
Abstract
Aims:
Acinetobacter baumannii has become an important nosocomial pathogen that causes invasive infections. We conducted a retrospective study to evaluate the risk factors for mortality due to A. baumannii bacteremia in children.
Materials and Methods:
We reviewed data from Seoul National University Children's Hospital from 2002 to 2013 for children with A. baumannii bacteremia, including age, gender, underlying disease, associated site of infection, duration of hospitalization, presence of neutropenia, and antibiotic susceptibility data. The outcome measures were the 7- and 30-day mortality rates.
Results:
Among 74 A. baumannii bacteremia cases, 35.1% were carbapenem nonsusceptible. Common comorbidities were malignancy or hematologic diseases (28.4%), followed by gastrointestinal/hepatobiliary diseases (21.6%). A total of 47.3% of patients had isolated bacteremia, and in 33.8% of patients, pneumonia accompanied bacteremia. The mortality rates were 18.9% at 7 days and 35.1% at 30 days. The significant associated factors for 30-day mortality were carbapenem nonsusceptibility (adjusted hazard ratio [aHR]: 1.28, 95% confidence interval [CI]: 1.10–11.82, p = 0.034), neutropenia (aHR: 1.68, 95% CI: 1.60–18.03, p = 0.007), and prior intensive care unit (ICU) admission (aHR: 1.15, 95% CI: 1.03–9.73, p = 0.045). The mortality rate among neutropenic patients with inappropriate empirical antibiotics was higher than that among patients with appropriate empirical antibiotics (90.1% vs. 33.3%, p = 0.031).
Conclusions:
We identified carbapenem nonsusceptibility, neutropenia, and prolonged ICU stay as independent risk factors for mortality due to A. baumannii bacteremia in children. An early administration of appropriate antibiotics should be enacted, especially in patients with neutropenia.
Introduction
Acinetobacter baumannii has become an important nosocomial pathogen that causes bacteremia among immunocompromised patients. 1 Previously, A. baumannii was considered to have less clinical significance. However, it has emerged as an invasive and life-threatening pathogen, largely demonstrated in the adult population, that results in significant mortality. 2 A time trend change has been observed in large tertiary care hospitals in South Korea during the past decades, with an increasing incidence of A. baumannii and its carbapenem resistance. 3
A. baumannii bacteremia in the pediatric population has been previously described in specific populations in neonatal intensive care units (ICUs) and pediatric ICUs; however, the general risk factors for mortality in the broader childhood population are limited.4,5 Additional data are needed to guide decisions on the management of A. baumannii bacteremia in children. The purpose of the present study was to evaluate the risk factors for mortality in children with A. baumannii bacteremia.
Materials and Methods
Study setting and data source
Seoul National University Children's Hospital is a 350-bed tertiary care hospital and referral center located in Seoul, Republic of Korea. We analyzed data collected by the Clinical Microbiology Laboratory from January 2002 to July 2013 to identify pediatric patients with A. baumannii bacteremia. All patients aged <18 years with A. baumannii isolated from blood cultures were included. We reviewed the medical records of individuals and identified patients with clinically significant A. baumannii bacteremia. Species identification was conducted with Vitek-2 system (bioMérieux, Hazelwood). Antibiotic susceptibility testing followed the recommendations of the Clinical and Laboratory Standards Institute (CLSI). 6 Given that certain members of the A. baumannii complex may not be identified at the species level from our system, the data represent isolates belonging to the A. baumannii complex.
Definition
A. baumannii bacteremia was defined as an isolation of A. baumannii in a blood culture specimen in patients with clinical features compatible with systemic inflammatory response syndrome. A nonsusceptible breakpoint for carbapenem (imipenem and meropenem) was defined as an MIC >8 μg/mL, in accordance with the CLSI guidelines. 6 Patients were categorized according to the associated site of infection as follows: “isolated bacteremia,” for patients with no identifiable source of infection; “pneumonia,” for patients with respiratory symptoms and radiographic evidence of infiltrates consistent with pneumonia; and “catheter-related,” for patients with A. baumannii isolated from central intravascular catheter. The empirical antibiotic therapies were classified as either appropriate or inappropriate, with the former defined as a treatment regimen that included one or more antibiotics active in vitro against the isolated strain, and the latter defined as a treatment regimen with antibiotics that did not have in vitro activity against the isolated strain. Neutropenia was defined as an absolute neutrophil count of <1,000 neutrophils/mm3, and the postoperative state was defined as a history of operation within 30 days before the onset of bacteremia.
