
Abstract
Introduction:
In just two decades Acinetobacter baumannii has attained considerable importance, evolving from an insignificant organism to a leading pathogen especially in intensive care unit settings globally. Treatment options are already very limited and have almost run out due to the rapid emergence of antimicrobial resistance. Evaluation of antimicrobials that are currently in use to determine their effectiveness against multidrug-resistant (MDR) strains and developing newer options is of utmost importance. We thus set out to determine the efficacy of routinely used antibiotics against MDR A. baumannii.
Materials and Methods:
This was a cross-sectional study conducted at the Department of Microbiology, Army Medical College, National University of Medical Sciences (Rawalpindi, Pakistan) from December 2015 to June 2016. The organisms were identified on the basis of colony morphology, gram staining, catalase, oxidase, motility test, and API (analytical profile index) 20NE. The organisms were considered to be MDR when the isolate was found to be resistant to at least one agent in more than three antimicrobial groups. Antibiotic sensitivity was determined using the modified Kirby-Bauer disc diffusion method according to Clinical Laboratory Standards Institute (CLSI) guidelines.
Results:
The 77 isolates were found to have good sensitivity to tigecycline (94.8%) and minocycline (80.5%). Most of the isolates were resistant to other routinely used antibiotics.
Conclusion:
A few antibiotics, tigecycline and minocycline, are still effective against these MDR A. baumannii. We need to remain up to date regarding the efficacy of antibiotics to effectively treat patients with these MDR bacteria.
Introduction
Acinetobacter baumannii has become a global medical challenge. Initially, it was not considered a pathogen and was sensitive to most of the routinely used antibiotics. It is now an important nosocomial pathogen as it is isolated very frequently, especially in critically ill patients in intensive care units, and it is fast becoming very difficult to treat pathogen. 1 Once this pathogen enters a hospital, it is very difficult to get rid of. The main reasons for its persistence are the ability to survive on inanimate objects, desiccation tolerance, resistance to disinfectants, rapid emergence of antibiotic resistant strains, and paucity of efficacious antibiotics. 2 A. baumannii's ability to carry and transfer genes for antibiotic resistance is also one of the reasons that it has become a serious health care threat. Treatment options are limited because the currently available antibiotics are losing efficacy and pharmaceutical companies do not have any novel antibiotics in the pipeline. 3 Tigecycline and colistin were brought into clinical use to combat these multidrug-resistant (MDR) isolates.4,5 However, isolates resistant to these drugs are also being reported.6–9
A. baumannii is mostly acquired within health-care facilities. 10 To be aware of the gravity of the situation, we need to continuously monitor their rate of isolation and their susceptibility pattern to antimicrobials which are currently in use. Knowledge of the susceptibility pattern is key when deciding treatment of patients with MDR A. baumannii.
Objective
To determine the in vitro efficacy of routinely used antibiotics against these MDR-A. baumannii in our setup.
Materials and Methods
This cross-sectional study was carried out at the Department of Microbiology, Army Medical College, Rawalpindi (National University of Medical Sciences), affiliated with Military Hospital, Rawalpindi. Duration of this study was 6 months (December 2015–June 2016). Isolates were collected by nonprobability convenience sampling.
All A. baumannii isolated from the routine clinical specimens (blood, pus, urine, nasobronchial lavage and so on) received in the laboratory from Military Hospital, Rawalpindi (1100 bedded), a tertiary care hospital, were included in the study. Duplicate samples received from the same patient during same course of illness were excluded. Isolates which were not MDR were also excluded.
The isolates were identified by gram stain, catalase test, oxidase test, motility test, and analytical profile index (API 20NE) (Biomeriux). Gram negative coccobacilli that were catalase positive, oxidase negative, and nonmotile were taken and the next day identified as A. baumannii, using an API 20NE. The results of API 20NE were interpreted after 48 hours according to manufacturer's instructions.
