
Abstract
Carbapenem-resistant Klebsiella pneumoniae (CRKP) strains pose a significant threat to public health. In this study, a survey was conducted in the Jiangxi Province of China, covering a total of 140 CRKP strains collected from 11 hospital laboratories from June 2016 to January 2018. All CRKP isolates were subjected to antimicrobial susceptibility testing, capsular serotypes, virulence gene profiles, multilocus sequence typing, and pulsed-field gel electrophoresis. The differences in the patient characteristics and distributions among the various regions were statistically significant (p ≤ 0.001). Most patients were hospitalized in intensive care units (30.0%) and burn departments (13.6%), with lower respiratory (52.1%) and urinary tract (15.7%) infections being most prevalent. A higher ratio of CRKP isolates were identified in the southern and central regions of Jiangxi than in the other regions. Only two carbapenemase genes, blaKPC and blaNDM, were responsible for phenotypic resistance in the tested CRKP strains (46.5% and 22.1%, respectively), among which several major sequence types (STs), such as ST11 (27.8%) and ST23 (14.8%), were identified. A total of 39 virulent strains were detected, of which 22 strains were classified by capsule serotyping. Hypervirulent genes were most common in the eastern and central regions of Jiangxi. In conclusion, CRKP strains in the Jiangxi Province have varied geographic distributions; the resistance rates of isolates harboring blaKPC decreased from southern to northern regions, whereas the drug resistance gene blaNDM showed a tendency to spread from a central point to the surrounding areas. ST23 carbapenem-resistant hypervirulent K. pneumoniae is emerging, resulting in an urgent need to enhance clinical awareness.
Introduction
Carbapenem-
Unfortunately, virulence and resistance could converge to produce strains that are able to cause severe and untreatable invasive infections, representing a major public health concern. 2 The Lancet Infectious Diseases journal reported a fatal outbreak of ventilator-associated pneumonia that was caused by an emerging carbapenem-resistant hypervirulent K. pneumoniae (hvKP) strain, which is a subtype of the prevalent sequence type (ST) 11 type of CRKP. 3 This hypervirulent strain causes not only hospital-acquired infections in immunocompromised patients but also community-acquired infections in healthy individuals.
The prevalence of CRKP is diverse across countries and regions and has been responsible for major hospital outbreaks that have led to a reduction in therapeutic options, resulting in high morbidity and mortality and increasing hospital lengths of stay and associated costs. 4 In China, the prevalence of CRKP shows geographic differences. Local surveillance data on antimicrobial resistance and the identification of risk factors for colonization and infection are critical. 5 In this study, we conducted province-wide surveillance of CRKP in the Jiangxi Province and investigated the prevalence and molecular epidemiologic features of the identified strains, with the hope of identifying the key strains and mobile resistance elements responsible for the increased prevalence. The results from this study will provide essential insight into effective strategy developments for the global control of CRKP to reduce untreatable infection rates in clinical settings.
Materials and Methods
CRKP isolates
Nonduplicate carbapenem-nonsusceptible K. pneumoniae isolates were collected from hospitals in 11 prefecture-level cities in Jiangxi Province (Supplementary Appendix S1), including Nanchang, Jingdezhen, Jiujiang, Pingxiang, Ganzhou, Xinyu, Yingtan, Ji'an, Yichun, Fuzhou, and Shangrao, from June 2016 to January 2018. One representative hospital from each location (usually the largest general hospital in the location) was chosen for sample collection. According to the geographical distribution, we divided the locations into four areas: east, west, south, and north. We separately analyzed the data from Nanchang, as a provincial capital city.
CRKP definition and antimicrobial susceptibility testing
CRKP was defined according to the recommendation of the Clinical and Laboratory Standards Institute (CLSI), 6 as K. pneumoniae strains resistant to at least one carbapenem agent such as imipenem, ertapenem, or meropenem. Isolate identification and antibiotic susceptibility testing were carried out using an automated Vitek-2 system (bioMérieux, Marcy l'Étoile, France). In this study, the minimum inhibitory concentration results were interpreted according to the breakpoints defined by the CLSI, 6 with the exception of tigecycline and colistin, which were defined by criteria set forth by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) 7 because of a lack of validated CLSI-established breakpoints.
