
Abstract
Background:
Increasing antimicrobial resistance is a major problem worldwide. Many urinary tract infection (UTI) isolates are resistant to all oral antimicrobial agents, necessitating intravenous treatment even for cystitis. Fosfomycin is a broad-spectrum antibiotic that achieves high and prolonged urinary drug concentration and is considered first-line treatment for uncomplicated cystitis. Our aim was to investigate fosfomycin susceptibility among urinary isolates and search for demographic or bacterial characteristics associated with fosfomycin nonsusceptibility.
Materials and Methods:
This is a retrospective study of all Gram-negative urinary isolates at Padeh-Poriya Medical Center in northern Israel. A total of 1503 isolates were tested for fosfomycin susceptibility, as well as susceptibility to other antimicrobial agents, by VITEK2 system and disk diffusion testing. Demographic and clinical data were obtained from patient electronic files.
Results:
A total of 1,503 isolates from patients' urine were included. Mean patient age was 64.6 years, 937 (62.3%) were female, 913 (60.7%) were Jews, and in 1,058 (70.4%) cases, the infection was community acquired; 28.1% were extended-spectrum beta lactamase (ESBL)-positive. A total of 1099 (73.1%) isolates were susceptible to fosfomycin. Fosfomycin nonsusceptibility was significantly correlated to year: 124 (20.7%) in 2015 versus 280 (30.9%) in 2016; patient age: 17.6% in patients ≤50 years versus 30% in patients >50 years; hospital-acquired UTI: 34.2% versus 23.8%; and presence of ESBL positivity: 31.1% in ESBL-positive versus 20.9% in ESBL-negative isolates (p for all <0.001).
Conclusions:
Fosfomycin nonsusceptibility among urine culture isolates is a worrisome phenomenon that is on the rise and is more often found in elderly patients, patients with nosocomial UTI, and isolates that are ESBL positive.
Introduction
Increasing antimicrobial resistance among bacteria that cause urinary tract infections (UTIs) is a major problem worldwide. Many isolates have become resistant to ampicillin, trimethoprim/sulfamethoxazole, and fluoroquinolones. In addition, alarming rates of extended-spectrum beta lactamase (ESBL)-producing bacteria have been reported from many countries.1–3 Thus, in many cases of UTIs, there is no oral treatment option, necessitating broad-spectrum intravenous antibiotic treatment with potential side effects—even for cystitis.
Fosfomycin is an antimicrobial agent used for treating UTIs and is recommended as one of the first-line treatment options for uncomplicated cystitis, prevention of recurrent cystitis, and cystitis/asymptomatic bacteriuria during pregnancy in the latest guidelines published by major national and international organizations.4–6
Fosfomycin was first discovered in Spain in 1969 from cultures of Streptomyces species. 7 It is currently available as a systemic antibiotic that has no structural relationship with other known classes of agents. Fosfomycin has a rapid bactericidal effect and a wide antibacterial spectrum, including methicillin-resistant Staphylococcus aureus, Vancomycin-resistant Enterococci, and a large number of Gram-negative pathogens.8,9 It targets bacteria by inhibiting phosphoenolpyruvate transferase, the first enzyme involved in the synthesis of peptidoglycan. 10 Major advantages of fosfomycin are the presence of an oral formulation with high bioavailability, a half-life of 2 hr, and excretion of up to 90% of the drug in unmetabolized form in the urine. 11
Resistance to fosfomycin occurs mostly by a chromosomal mutation that affects drug transport, thus decreasing uptake with ensuing low intracellular drug levels. 12 Resistance among urinary tract isolates has been reported to be <1% in previous studies, whereas more recent studies have reported resistance rates of up to 5% in Escherichia coli isolates and up to 20% in other Enterobacteriaceae.13,14
There have been no previous published studies of susceptibility rates to fosfomycin from Israel. The aim of our study was to assess susceptibility rates to fosfomycin in urinary isolates from patients with UTIs in our medical center in northern Israel and to search for demographic, clinical, or bacterial characteristics that might be associated with increased fosfomycin nonsusceptibility in an era of increased fosfomycin use.