Study design and data analysis
We assessed the risk factors for mortality due to bacteremia caused by A. baumannii in children through a retrospective review of medical records. We collected data for age, gender, underlying disease, associated site of infection, and duration of hospitalization and ICU treatment before the onset of bacteremia. We also reviewed the empirical antibiotic regimen, carbapenem nonsusceptibility, history of receiving surgery, and the presence of neutropenia.
The crude outcome measures were the need for inotropes, the need for mechanical ventilation, persistent bacteremia after 48 hours, and the 7- and 30-day mortality rates. The chi-square test was used to compare categorical variables, and the Kaplan–Meier method was used for survival analysis. To identify the independent risk factors for 30-day mortality, a stepwise backward multivariable logistic regression analysis model was used. Hazard ratios (HRs) and their 95% confidence intervals (CIs) were calculated. All p-values were two-tailed, and p-values <0.05 were considered statistically significant. For analyses, we used R Studio version 1.1.423 with “survival” and “survminer” packages (R Studio, Boston, MA).
This study was approved by the Seoul National University Hospital Institutional Ethics Board (IRB No. 1311-041-532).
Results
Study population
In total, 74 consecutive pediatric patients with A. baumannii bacteremia were identified among 1,644 isolates (Figs. 1 and 2). Supplementary Figure S1 depicts the trend of Acinetobacter isolates over time. Of these, 39.2% (n = 29/74) were infants aged less than 12 months (Table 1). A total of 35.1% (n = 26/74) patients had carbapenem-nonsusceptible isolates; 28.4% (n = 21/74) patients had malignancy or hematologic diseases; 21.6% (n = 16/74) patients had