Clinical and epidemiologic information
The medical records of each patient were reviewed. Clinical data, including demographic information, medical history, comorbidities, treatments, and outcome at discharge, were collected. Infections were classified as either community- or health care-associated according to standard epidemiologic definitions established by the U.S. CDC. 8
Screening of carbapenemase resistance genes
Polymerase chain reaction (PCR) and nucleotide sequencing were performed to screen for the presence of the carbapenemase-encoding genes blaVIM, blaIMP, blaKPC, blaOXA-48, blaIMI, blaGES, and blaNDM, as described previously. 9 The phenotypes were evaluated using a modified carbapenem inactivation method (mCIM). 10
Detection of K. pneumoniae virulence genes
We identified the capsular antigen genes encoding for K1, K2, K5, K20, K54, and K57 antigens, and amplified the magA (mucosal phenotypic associated gene A) and rmpA (regulator of mucosal phenotypic gene A) genes simultaneously using PCR as described previously. 11
Molecular genotyping of isolates
Pulsed-field gel electrophoresis
Pulsed-field gel electrophoresis (PFGE), as a predominant strain typing method used to confirm the genetic relatedness of isolates, was performed as described by Pfaller and colleagues. 12 Whole chromosomal DNA was digested with XbaI (Bio-Rad Laboratories), and the restriction fragments were separated in a CHEF Mapper XA System (Bio-Rad Laboratories). A cluster analysis was performed with the Dice similarity coefficient and unweighted pair group matching algorithm, with a tolerance of 1.0% and 1.0% optimization using the BioNumerics version 7.0 program. The Salmonella strain H9812 was used as the control strain. Dendrograms depicting the genetic relatedness of the test strains were generated from the homology matrix to describe the relationships of the PFGE profiles of the test strains.
Multilocus sequence typing
Multilocus sequence typing (MLST) was performed on all CRKP isolates by amplifying the seven standard housekeeping loci, including gapA, infB, mdh, pgi, phoE, rpoB, and tonB, as previously described. 13 STs were assigned using the online Pasteur Institute MLST website*, database. 14 A minimum spanning tree was created using the BioNumerics version 7.0 program.
Statistical analyses
Chi-square tests, Fisher's exact tests, or Kruskal–Wallis tests were used to explore the association between the clinical and epidemiologic characteristics of the infected patients and strain genotypes. The level of statistical significance was defined as a p value of ≤0.05. All statistical analyses were performed using SPSS v.22 software.
Results of the Survey
CRKP strains and antibiotic susceptibility
A total of 140 nonduplicated CRKP strains collected from hospitals in 11 prefecture-level cities in the Jiangxi Province were studied to identify the molecular epidemiologic features of these organisms. The isolates originated from different anatomic sites, including sputum (n = 80, 57.1%), urine (n = 22, 15.7%), bodily secretions (n = 15, 10.7%), blood (n = 15, 10.7%), bile (n = 2, 1.4%), throat swabs (n = 2, 1.4%), cerebrospinal fluid (n = 2, 1.4%), and pus (n = 2, 1.4%). The antimicrobial resistance rates of the 140 CRKP isolates are shown in Table 1. All 140 CRKP isolates were resistant to ampicillin, cefazolin, and imipenem; in addition, some isolates were resistant to meropenem (98.6%), cefotetan (98.2%), and aztreonam (97.2%). The antimicrobial agents with susceptibility of <60% included amikacin (59.1%) and ertapenem (33.3%).
Antimicrobial Resistance Profiles in 140 Carbapenem-Resistant Klebsiella pneumoniae Isolates
AK, amikacin; AMP, ampicillin; ATM, aztreonam; CAZ, ceftazidime; CFZ, cefazolin; CIP, ciprofloxacin; CRO, ceftriaxone; CTT, cefotetan; ETP, ertapenem; FEP, cefepime; IMP, imipenem; LVX, levofloxacin; MEM, meropenem; MIC, minimum inhibitory concentration; SAM, ampicillin/sulbactam; TGC, tigecycline; TZP, piperacillin/tazobactam.