All isolates identified as A. baumannii were subjected to susceptibility testing. The efficacy of antibiotics was determined by modified Kirby-Bauer disc diffusion method according to Clinical Laboratory Standards Institute (CLSI) guidelines. 11 A bacterial suspension equivalent to 0.5 McFarland turbidity standard was prepared of all the isolates. This was then applied on Mueller Hinton agar (oxoid) plates with the help of sterile swabs. Antibiotic discs of ceftriaxone (30 μg), trimethoprim-sulfamethoxazole (1.25/23.75 μg), amikacin (30 μg), gentamicin (10 μg), meropenem (10 μg), minocycline (30 μg), piperacillin-tazobactam (100/10 μg), ciprofloxacin (5 μg), and tigecycline (15 μg) (oxoid) were applied on Mueller Hinton agar plates. Escherichia coli (ATCC 25922) was used as the quality control strain. The plates were then incubated at 35 ± 2°C in ambient air for 20–24 hours.
Next day, the susceptibility of A. baumannii to the antibiotics was determined by observing the zone of inhibition around each disc using transmitted light. The zones were then correlated with those given in CLSI. The breakpoints used for tigecycline were ≥16 (susceptible) as suggested by Jones et al. 12
Isolates which were resistant simultaneously to at least one antibiotic in at least three classes of antibiotics were identified as MDR strains. Sensitivity pattern of the MDR isolates was noted and percentages calculated. Relevant clinical data of patients from whom these isolates were obtained were also noted.
Data were entered into and analyzed using Statistical Package for Social Sciences (SPSS) version 20.0. Qualitative variables such as gender, susceptibility to antimicrobials, and ward distribution were measured by frequency and percentages.
Results
In our study, 77 MDR isolates of A. baumannii were isolated. A total of 109 A. baumannii were isolated during the study period out of which 77 (71% approximately) were MDR, whereas 32 (29%) were non-MDR.
Of these MDR A. baumannii, 46 (59.7%) isolates were from males and 31 (40.3%) from females. The male to female ratio was 1.5:1.
These isolates were from many different setups from our hospital. Of these, 26 were isolated from the neonatal intensive care unit (NICU), 26 from ICU, 2 from pediatric ICU (PICU), 2 from nephrology ward, 4 from pediatric ward, 13 from medical ward, 1 from Armed Forces Institute of Rehabilitation Medicine, and 3 from postoperative surgical ward.
Of the 77 isolates, 22 each were isolated from blood specimen and nasobronchial lavage (NBL), 18 from Pus and pus swabs, 9 from endotracheal tips, 2 each from urine and sputum, and 1 each from CSF and eye swab. The percentages of these are shown in Fig. 1.