gastrointestinal or hepatobiliary diseases; 14.9% (n = 11/74) patients had cardiovascular diseases; 12.2% (n = 9/74) patients had neurologic or neuromuscular diseases; and 12.2% (n = 9/74) patients were premature infants. A total of 47.3% (n = 35/74) patients had isolated bacteremia; 33.8% (n = 25/74) patients had pneumonia; and 16.2% (n = 12/74) patients had catheter-related A. baumannii bacteremia. The median time of total hospital stay before the onset of bacteremia was 25.5 days (range: 1–950 days), and the median time of ICU stay before onset of bacteremia was 7.0 days (range: 0–204 days). In total, 33.8% (n = 25/74) and 31.3% (n = 23/74) patients required inotropic support or intubation with mechanical ventilation. A total of 23.0% (n = 17/74) patients had persistent bacteremia after 48 hours. The median time from the onset of A. baumannii bacteremia-related death was 3 days (range: 1–30 days); the 7-day mortality rate was 18.9% (n = 14/74), and the 30-day mortality rate was 35.1% (n = 26/74).
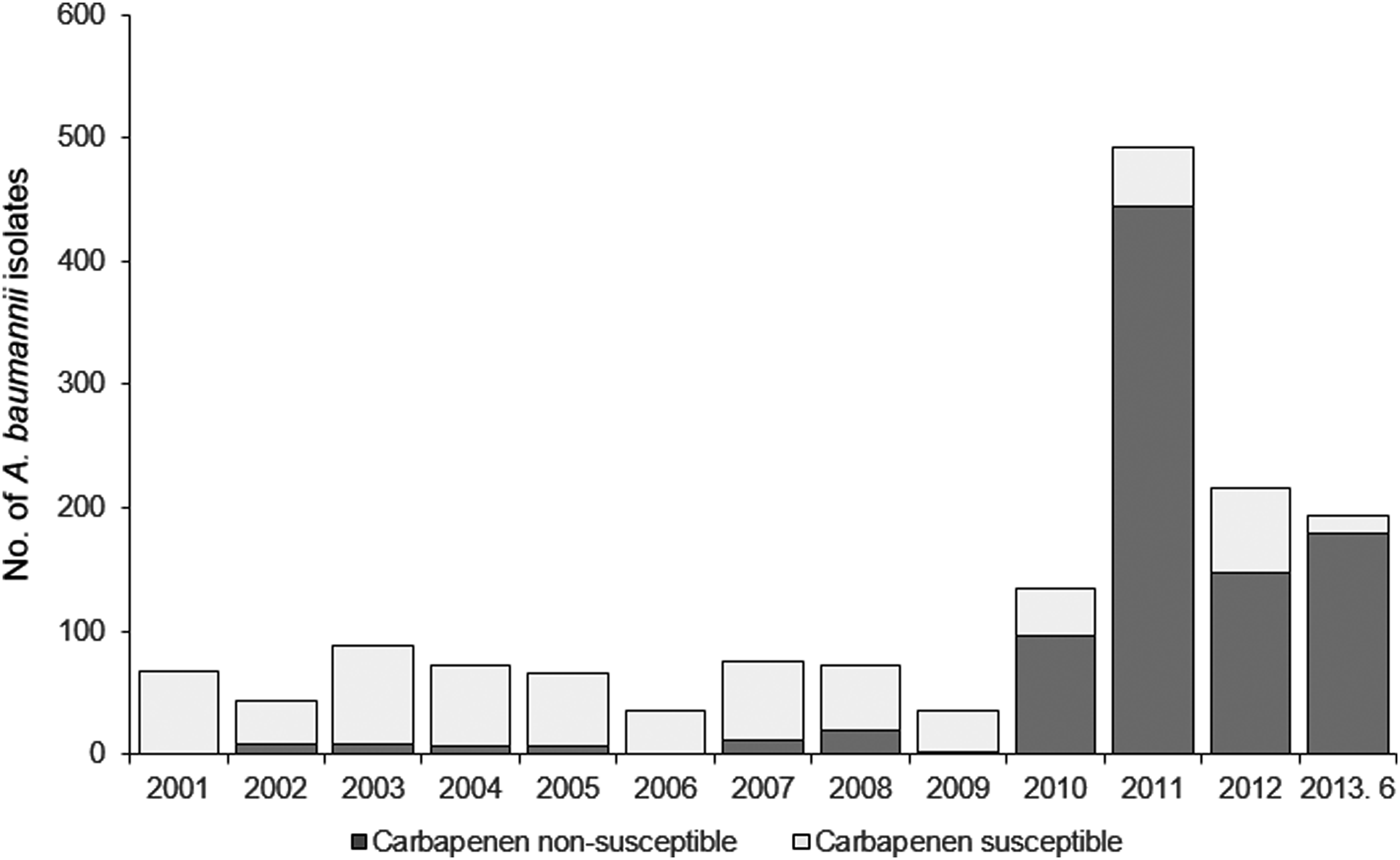
Trend of Acinetobacter baumannii isolates by carbapenem susceptibility, 2001–2013.
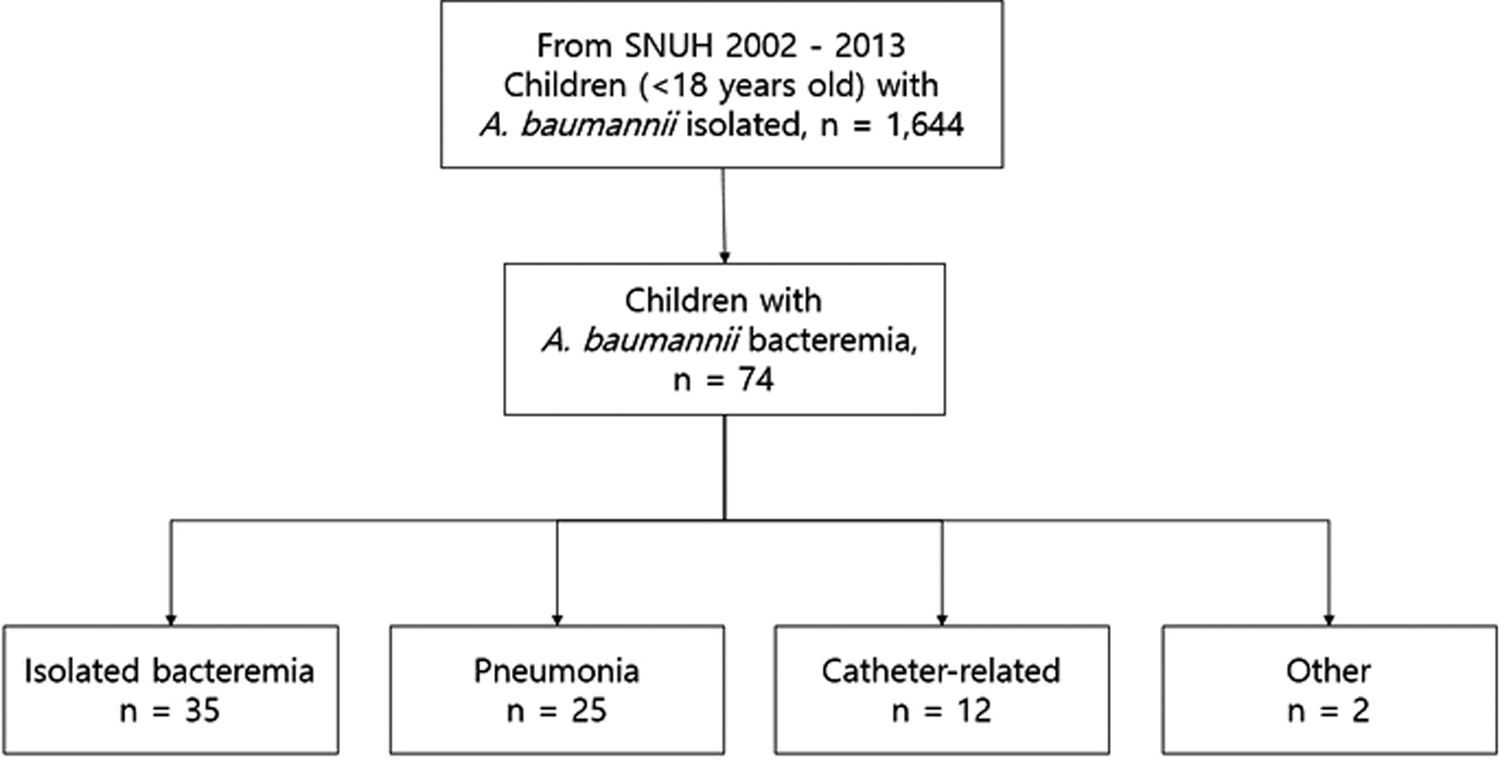
Flowchart of the number of A. baumannii cases screened, recruitment of cases, and number of cases of bacteremia in different anatomical sites.
Demographic and Clinical Characteristics of 74 Children with Acinetobacter baumannii Bacteremia
Risk factors associated with 7- and 30-day mortality
Factors associated with 7- and 30-day mortality due to A. baumannii bacteremia are described in Tables 2 and 3. The significant associated factors for 7- and 30-day mortality from the univariate analysis were identified as having a carbapenem-nonsusceptible isolate, malignancy or hematologic diseases, pneumonia, and neutropenia (Table 2). Multivariate