General clinical characteristics
In total, 140 patients infected with CRKP were enrolled. The demographic and clinical characteristics of patients are summarized in Table 2. The majority of patients were males (75.0%), with ages ranging from 4 to 88 years, but this ratio was lower in the central district (47.5%). CRKP isolates were obtained from patients admitted to intensive care units (ICUs; n = 42, 30.0%), burn units (n = 19, 13.6%), neurosurgery wards (n = 15, 10.7%), respiratory medicine wards (n = 15, 10.7%), pediatric wards (n = 12, 8.6%), urinary surgery wards (n = 11, 7.9%), orthopedics and traumatology wards (n = 10, 7.1%), geriatric wards (n = 2, 1.4%), and other wards (n = 14, 10.0%). In southern Jiangxi, the patients were mainly from burn units, while those in other regions were primarily concentrated in ICUs. The differences in the patients' characteristics and distributions in the various regions of Jiangxi Province were statistically significant (p ≤ 0.001). The most prevalent infections were in the lower respiratory (n = 73, 52.1%) and urinary tracts (n = 22, 15.7%). There were also significant differences regarding the site of infection and the various regions (p ≤ 0.001), with lower respiratory tract infections being dominant in central, eastern, and western Jiangxi and skin and soft tissue infections being dominant in the southern region. Surgical treatments were performed in 40.7% (n = 57) of the patients. In addition, invasive medical devices, including urinary (n = 86, 61.4%) and central venous catheters (n = 75, 53.6%) and invasive mechanical ventilators (n = 48, 34.3%), were commonly used at the time of infection. The rate of infections in patient with central venous catheters in the western region was only 28.0%, while that in the other regions was more than 50.0%. Among these patients, 15.7% (n = 22) presented clinical improvement at discharge, and 2.9% died (n = 4).
Patients' Demographic and Clinical Characteristics
The variable was statistically different (a p value of ≤0.001) when compared among the northern, eastern, southern, western, and central Jiangxi provinces using the chi-square, Fisher's exact, or Kruskal–Wallis tests.
The variable was statistically different (a p value of ≤0.05) when compared among the northern, eastern, southern, western, and central Jiangxi provinces using the chi-square, Fisher's exact, or Kruskal–Wallis tests.
N, no one.
Distribution of antimicrobial resistance genes
Among the 140 CRKP isolates, only 2 carbapenemase genes, blaKPC (n = 65, 46.4%) and blaNDM (n = 31, 22.1%), were detected. The carbapenem-resistant isolates were found to be carbapenemase producers according to the mCIM. In accordance with the phenotypic results, 65 CRKP isolates were positive for blaKPC, and 31 CRKP isolates were positive for blaNDM. Antimicrobial resistance was serious in the southern and central Jiangxi regions. The resistance rates of isolates with blaKPC were 40.0%, 80.0%, 30.0%, 0.0%, and 67.5% in eastern, southern, western, northern, and central Jiangxi, respectively. The resistance rates of isolates with blaNDM were 30.0%, 0.0%, 21.0%, 12.5%, and 37.5% in eastern, southern, western, northern, and central Jiangxi, respectively. Only blaKPC was detected in the southern regions, and the resistance rates of isolates with blaKPC decreased from the southern to northern regions. The blaNDM drug resistance gene showed a tendency to spread from a central point to the surrounding areas; only blaNDM was detected in the northern regions (Fig. 1).

Carbapenem resistance rate and relative prevalence of various carbapenemase-producing elements among clinical CRKP strains recovered from different cities in the Jiangxi province. Different background colors represent different carbapenem resistance prevalence rates. Circle partitions represent the prevalence of different carbapenemases produced by CRKP strains at different locations. CRKP, carbapenem-resistant Klebsiella pneumoniae. Color images are available online.
Distribution of serotypes and virulence genes
A total of 39 virulent strains were detected, of which 22 strains were classified by capsule serotype, including 6 strains of K1, 8 strains of K2, 5 strains of K5, 3 strains of K57, and no strains of K20 or K54. Among the virulence genes, 19 and 7 strains presented rmpA and magA, respectively. These two virulence genes were simultaneously detected in five strains. From the virulence gene distributions, we found that K1 and K2 were most common in eastern Jiangxi, K57 was detected only in the Nanchang area, and rmpA had the highest detection rate in southern Jiangxi (Table 3 and Fig. 2).

