an important factor in resistance to rifampin. Thus, rifampin catalyzes Hsp90β phosphorylation by activating CK-2. Phosphorylated Hsp90β reacts with PXR (pregnane X receptor) and sustains it, leading to P-gp expression; therefore, inhibition of Hsp90β and CK-2 can reduce the expression of P-gp. 20 The occurrence of mutations in rpoB can also lead to resistance to rifampin. Although a single mutation in the S531L region of the rpoB gene can be the cause of resistance, a double mutation in rpoB (S531L, V615M) with a minimum inhibitory concentration (MIC) much higher than that for a single mutation in resistant strains increases resistance to this drug, indicating a role in successful transmission of these strains. 21
Manu2 lineage, which plays a prominent role in mixed infections by influencing the host immune response, is a possible mechanism for resistance to rifampin in nonmutated isolates in the rpoB gene. 22 Polymorphism in the 677G>A allele of the ABCB1 gene may also be associated with rifampin and ethambutol resistance. The possible mechanism for this resistance is 893Ala/Thr replacement in P-gp, which facilitates development of DR-TB. 23 In addition, mutation in the embB codon 306 may lead to resistance to ethambutol. The single nucleotide polymorphism of this codon is an attractive biomarker for screening for resistance to various drugs. 24
Ethambutol targets the cell wall through interaction with arabinosyltransferase involved in arabinogalactan biosynthesis and then inhibits polymerization of the arabinan of arabinogalactan. 25 Most mutations in the gyrA gene at codon 94 can result in high levels of resistance to gatifloxacin and moxifloxacin and reduce the effectiveness of treatment in patients with MDR-TB when treatment by injection is still effective. 26 Mutations of gyrB can result in resistance to fluoroquinolones (ofloxacin and moxifloxacin) either alone or along with gyrA mutations at particular loci. 27
PZAR is related to the frequency of pncA mutations; therefore, identification of these mutations can help with selection of appropriate anti-TB drugs.28–30 Although there is controversy about the relationship between resistance to PZAR and the panD gene, it has been shown that mutation of histidine to arginine at subunit 21 (H21R) and mutation of isoleucine to valine at subunit 49 (I49V) at the inactive position of the gene lead to PZAR. 31 However, some studies have reported that mutations of the panD gene do not relate to this resistance. 30
Streptomycin resistance is also associated with the mutation of rpsL in codons 43 (K43R; high-level mutation) and 88 (K88R) and rrs genes (low-level mutation), as well as deletion mutations in the gidB gene (low-level dual mutation in E92D and A205A).32,33 In creation of resistance to trimethoprim, point mutation E84G in the dihydrofolate reductase enzyme gene may also occur. 34 Mutations in rv0678 of the addition and removal of nucleotide G at position 193 (mutations in T1052C), rv1979c (V351A change in amino acids), and rv2535c (mutation in E89) also are important mechanisms for inducing resistance to clofazimine. 35
Drug resistance mutations can reduce virulence in these strains. 36 Although resistant strains have a slower and longer replication time, they can survive because of fast adaptation to repair mechanisms and the release of repaired DNA. 37 In general, selection of a limited number of target mutations enables us to detect a wide range of drug resistance profiles, although in countries with poor resources, phage amplification technology can be useful in identifying MDR strains. 38 The genes involved in development of drug resistance along with the relevant mutation are listed in Supplementary Table S1.