analysis using a logistic regression model revealed that the significant independent risk factors associated with 7-day mortality were carbapenem nonsusceptibility (adjusted HR [aHR]: 2.74, 95% CI: 1.23–194.30, p = 0.034) and the presence of neutropenia (aHR: 2.55, 95% CI: 1.92–85.56, p = 0.009) (Table 3). Risk factors associated with 30-day mortality were carbapenem nonsusceptibility (aHR: 1.28, 95% CI: 1.10–11.82, p = 0.034), neutropenia (aHR: 1.68, 95% CI: 1.60–18.03, p = 0.007), and a previous ICU stay for more than 7 days (aHR: 1.15, 95% CI: 1.03–9.73, p = 0.045). Post hoc power estimates for significant variables (carbapenem nonsusceptibility, neutropenia, previous ICU stay) were all greater than 98% with Alpha of 0.05.
Univariate Analysis on Risk Factors Associated with 7- and 30-Day Mortality Among 74 Children with A. baumannii Bacteremia
CI, confidence interval; HR, hazard ratio; ICU, intensive care unit.
Multivariate Analysis on Risk Factors Associated with 7- and 30-Day Mortality Among 74 Children with A. baumannii Bacteremia
aHR, adjusted HR.
Table 4 describes the susceptibility to carbapenem and appropriateness of empirical antibiotics affecting 7- and 30-day mortality in children with A. baumannii bacteremia in the presence of neutropenia. Among neutropenic patients, none of the patients with carbapenem-susceptible pathogens died (n = 3), whereas 100% (n = 11) of the patients with nonsusceptible Acinetobacter died. In neutropenic patients, inappropriate empirical antibiotics was associated with increased mortality (90.1%) compared to patients who received appropriate empirical antibiotics (33.3%). Among nonneutropenic patients who received inappropriate empirical antibiotics, the mortality rates increased from 12.5% (4/32) at 7 days to 31.3% (10/32) at 30 days.