Virulence rate and relative prevalence of various virulence elements among clinical CRKP strains recovered from a different city of Jiangxi province. Different background colors represent different prevalence of virulence rate. Circle partitions represent the prevalence of different virulence genes harbored by CRKP strains at different locations. Color images are available online.
Distribution of Serotypes and Virulence Genes in the Highly Virulent Capsule of Klebsiella pneumoniae
magA, mucosal phenotypic associated gene A; rmpA, regulator of mucosal phenotypic gene A.
Distribution of sequence and PFGE types
The clonal relatedness of all of the CRKP isolates was determined using PFGE and MLST, as shown in Figs. 3 and 4. Among the 140 CRKP isolates that harbored carbapenemase genes, 33 PFGE patterns and 15 STs were identified. Unlike other regions of the world, where K. pneumoniae ST258 is the major strain that produces carbapenemases, ST11 is the most dominant strain in China.15,16 ST11 accounted for 27.8% of the isolates, followed by ST23 (14.8%), ST1886 (11.1%), ST345 (7.4%), ST309 (7.4%), ST35 (5.6%), ST8 (3.7%), ST25 (3.7%), ST1884 (3.7%), and the single isolates ST20, -65, -152, -592, and -2464. The ST11 type was prevalent in eastern Jiangxi and the Nanchang district. We noted that ST23 was the predominant type in southern Jiangxi, as 10 of the 25 identified CRKP isolates belonged to this strain. All ST23 strains were identified as the same clone, as they exhibited identical PFGE patterns, suggesting that clonal dissemination is common in certain regions. Most of the ST types of K. pneumoniae, including ST11 (18/31) and ST1886 (8/10), mainly harbored blaKPC, whereas ST23 (7/11) mainly harbored blaKPC. Moreover, K. pneumoniae ST11 and ST1886 were found to harbor both blaNDM and blaKPC in central Jiangxi.
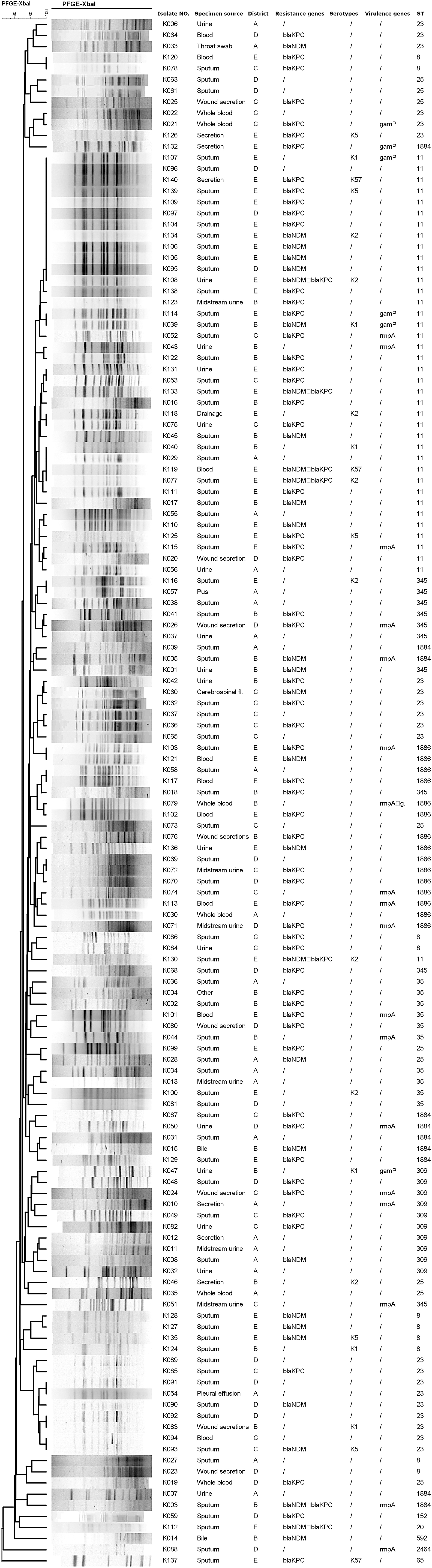
PFGE dendrogram showing the genetic relationship between representative CRKP strains. The PFGE dendrogram was generated with BioNumerics software. The band analysis was created using the Dice similarity coefficient and the unweighted pair group method with arithmetic averages. The dashed line corresponds to 80% as the cutoff for close genetic relationships (A is for northern Jiangxi, B is for eastern Jiangxi, C is for southern Jiangxi, D is for western Jiangxi, and E for central Jiangxi). PFGE, pulsed-field gel electrophoresis. Text can be magnified for improved readability.