Targeting of Mtb Components
A strategy for disease prevention and the spread of resistant strains is to target different parts of bacteria. Targeting of the membrane of Mtb, which eliminates bacteria, can be done by chemotherapy and is a good way to slow down progression of genetic resistance and eventually shorten the duration of anti-TB regimens. Boromycin is an ionophore for potassium ions that decrease intracellular ATP levels, leak cytoplasmic proteins, damage the cell membrane, and act as potent inhibitors for the growth of DR-TB strains with prominent bactericidal activity. 39
While inhibition of synthesis of arabinogalactan and mycolic acid remains a primary target for drugs, mechanisms for the transfer and synthesis of peptidoglycan and decaprenyl phosphate carrier lipids are also interesting targets. 40 Likewise, mycobacterial membrane protein large (MmpL), which plays a vital role in transmission of lipids in the pathogen, is a possible drug target. The combination of SQ109 as an inhibitor of type 3 of this protein synergistically with anti-TB drugs shortens the treatment period. This compound, as an analog of ethambutol (inhibiting the synthesis of trehalose dimycolate), prevents the connection of mycolates to arabinogalactan in the cell wall. MmpL3 transmits trehalose mycolate. 41 Indole carboxamides, adamantyl urease, tetrahydropyrazolopyrimidine, and diarylpyrrole BM212 can inhibit transmission of MmpL3, probably by their abilities to eliminate the transmembrane electrochemical proton gradient. 42 Efflux pump mechanisms involved in detoxification of intracellular metabolites and cell homeostasis may be inhibited by thioridazine compounds. They have been found to have a high capacity for efflux inhibition as well as low toxicity and significant synergistic effects with anti-TB drugs both in vitro and in macrophages. These compounds can be used as auxiliary drugs for treatment of TB. 43
It has been shown that AZD5847, a new anti-TB agent, has a good effect against Mtb by inhibiting protein synthesis and its use during the primary bactericidal phase and sterilization stage of treatment can be beneficial. 44 Mtb shows enzymatic activity for which compounds can affect the growth and survival of bacteria and inhibit enzymes. The antigen, 85 Mtb, features mycolyl-transferase activity that produces trehalose dimycolate. The substrate analogs of this enzyme inhibit bacterial growth. The new inhibitor of 85C antigen, I3-AG85, in infectious macrophages prevents bacterial survival and can be used as a target for controlling DR-TB. 45
Acetohydroxyacid synthase is required for biosynthesis of branched-chain amino acids and converts two pyruvate molecules to acetoacetate, which is considered vital for formation of essential amino acids as important intermediaries. A single-stranded DNA as a new class of potent inhibitors of this enzyme can be a candidate for a new drug against DR-TB.46–48 The increase in matrix metalloproteinases (MMPs) in TB can cause cell recruitment, tissue destruction, cavitation, and release of matrix degradation products, which affects the severity of the disease. However, their secretion can be controlled by signaling pathways, including mitogen-activated protein (MAP) kinase, the PI3-kinase/Akt pathway, and transcription factors NF-κB and AP-1. Factors such as doxycycline, Ro32-3555, dexamethasone, and p-aminosalicylic acid can inhibit secretion of MMPs and can be considered as interesting drug targets. 49
N-acetylglucosamine-1-phosphate uridyltransferase is an essential enzyme involved in construction and assembly of the cell wall. It plays a vital role in the final stages of peptidoglycan formation by acetyltransferase and uridine transferase activity and can be a significant target for development of anti-TB drugs. 50 Shikimate kinase (SK) plays a role in aromatic amino acid formation through the SK pathway and is an essential enzyme for survival. However, the combination 5631296, a thiobarbiturate, as an inhibitor of this enzyme, shows mycobactericidal activity in synergy with rifampin. 51
In addition, isocitrate lyase, involved in fatty acid metabolism, and methionine aminopeptidase, involved in changes after protein translation, are vital mycobacterial enzymes that maintain the latency of TB infection, of which salicylanilide derivatives are important as inhibitors. 52 Salicylanilide pyrazinoate is an antimycobacterial agent with low MIC and toxicity that can inhibit Mtb-resistant strains. 53 APS reductase plays a role in biosynthesis of essential sulfur molecules for the survival and pathogenesis of bacteria. Thus, the inhibitors of this enzyme can significantly affect the level of cellular sulfurous metabolites in live mycobacteria. 54
Histone deacetylase 6 enzyme inhibits IL-10 and is inhibited by tubastatin A. It further strengthens the immune response and restricts the growth of mycobacteria. 55 Inhibition of the bacterial I-asparaginase enzyme, which plays a role in nitrogen assimilation and neutralization of acidic conditions in alveolar macrophages, can be effective against infection. 56 Mycobacterial caseinolytic protease enzymes P1 and P2 can also be controlled by bortezomib (Velcade), an effective anti-TB agent that has bactericidal properties. 57
Phosphopantetheine adenylyltransferase (CoaD) and dephospho CoA kinase (CoaE) enzymes are necessary for bacterial survival. Targeting of these enzymes can be a suitable area for development of inhibitors against this bacterium. 58 Propargyl-linked antifolates act as potent inhibitors of dihydrofolate reductase of Mtb, which penetrate into the outer membrane. 59 As can be seen, the enzymes of Mtb can be changed by various compounds and drugs. Preventing their activity affects the function and life of the bacterium and thus they are used in treatment and prevention of the disease and the prevalence of DR strains. Parts and enzymes of Mtb targeted by different compounds are shown in Fig. 1. The mechanisms of various agents targeting the components and enzymes of mycobacteria are summarized in Supplementary Table S2.