Susceptibility to Carbapenem and Appropriateness of Empirical Antibiotics Affecting 7- and 30-Day Mortality in Children with A. baumannii Bacteremia, by Presence of Neutropenia
Figure 3 describes 30-day mortality rates overall (A) and stratified according to the presence of neutropenia (with 95% CI in dotted line) (B). A trend toward a lower probability of survival with the neutropenic group was demonstrated (p < 0.001, by log-rank method).
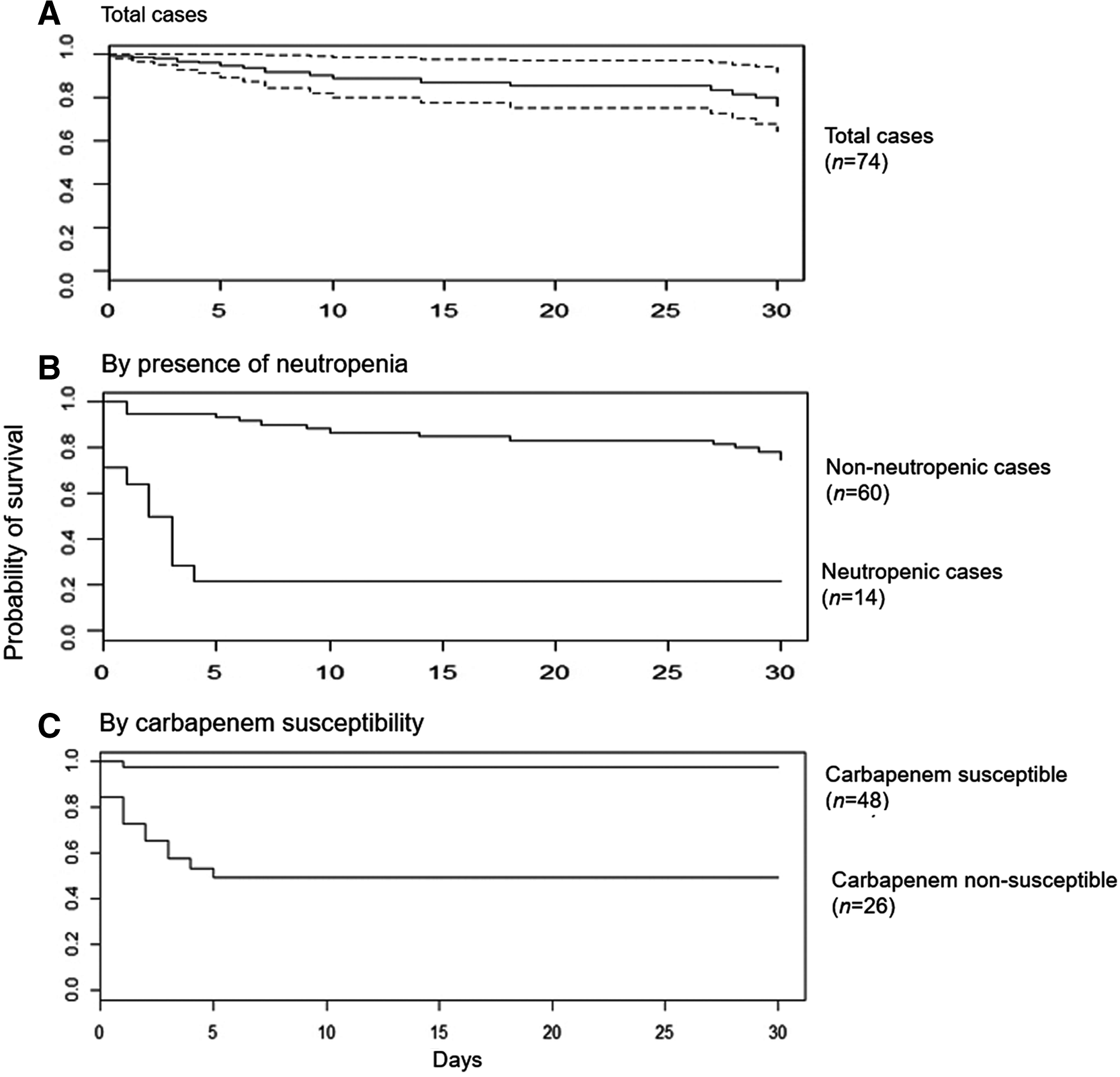
Cox proportional-hazards model curve for 30-day mortality among 74 children with A. baumannii bloodstream infection,
Discussion
In this study, we reviewed a large number of A. baumannii bacteremia cases in children in a tertiary care children's hospital setting with a wide spectrum of disease severity and a substantial burden of multidrug resistance. The significant rates of case fatality by 7 and 30 days were 18.9% and 35.1%, respectively, which are not dissimilar to findings in previous studies.7,8 Nearly one-third of the patients required inotropic support or a mechanical ventilator, and one-quarter of the patients had persistent bacteremia 48 hours after the initial blood culture. As demonstrated by other studies, A. baumannii is associated with a severe course of disease and high mortality rates. 9 As more options for immunosuppressive therapies become available, a further increase in the number of children with risk factors for A. baumannii-associated mortality is expected.