Materials and Methods
This is a retrospective study of all 1,503 urinary isolates cultured at the microbiology laboratory of Padeh-Poriya Medical Center from January 2015 to December 2016. Demographic, clinical, and laboratory data, including patient age, gender, race, if residing at a long-term care facility, and location of infection acquisition (community acquired and nosocomial acquisition of UTI after >48 hr of hospitalization), were extracted from computerized patient medical records. Inclusion criteria were patients of all ages with a positive urine culture that was assessed for fosfomycin susceptibility. Successive urinary cultures from the same patient during the same hospitalization with an identical pathogen and susceptibility profile were not included. The study was approved by the hospital's ethics committee.
Urinary cultures were obtained from midstream urine samples or through urinary catheters in cases wherein a midstream sample could not be given. Samples were seeded either on DipStreak™ slides (Novamed, Israel) or in sterile containers. DipStreak slides use MacConkey agar as culture medium for Gram-negative organisms (only Gram-negative organisms were cultured) and CHROMagar orientation medium that enables early recognition of bacteria by colony color (blue for E. coli and pink for Klebsiella spp., etc.). Urinary samples that were collected in sterile containers were cultured on CHROMagar orientation medium (Hy-Laboratories Ltd., Israel). Urine cultures were incubated at 37°C for 24 hr. A positive urinary culture was defined according to the American Society of Microbiology guidelines. 15 Antimicrobial susceptibility testing to fosfomycin was performed for all Gram-negative isolates using the disk diffusion method by extrapolating the Clinical and Laboratory Standards Institute's 16 standards for E. coli. Susceptibility to other antibiotics was assessed using the VITEK® system (bioMérieux, SA, France). Final bacterial identification was performed using MALDI-TOF MS technology (Bruker Daltonics, Bremen, Germany).
Statistical analysis
Association between fosfomycin nonsusceptibility and demographic, clinical, and laboratory variables was assessed by chi-square test, where p-value <0.05 was considered statistically significant. Data processing was done using SAS® version 9.1.
Results
A total of 1,503 urinary Gram-negative isolates from urine cultures, 598 in 2015 and 905 in 2016, were included in the study. Mean patient age was 64.6 years (range = 17 days to 106 years), 937 (62.3%) were female, 913 (60.7%) were Jews, and 562 (37.3%) were Arabs. In 1,058 (70.4%) cases the infection was community acquired and in 445 (29.6%) the infection was nosocomial in origin.
E. coli was the most common isolate, found in 800 (53.2%) cases, followed by Klebsiella spp. in 305 (20.3%) cases, Proteus spp. in 141 (9.4%) cases, and Pseudomonas aeruginosa in 112 (7.4%) cases. Four hundred twenty (28.1%) of 1,492 isolates that were tested for ESBL were found to be positive. There was no significant change in the proportion of the various Gram-negative bacteria between the 2 years of the study.
Susceptibility to fosfomycin was found in 1,099 (73.1%) of all isolates. Fosfomycin nonsusceptibility increased significantly from 2015 to 2016: 124 isolates were nonsusceptible (20.7%) in 2015 versus 280 (30.9%) in 2016 (p < 0.005) as shown in Figure 1. Nonsusceptibility was significantly correlated with patient age: 17.6% nonsusceptibility in 66 out of 375 patients ≤50 years of age versus 30% in 338 out of 1,128 patients >50 years of age (p < 0.005). Fosfomycin nonsusceptibility was found in 167 of 566 male patients (29.5%) and 237 of 937 female patients (25.3%) (p = 0.196). Nonsusceptibility was found in 28.1% of Jewish patients and 25% of Arab patients (p = 0.44). Nonsusceptibility was significantly correlated with nosocomial acquisition of UTIs: 34.2% versus 23.8% in community-acquired cases (p < 0.005) (Fig. 2).