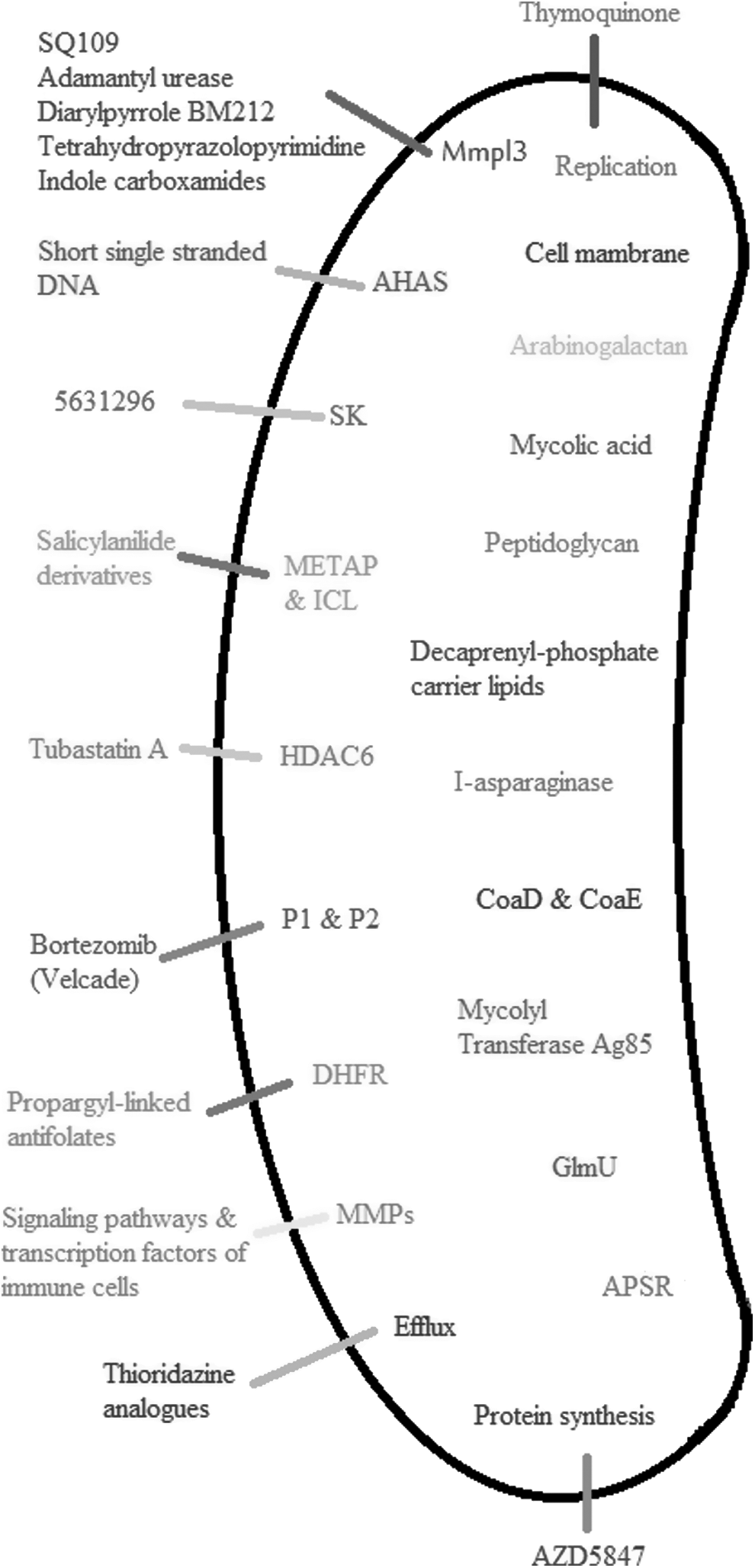
Parts and enzymes of Mtb targeted by different compounds. Interior shows the various enzymes of Mtb and processes associated with pathogen survival, each of which can be independently targeted by various compounds and drugs (exterior). The different parts of bacteria and other enzymes are attractive targets for the design of new anti-TB drugs and the increased effectiveness of existing drugs to control resistant strains. AHAS, acetohydroxyacid synthase; APSR, APS reductase; CoaD, phosphopantetheine adenylyltransferase; CoaE, dephospho CoA kinase; DHFR, dihydrofolate reductase; GlmU, N-acetylglucosamine-1-phosphate uridyltransferase; HDAC6, histone deacetylase 6; ICL, isocitrate lyase; METAP, methionine aminopeptidase, MMP, matrix metalloproteinase; MmpL3, mycobacterial membrane protein large 3; Mtb, Mycobacterium tuberculosis; P1 and P2, mycobacterial caseinolytic protease enzymes; SK, shikimate kinase.
Challenges to the Immune System and MDR-TB
The prevalence of resistant strains changes the levels of various cytokines in humoral and cellular immune systems. T cell intervention increases specific responses to Mtb, which can be useful for relapse-free treatment, especially when anti-TB drug therapy is insufficient. 60 Therefore, the association between activation of Mtb-specific T cells and a positive sputum culture and the response to treatment is very strong and would be useful in development of T cell biomarkers in the treatment of TB. 61
In general, improving cellular immune function is an important factor in the successful treatment of DR-TB. In addition, when drug therapy is combined with other treatments, it can increase the cellular immune response. For example, the response of IL-10 to the antigen of bacteria after surgery increases in the treated patients. 62 Some combinations can also enhance cellular immune responses. A Chinese extract has shown positive regulation of transcription factor levels and an increase in IFN-γ and IL-12-stimulated cell-mediated immunity. 63 In this way, the activity of CD8+ T cells in patients with DR-TB increases significantly after antigenic stimulation, 64 although the M strain can evade macrophage lysis by impairing cytotoxic T cell activity. 65