We have identified that the presence of neutropenia was an independent risk factor for 30-day mortality due to A. baumannii bacteremia in children. Neutropenia is a well-known major risk factor for developing serious infections. 10 Despite advances in supportive care, neutropenia, either acquired from chemotherapy or other reasons, may result in possible life-threatening complications in children. Our findings in the pediatric population are in agreement with previous studies that have demonstrated that neutropenia increases the risk for mortality in patients with A. baumannii bacteremia. Choi et al. reported that among 72 adult patients, the independent risk factors for mortality were found to be neutropenia and elevated Acute Physiology, Age, and Chronic Health Evaluation (APACHE) II scores. 11 A study of 52 pediatric patients with A. baumannii infections reported an overall mortality rate of 42.3%, while sepsis with neutropenia was identified as a significant factor associated with in-hospital mortality. 12 One of the largest studies that included A. baumannii bacteremia in Thai children reported that the 30-day mortality risk of A. baumannii bacteremia was 26.1%, while cancer-related neutropenia was associated with an increased risk of death with an adjusted odds ratio (OR) of 4.54 (95% CI: 1.09–18.79). 13 It is challenging to control for all known and unknown confounding factors that may play a role in the disease severity caused by A. baumannii bacteremia. Nevertheless, given the consistent association in different study populations and the biological plausibility, it would be reasonable to propose that neutropenia is an important risk factor for disease severity in pediatric patients with A. baumannii invasive infections.
In our study, 69.2% (18/26) of patients with carbapenem-nonsusceptible A. baumannii bacteremia died, which was significantly higher than the mortality in patients with carbapenem-susceptible A. baumannii bacteremia. After adjusting for clinically significant variables, a significant association was identified between nonsusceptibility and mortality in children. Previous studies have reported an association between carbapenem resistance and patient outcome. Wareham et al. found that carbapenem resistance was significantly associated with 30-day mortality among all age groups by >10% in excess with an adjusted OR of 2.27 (0.87–5.93). 14 Similarly, a study by Sheng et al. also suggested that patients with carbapenem-resistant A. baumannii bacteremia had a higher mortality rate than patients with carbapenem-susceptible A. baumannii bacteremia (46.0% vs. 28.3%, p = 0.04). 15 Given that resistant pathogens tend to be more frequently associated with patients having comorbid medical conditions, it is challenging to interpret the influence of the appropriateness of empirical antibiotics on the outcomes of such patients. There have been conflicting results among previous findings regarding whether carbapenem resistance or the inappropriateness of empirical antibiotics were related to the increased risk of mortality due to A. baumannii infections. Esterly et al. found that patients who received appropriate antibiotics were less likely to die, regardless of carbapenem resistance (93.5% vs. 74.2%, p = 0.02). 16 Subsequent multivariate analysis showed that the appropriateness of antibiotic, indeed, was the major risk factor for mortality in patients with A. baumannii bacteremia (p = 0.02). In the Korean adult population, Kwon et al. found that imipenem resistance was a major risk factor for 30-day mortality due to A. baumannii bacteremia (57.5% vs. 27.5%); however, multivariate analysis found that inappropriate antimicrobial treatment was significantly associated with the risk of mortality (adjusted OR = 6.05, 1.34, 27.3). 17 Because carbapenem-nonsusceptible A. baumannii isolates are resistant to most empirical antibiotics, these patients are more likely to receive inappropriate empirical antibiotics than the patients with carbapenem-susceptible isolates. Likely, a larger study with higher statistical power to detect the significance would be needed to answer this question. However, it would still be very challenging given the diversity of the patient population affected by A. baumannii bacteremia with multiple confounding variables to adjust.