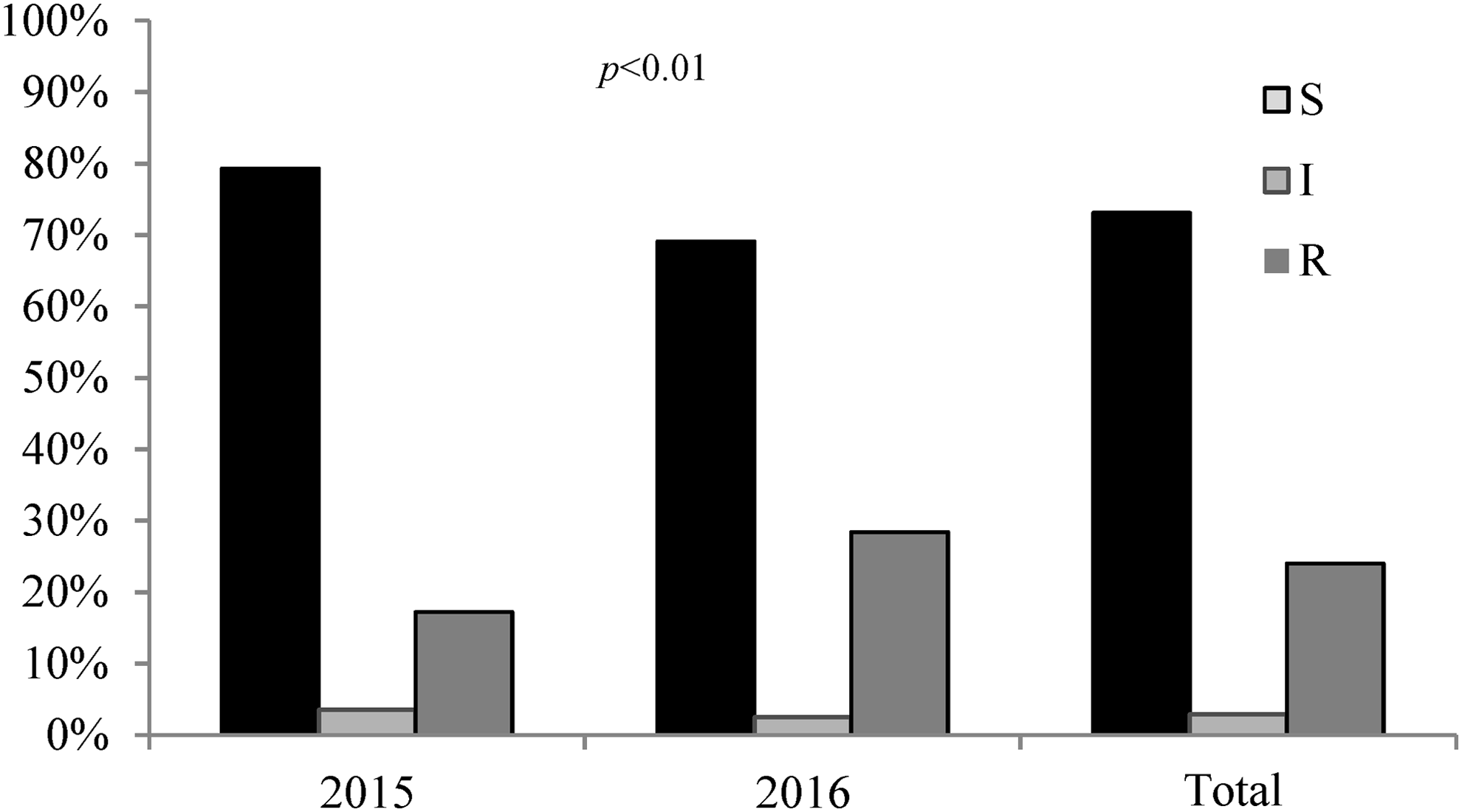
Fosfomycin susceptibility among urinary isolates in 2015 versus 2016 (n = 1,503).

Fosfomycin susceptibility among urinary isolates in community-acquired versus hospital-acquired urinary tract infections (n = 1,503).
Nonsusceptibility to fosfomycin was 5.6% in E. coli isolates, 63.1% in Klebsiella spp. isolates, 26.9% in Proteus spp. isolates, and 56.7% in P. aeruginosa isolates. Nonsusceptibility was found to be significantly associated with the presence of ESBL: 31.1% in ESBL-positive versus 20.9% in ESBL-negative isolates among 1,389 cultures that were tested for the presence of ESBL (p < 0.005) (Fig. 3).