Minimal spanning Klebsiella pneumoniae Tree based on multilocus sequence typing. Different colored circles indicate different sequence genotypes. The size of the circle is proportional to the number of strains, the solid black line between the connecting circles indicates the difference in the presence of a housekeeper gene for the two sequence genotypes, the gray line indicates the difference in two housekeeper genes, and the dashed lines indicate the differences in three or more alleles. Color images are available online.
Discussion
Infections caused by CRKP strains are a pressing issue for public health. Several studies have certified that CRKP, which is one of the most critical nosocomial pathogens, could increase mortality rates, especially in patients with severe diseases. 17 Although several attempts have been made to control the spread of these infections at local and national levels, the rapid dissemination of CRKP still poses an urgent global threat. 18 Local epidemiologic data on the prevalence of specific clones of CRKP are indispensable for developing clinical treatment regimens and evaluating the outcomes of different therapeutic strategies. 19
In this study, most of the patients were hospitalized in ICUs and burn departments. ICUs are the principal hospital reservoirs of MDR bacteria, and a recent stay in the ICU markedly increases the probability of K. pneumoniae isolation in patients. Previous studies showed that long-term catheter use, frequent antibiotic use, and weakened immune systems were the leading causes of nosocomial infections. 20 Assorted invasive procedures and medical histories, including previous hospital admissions, were strongly correlated with CRKP infections.21,22 There were significant differences regarding the sites of infection among the various regions, with lower respiratory tract infections being dominant in central, eastern, and western Jiangxi, and skin and soft tissue infections being dominant in the southern region. In contrast to developed countries, antibiotic overuse or misuse is still universal in Jiangxi Province, particularly in rural areas in the southern region. People living in impoverished regions have a stronger need for antimicrobial therapy, and poverty can prompt short treatment courses or the use of low-quality drugs. Furthermore, due to the large population in central Jiangxi, the prevention and control of multidrug-resistant hospital infections need to be strengthened through the implementation of multimodal infection prevention and control strategies and hand hygiene compliance for the control of CRKP.
With increasing antibiotic resistance, CRKP drug resistance and virulence genes have become the foci of health concerns in clinical settings. Many studies have shown that Klebsiella pneumoniae carbapenemase (KPC)-producing bacteria are widespread in China, Israel, Greece, South America, and the United States,23,24 and that the CRKP capsular polysaccharide is a crucial pathogenic virulence factor that results in strong resistance to neutrophil phagocytosis and the bactericidal effects of complement in serum. The acquisition of drug resistance genes in Staphylococcus aureus is often accompanied by the loss of virulence genes and other pathogenic factors. 25 Therefore, methicillin-sensitive S. aureus usually harbors more virulence-related genes than drug-resistant strains. In CRKP, resistance genes are similar to virulence genes. Although the hypervirulent and antimicrobial-resistant populations of K. pneumoniae were largely nonoverlapping, some isolates with combined virulence and resistance were detected.26,27 More importantly, hypervirulent CRKP isolates have emerged in clinical settings.3,15 At present, 78 different capsule serotypes have been reported, among which K1, K2, K5, K20, K54, and K57 are hypervirulent K. pneumonia strains that are closely associated with various invasive infections in humans and animals.28,29 We investigated the capsular serotypes of the four CRKP strains (K1, K2, K5, and K57) isolated in the Jiangxi area. Almost all of the CRKP-associated infections were severe and manifested as septicemia, liver abscesses, and extrahepatic infections, which are associated with the K1 and K2 capsular serotype strains. 30 We found that magA is not a specific CRKP virulence gene but is closely related to the K1 capsular serotype, while rmpA, the positive regulator of gmaP, is associated with the mucoid phenotype of the K2 capsular CRKP serotype. Furthermore, we found that the detection rate of the K1 and K2 capsular serotypes in the Jiangxi area was 10%, which was lower than the detection rate of the capsular CRKP serotypes reported in other domestic studies.