Patients with MDR-TB have the highest levels of IL-17 responses that depend on CD4+ and CD8+ T cells. This rate is related to high-level antigen loading, which indicates its immunopathological role in these patients. 66 On the other hand, the expression of Vγ2Vδ2 T cells increases resistance to TB; therefore, targeting these cells as an intervention in resistance can be considered. 67 NLRC3 from the NOD-like receptor family is a possible therapeutic target in TB through negative regulation of CD4+ T cells in the lung and spleen, preventing their differentiation and proliferation. 68
The frequency of Treg cells is high in patients with active TB and can be reduced by successful surgical treatment. 69 FoxP3+ Tregs that are stimulated by ESAT-6 and Ag85B from Mtb cause the failure of the immune response to kill bacteria. 70 Of course, the PD-1/PD-L1 signaling pathway is essential for this suppression; thus, by inhibiting this pathway, the T cell responses can be returned to the original state. 71 It is also possible to reduce the frequency of FoxP3+ cells by blocking the increased level of IL-10 in DR patients. 72
In patients with DR-TB, the frequency of B cells also changes. Some, such as IgD+CD27+ memory B cells, decrease, while the frequencies of IgD+CD38++, CD69+, and TLR9+ B cells increase. These changes can be helpful in applying the right strategies to improve the humoral immune response against Mtb. 73 The components that trigger humoral immune responses include the proteins Rv2241, Rv0009, Rv0407, and Rv2624c. 74 By examining the level of immune response and changes in various components of the immune system, TB and resistance can be identified and can be used to develop strategies for correct and effective treatment of these patients.