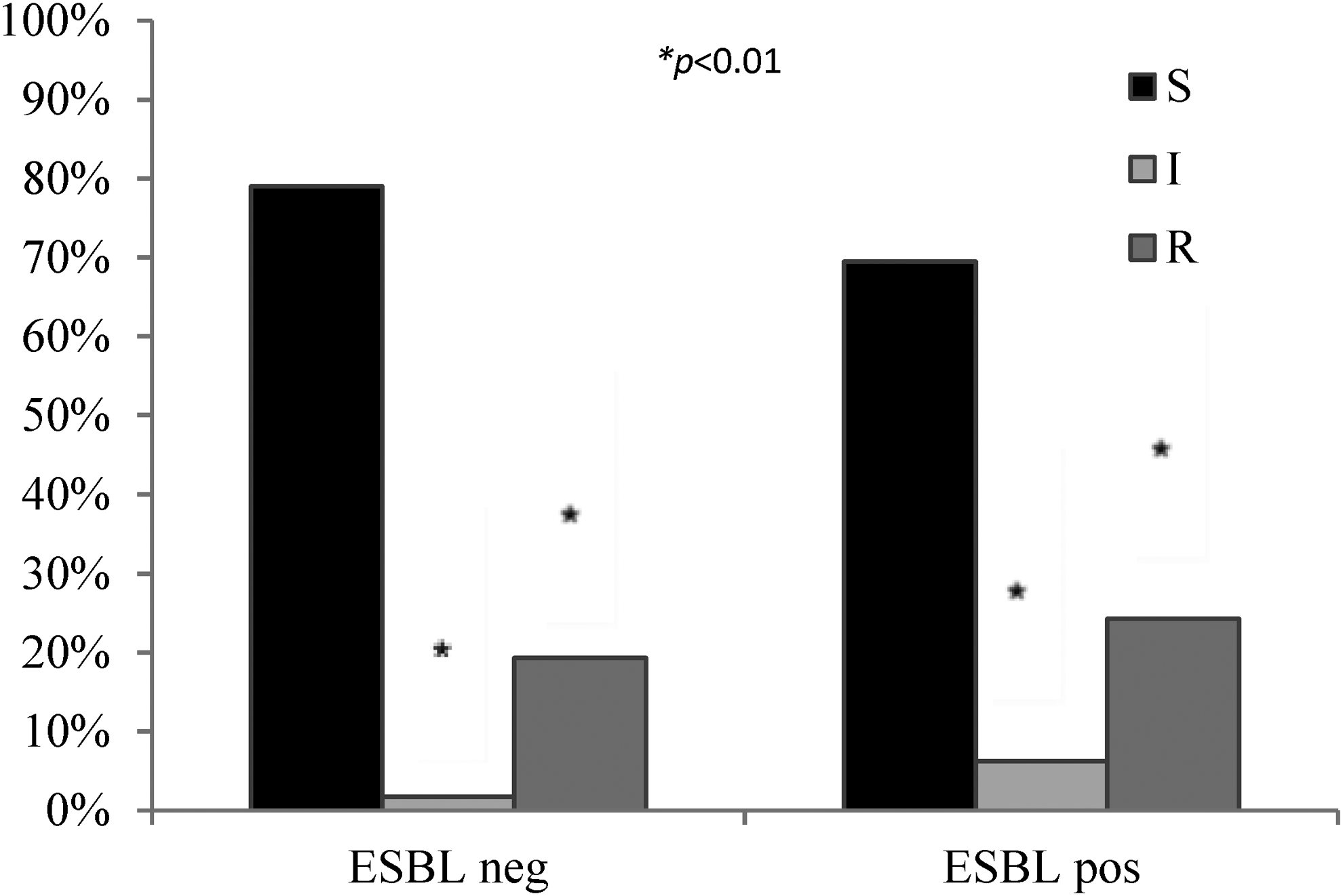
Fosfomycin susceptibility among ESBL-positive and ESBL-negative urinary isolates (n = 1,389). ESBL, extended-spectrum beta lactamase.
Susceptibility of urinary isolates to other antibiotics is depicted in Table 1. Fosfomycin nonsusceptibility was significantly associated with nonsusceptibility to ampicillin, amoxicillin–clavulanate, cefalosporines, gentamicin, nitrofurantoin, piperacillin/tazobactam, ertapenem, and trimethoprim–sulfamethoxazole (p < 0.05 for all). We did not find a significant correlation between ciprofloxacin and nonsusceptibility (p = 0.256).
Susceptibility of Urinary Isolates to Various Antibiotics
Discussion
Fosfomycin is a bactericidal antibiotic with a broad spectrum of activity against urinary tract pathogens. Both intravenous and oral formulations of fosfomycin have been in use for many years for the treatment of UTIs, but lately its use has increased due to the resistance of urinary tract pathogens to many antimicrobials, with fewer treatment options. We aimed to assess whether this might lead to increased resistance to fosfomycin.