We also found an increased risk of mortality among children with prolonged ICU stays. In general, A. baumannii is considered a nosocomial pathogen, and 50/74 (67.6%) children had prolonged prior hospital stays of more than 14 days, and 38/74 (51.4%) children had more than 7 days of ICU stays prior. In 2010–2011, we had a cluster of carbapenem-nonsusceptible A. baumannii invasive infections in the pediatric ICU, comprising a total of 13 patients, all of whom were included in this analysis. 4 The outbreak was driven by two sequence types, likely originating from a single source of transmission, causing high case fatality rates of 84.6% (11/13). It is still unclear whether the virulence was mediated by a specific phenotype of Acinetobacter or because it was clustered among patients with worse morbidity. However, it seems clear that resistant strains of Acinetobacter are associated with the adverse clinical outcomes of prolonged lengths of stay in the ICU, as observed in other studies. 18
Our findings are subject to several limitations. First, the comparison of the outcomes between the patients may have been confounded by the differences in the patient's comorbid conditions. Indeed, inappropriate empirical antibiotic and carbapenem nonsusceptibility were identified as independent risk factors for mortality in this study, although the statistical inference could not be made due to the small number of populations included in this study. Second, the potential influence of the timing of antibiotic administration (empirical and definitive) was not evaluated. Given that the untimely administration of antibiotics is associated with adverse patient outcomes, this factor may have affected the results of our analyses. Lastly, insufficient control of confounding factors of patient's clinical characteristics should be taken into account. Differences in Acinetobacter species may have affected the outcome of the patients, which were not identifiable in our study. One previous study from Korea demonstrated a high prevalence of A. nosocomialis with less resistance to carbapenem. 3 Given that our system has limited speciation of the Acinetobacter isolates, further investigation into the difference in clinical outcomes among Acinetobacter species would be of clinical interest. It is necessary to control the factors that may confound the association with mortality rates, and although we have gathered information on patient factor (age, severity of illness, and comorbidity), pathogen factor (species and antimicrobial susceptibility), and clinical practice (appropriate administration of antibiotics and previous hospitalization), we may have not had complete control over confounders.
Despite these potential limitations, our data have certain strengths. First, these data were collected over an 11-year period from the largest referral children's hospital in South Korea, which provides specialized and broad medical and surgical care for the nationwide population of 50 million. The patient population is highly diverse, with the largest volume pediatric ICU admissions and the largest oncology service in the nation, which is critical for collecting sufficient data on A. baumannii bacteremia cases in children. Second, complete clinical data were investigated to describe detailed information of each A. baumannii bacteremia case. Given the complexity of interactions between antibiotics, resistance of the pathogen, and the host factors, there are multiple variables to be taken into account for adjustment, which we aimed to obtain in this study. Despite the similarities and differences with other recently characterized A. baumannii bacteremia cases in other locations, these findings in South Korea may well represent a global “median” of illness presentation and outcome for A. baumannii bacteremia in children that is more appropriate than reports only from limited-resource health care settings.
In conclusion, we identified carbapenem nonsusceptibility, neutropenia, and prolonged ICU stay as independent risk factors for mortality due to A. baumannii bacteremia in children. The identification of risk factors for mortality demonstrates the need to identify patients at-risk of a severe course of infection. We emphasize an early and aggressive management approach in patients with neutropenia, including early hospitalization and administration of antibiotics, close observation, and monitoring until the resolution of neutropenia. The risk factors for A. baumannii infection described in this report may provide guidance for clinicians with respect to the patient's characteristics and outcomes of A. baumannii bacteremia in children.
Footnotes
Disclosure Statement
All authors, Y.J.C., H.J.L., and E.H.C., disclose that there are no commercial associations that might create a conflict of interest in connection with the submitted article. Furthermore, we confirm that all conflicts of interest, whether they are actual or potential, are not present.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.