Vaccines
Various vaccines have been designed to protect against MDR-TB. In fact, cytotoxic T cells and effector molecules such as granulysin can be stimulated by DNA vaccines. 75 For example, a new vaccine containing HSP65+IL-12 DNA, granulysin, and Ksp37 can stimulate cytotoxic T cells and provide strong protection. 76 The combination of ID93/GLA-SE proteins against MDR-TB provides protection in animal samples and has been shown to increase BCG effectiveness in children. 77
Immunization with TNF-α-rBCG-Ag85-ESAT6 can provide a strong immune response and is a candidate for future studies. 78 The combination of WH121/DMT, consisting of five antigens such as BCG, can provide short- and long-term protection against Mtb infection in mice. The vaccine alone or with repeated vaccination offers much more prominent protection than BCG. 79 Therefore, in addition to treatment with various drugs for prevention with the aim of eradicating the disease and resistance, vaccines designed for this purpose require more serious attention.
Diagnosis
There are several methods of diagnosing DR-TB, some conventional and some novel. New ways can be quick, reliable, and more accurate than old ones such as the 2,3,5-triphenyltetrazolium chloride (TTC) assay in comparison with the traditional Nielson method. In terms of the accuracy of the test, time taken to perform it, need for a special tool to conduct it, and convenient interpretation of results, it is a cost-effective method for accurate and rapid detection of resistance to isoniazid and rifampin and can be used in laboratories with limited resources. 80 TTC is a redox indicator that produces water-insoluble, red formazan crystals when reduced by dehydrogenase in actively growing microbial cells. 81
The Xpert Mtb/RIF method is a specific and sensitive test for diagnosing pediatric pulmonary TB as well as resistance to rifampin. 82 This is a cartridge-based, fully automated, nucleic acid amplification test for detection of TB and rifampin resistance that is used in endemic countries. It purifies and amplifies by rapid, real-time polymerase chain reaction (PCR) and identifies targeted nucleic acid sequences in the TB genome. It provides results from unprocessed sputum samples in <2 hours. 83 Resazurin microtiter assay is also reliable for detection of MDR isolates in laboratories with limited resources. 84 This method uses the oxidation–reduction colorimetric indicator, resazurin, for determination of drug-resistant antimicrobial agents against Mtb. Resazurin is blue in its oxidized state and turns pink when reduced by viable cells. This technique has been described for MIC determination with Mtb clinical isolates and has been tested successfully against INH and RIF for detection of MDR-TB. 85 The CTC (5-cyano-2,3-ditolyl tetrazolium chloride) colorimetric technique is possibly the fastest way to detect PZA susceptibility in Mtb isolates. 86 This colorimetric method has been used as an indicator of the respiratory activity of mycobacteria.87,88
For identifying PZAR strains, pncA sequencing can be reliable. 89 In this case, mutation in the pncA gene encoding the pyrazinamidase enzyme is the main mechanism of resistance to PZA. 90 PCR-Restriction Fragment Length Polymorphism can also be used to detect sensitivity to ethambutol. In this case, mutations occur that lead to replacement of valine, leucine, and isoleucine amino acids in the 306 position in embB instead of methionine. 91 Position 306 in this gene is as a suitable marker for detecting resistance to TB drugs. 25
Treatment
Treatment of DR-TB requires new drugs or novel combinations for which resistance has not been detected. The combination of rifampin and carbapenem can be more effective against resistant strains because carbapenem changes the peptidoglycan layer and alters permeability to rifampin, which leads to an increase in its effective concentration in cytosol. Transcriptional suppression by rifampin does not allow cells to regulate the expression of targeted proteins by carbapenem. 92 In addition, ertapenem is well tolerated during treatment with MDR strains. Because of its fast acylation and slow deacylation, it is a poor substrate for β-lactamase, is not easily hydrolyzed by these enzymes, and will maintain activity well against bacteria.93,94