In this study, we found a susceptibility rate of 77% in 1,503 Gram-negative urinary isolates (and 94.4% among E. Coli isolates) collected from patients during 2015–2016 at our medical center. This rate is somewhat lower than previously reported from various studies around the world, including studies published during the past few years. A study from India has found 100% susceptibility to fosfomycin in 564 E. Coli isolates from patients' urine cultures during January–March 2016. 17 A study from the United States has reported 99.6% fosfomycin susceptibility in E. coli isolates. 18 A study from the Czech Republic that examined 3,295 urine cultures during 2013–2014 has found fosfomycin susceptibility in 97% of E. coli isolates and 80.4% of Klebsiella isolates. 19
It is possible that the high resistance rate found in our study may be due to the fact that all cultures obtained at our medical center were from patients who were hospitalized with suspected UTIs (or UTI acquired during hospitalization) and not from outpatients, thus indicating a population of patients with a more complicated or severe UTI who might have received prior antibiotic courses for their infection as well. We found a significant increase in fosfomycin nonsusceptibility from 124 isolates (20.7%) in 2015 to 280 (30.9%) isolates in 2016. These data are worrisome and might reflect the fact that because resistance to other antibiotics used in the treatment of UTIs is on the rise, and because recent guidelines advocate the use of fosfomycin as first-line treatment of lower UTIs, the use of fosfomycin is increasing in both outpatient and inpatient settings, with a possible ensuing increase in resistance. Fosfomycin might represent the last-resort drug for extensively drug-resistant (XDR) bacteria, and thus our findings are a cause of great concern. A recent study from Great Britain has found an increase in fosfomycin use from 2013 to 2015 for patients with multiresistant urinary pathogens. 5
Fosfomycin nonsusceptibility was found to be significantly higher in patients >50 years of age. Older age is a risk factor for infection with resistant bacteria, such as Methycillin-resistant Staphylococcus aureus (MRSA)- or ESBL-producing Enterobacteriaceae, mostly due to increased prevalence of chronic diseases and exposure to antibiotics and health care facilities. 20 Indeed, in our study we found that fosfomycin nonsusceptibility was significantly higher in cases of nosocomial UTI than in community-acquired infections. This is not a surprising finding, as a nosocomial source of infection is known to be linked to multidrug-resistant pathogens. In this study, a significant difference in nonsusceptibility to fosfomycin was found between E. coli (6%) and other Gram-negative uropathogens (Klebsiella spp. 63%, Proteus spp. 27%, and P. aeruginosa 57%). Other studies have also demonstrated lower susceptibility rates among non-E. coli isolates, 17 with a study from three Veterans Affairs facilities in Massachusetts demonstrating 97% susceptibility among E. coli versus 64% in Klebsiella spp. 21
In our study, urine cultures with ESBL-producing bacteria had a higher rate of fosfomycin nonsusceptibility than urine cultures with non-ESBL-producing bacteria, reaching 30.5%. ESBL-producing bacteria frequently acquire additional resistance mechanisms, so that they are more resistant to other antimicrobial agents such as fluoroquinolones. A US study has found that among 204 patients with UTIs caused by ESBL-producing Enterobacteriaceae, fosfomycin resistance rate was 19.9%. 21 Another study from the United States involving 91 multidrug-resistant urinary isolates has found 5% resistance to fosfomycin, with only 1% resistance among ESBL-producing bacteria. 22
The weaknesses of this study include the fact that it assessed isolates from a single hospital in northern Israel and thus may not constitute a representative sample of Israel as a whole. Even though CLSI guidelines state that the disk diffusion method is only approved for assessing E. coli susceptibility to fosfomycin, we extrapolated the standard for other Gram-negative bacteria as well. Another weakness of this study is that only Gram-negative bacteria were assessed, so the study lacks information regarding fosfomycin susceptibility among Gram-positive urinary pathogens. We did not assess prior antibiotic exposure as a factor that might influence fosfomycin nonsusceptibility. In addition, only samples from those hospitalized due to suspicion of UTIs were studied, and so it is possible that patients with UTIs treated as outpatients may harbor fewer resistant strains. In addition, a multivariable analysis was not conducted, as some of the factors associated with fosfomycin resistance may be dependent on each other.
The strength of this work is that it includes a large number of isolates and that it is the first published work assessing fosfomycin nonsusceptibility in Israel.
Our finding of high nonsusceptibility rates to fosfomycin is very worrisome and points to the importance of ongoing monitoring of resistance rates to this agent, and the possibly for the need of curtailing its use.
Ethics Approval
The study was approved by the hospital's ethics committee.
Footnotes
Disclosure Statement
No competing financial interests exist.