Multiple CRKP strains have been detected in China, and several unique strains are responsible for the increasing number of CRKP infections in China. MLST studies showed that CRKP clones were widespread. Considering our current research on novel CRKP epidemiologic data in China, we emphasize the need to actively monitor CRKP dissemination. ST258 is a frequently reported CRKP strain worldwide, 31 but ST11, which has exhibited signs of multiclonal dissemination, is the dominant CRKP type in Jiangxi Province. Other strains are relatively rare and sporadic in their distributions, with ST23 being the next most common strain. There is a different trend of carbapenemase-producing STs in Jiangxi Province. Some previous studies showed that most of the K. pneumoniae STs, including ST11, harbored blaKPC, whereas K. pneumoniae ST23 mainly harbored blaNDM.5,32 However, in this study, most of the STs of K. pneumoniae, including ST11 and ST1886, were found to mainly harbor blaKPC, whereas ST23 mainly carried blaKPC. We noted that ST23 was the predominant strain in southern Jiangxi, as 10 of the 25 tested CRKP isolates belonged to this strain. All ST23 strains were identified as the same clone, as they exhibited identical PFGE patterns, suggesting that clonal dissemination is common in certain regions. Further research is needed to understand the adaptability of different plasmids that encode carbapenemases in different CRKP strains. Therefore, attention should be focused on the identification of sporadic STs and surveillance of the most prevalent clonal complexes.
We reported the first province-wide CRKP surveillance study in Jiangxi. We found that the CRKP strains in Jiangxi Province were transmitted by CRKP polyclones with high drug resistance and high virulence elements. The resistance rate of isolates harboring blaKPC decreased from south to north, whereas the drug resistance gene blaNDM tended to disseminate from a central point to the surrounding areas. The hospital in Nanchang, the provincial capital city (Supplementary Appendix S1), is responsible for the treatment of critically ill patients from all over the province, which could be the reason why the drug resistance rates in the Nanchang area have reached serious levels. ST11 has been the dominant CRKP strain, but ST23 carbapenem-resistant hypervirulent K. pneumoniae is emerging. According to the results of this study, we propose that nosocomial CRKP infection control strategies should be reevaluated and adjusted. Although the economy in Jiangxi Province is underdeveloped, CRKP treatment must be considered urgent. Therefore, the establishment of increased and improved bacterial surveillance in hospitals is crucially needed to prevent the further spread of resistant bacteria.
Footnotes
Acknowledgments
We are grateful for the medical and research personnel who assisted in the collection of CRKP strains: Bin Zhou (The Third Affiliated Hospital of Nanchang University), Manli Liu (Jiujiang First People's Hospital), Yi Liu (Jingdezhen First People's Hospital), Bin Zhu (Shangrao City People's Hospital), Jitao Xu (Yingtan City People's Hospital), Ruoping Jiao (Fuzhou First People Hospital), Qiunv Feng (Ganzhou City People's Hospital), Lixin Luo (Ji'an City Centre People's Hospital), Rongping Huang (Xinyu City People's Hospital), Jian Yang (Pingxiang City People's Hospital), and Wenzhi Huang (Yichun City People's Hospital).
Authors' Contributions
X.C. contributed to the study design, data interpretation, and review of the manuscript. L.Z. and Q.D. contributed to the drafting of the manuscript. L.Z., T.Z., and J.Z. contributed to the data acquisition, experiments, and analysis. Y.L. contributed to the supervision of the investigation. All the authors were involved in writing, critically revising for intellectual content, and approving the final version of the manuscript submitted for publication.
Disclosure Statement
All authors report no conflicts of interest relevant to this article.
Funding Information
This study was funded by grants from the Jiangxi Science and Technology Agency Funding Project of China (Grant No. 20152ACG70015).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.