Fluoroquinolones can be effective for these isolates by shortening the treatment process in patients with resistant strains, which will reduce costs to the health system. A significant improvement and lack of recurrence have been seen with the addition of fluoroquinolones to regimens of patients with isoniazid-resistant TB.95,96 Fluoroquinolones act by inhibiting essential enzymes for the survival of bacteria, including topoisomerase II (DNA gyrase) and topoisomerase IV. 97 It has been shown under laboratory conditions that sitafloxacin has a strong activity against resistant strains. It has been shown that mutations in the gyrA and gyrB genes have less effect on this fluoroquinolone compared with others. 98
Patients with MDR-TB also can use new drugs such as bedaquiline and delamanid. 99 In patients with resistant strains, delamanid has a very low MIC and its resistance is very rare, thus it is well tolerated in the medication regimen of these patients. 100 Bedaquiline inhibits mycobacterial ATP synthase and can be a safe and effective treatment for this group.101,102 Thymoquinone, as an active anti-TB agent, can inhibit replication of the mycobacterium by inhibiting nitric oxide induced by Mtb. Its anti-inflammatory effects make it an effective drug for TB. 103 Tamoxifen, a synthetic antiestrogen, targets the bacterial membrane and shows antitubercular activity against sensitive and resistant strains as well as reduces the number of mycobacteria in macrophages in a dose-dependent manner. 104
D-LAK120-A peptide inhibits the activity of nucleic acid and proteins and causes the death of bacteria. The compound I2906 targets the isocitrate lyase, which plays an important role in maintenance of persistent infection in inflammatory macrophages. 105 These have been shown to be effective agents in combination with isoniazid (separately), which increase the efficacy of the drug in the treatment of TB under laboratory conditions and facilitate the access of isoniazid to the bacterium by increasing pathogen permeability.106,107 The 6d and 7b compounds exhibit prominent antimycobacterial activity that targets the pathway of pantothenate synthesis as an essential factor in bacterial growth and virulence and can inhibit isoniazid-resistant Mtb strains.2,108 Imidazopyridine amides 49 and 50 reduce the number of bacteria in lungs of infected mice by targeting ubiquinol cytochrome C reductase and are considered DR anti-TB agents.109–111 Bis-biguanide dihydrochloride is a potent antimycobacterial agent that inhibits bacterial replication and resistant strains and reduces pathological damage. 112
IDR-1018 is a peptide that targets bacterial biofilms and can be used as an adjuvant treatment against antibiotic-resistant infections. 113 In fact, this peptide, as well as IDR-HH2, reduces bacillary loads in animal models of DR-TB, which ultimately reduces inflammation and pneumonia. Therefore, these peptides can have roles as novel types of immunotherapies against TB. 114 In general, the use of new compounds and drugs alongside traditional drugs to prevent resistance is promising. 115 The mechanisms of various drugs targeting the mycobacterial activity and survival are listed in Supplementary Table S3.
Conclusions
The purpose of this study was to investigate various aspects of TB resistance to provide suitable solutions for prevention and treatment of TB, in particular DR-TB. As seen, mutations play an important role in development of MDR-TB and selection of these mutations can be a good way to understand the type of resistance to anti-TB drugs. In such a case, patients can be initially treated with proper and effective therapeutic choices to accelerate the course of treatment and improve patient health.
Targeting of components and the various enzymes of Mtb are both necessary for sustainability, proliferation, and actions associated with bacterial survival and can lead to finding a way to damage or destroy the pathogen so that patients recover faster and the spread of the disease, especially resistant strains, is prevented. Although significant studies have been conducted in recent decades to advance TB treatment strategies, further research is needed to increase the chance of treatment with new anti-TB drugs to stop the spread of this deadly infection and decrease the risk of a global outbreak of DR strains.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.