Distribution of isolates from various specimens. ETT, endotracheal tube; NBL, nasobronchial lavage. Color images are available online.
The results of antibiotic sensitivity were interpreted according to CLSI guidelines. 11 The sensitivity rate of the 77 isolates to the antibiotics was cotrimoxazole 17% (n = 13), gentamicin 10.4% (n = 8), amikacin 5.2% (n = 4), minocycline 80.5% (n = 62), ciprofloxacin 1.29% (n = 1), ceftriaxone 1.29% (n = 1), meropenem 6.5% (n = 5), piperacillin-tazobactam 7.8% (n = 6), and tigecycline 94.8% (n = 73). These results are summarized in Fig. 2.
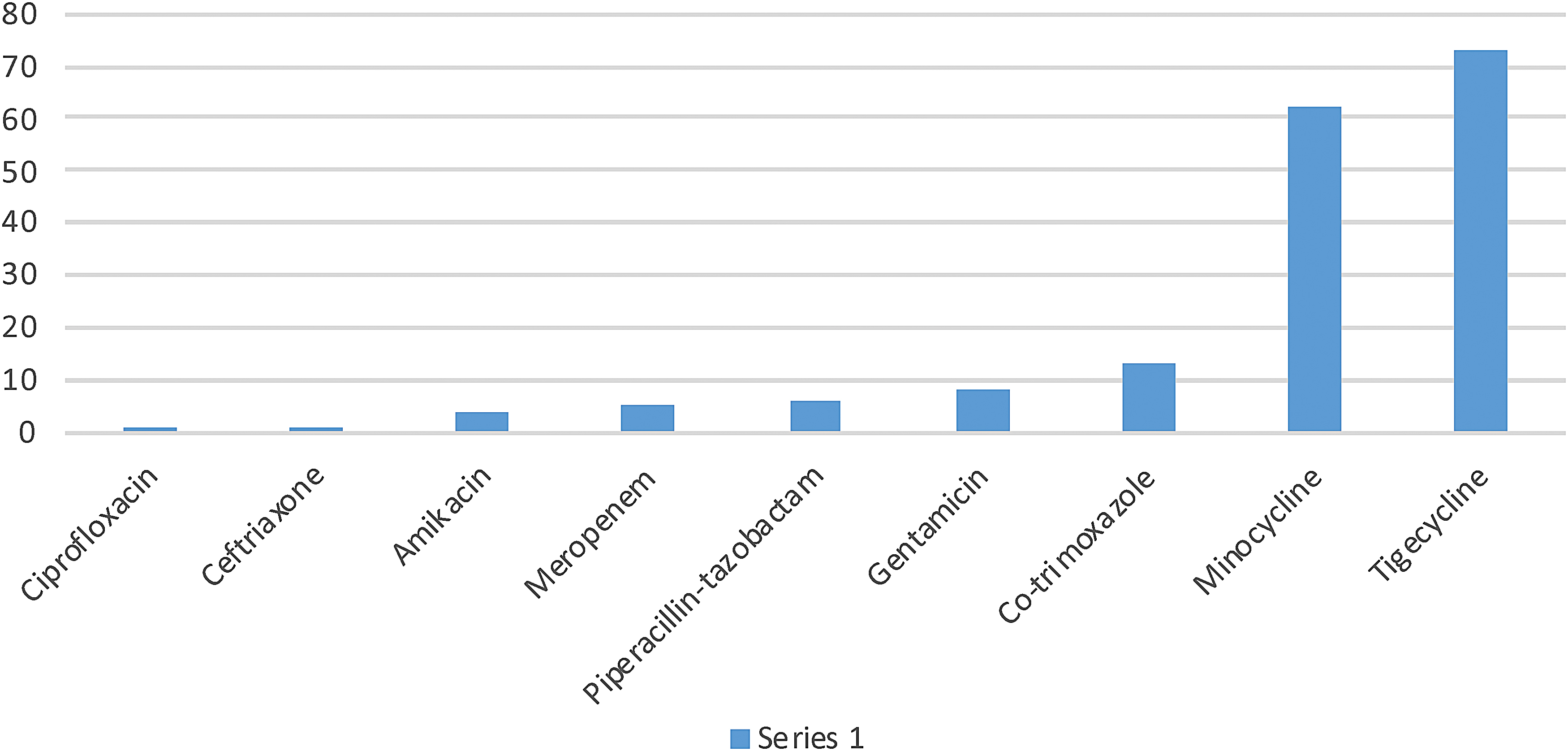
Sensitivity pattern to antibiotics (n = 77). Color images are available online.
Discussion
Acinetobacter is fast becoming an organism which when isolated from a patient becomes a source of great concern for the treating clinician. Most of the isolates in our setup are susceptible to only a few antibiotics and even those antibiotics can lead to serious adverse effects. The choice has to be made very wisely, keeping in view the condition of patient, the comorbids, and the local susceptibility pattern.
In our study, tigecycline was found to have the maximum efficacy 94.8% (n = 73) against MDR A. baumannii, followed by minocycline 80.5% (n = 62). Begum et al. from Islamabad conducted a study from February 2011 to December 2011 and found that Acinetobacter showed highest sensitivity to minocycline (100%) and tigecycline (91%) and were resistant to cephalosporins, carbapenems, flouroquinolones, and β-lactam drugs. 13
Sahu et al. carried out a surveillance study in Odisha from April 2015 to March 2016 in the Department of Microbiology at a Tertiary Care Teaching Hospital. They found that maximum isolates were sensitive to tigecycline (99.56%) and colistin (96.47%), then amikacin (30.39%), levofloxacin (29.95%), meropenem (25.55%), ampicillin-sulbactam (95.15%), cefepime-tazobactam (94.27%), tobramycin (92.51%), and ceftriaxone-tazobactam (89.43%). They found that out of the 227 isolates of Acinetobacter species, 71 (31.28%) were extended spectrum beta lactamase (ESBL) producers and 144 (63.44%) isolates were MDR, and 8 cases (3.52%) were resistant to colistin. One pan-drug isolate was also found. 14
Another study was conducted at Aseer Central Hospital, Saudi Arabia from 2014 to 2015. Out of the 105 Acinetobacter isolates, 103 (98.1%) were found to be MDR. Of these, the A. baumannii strains showed 100% sensitivity to colistin and cotrimoxazole (74.5%). Remaining 19 antimicrobials revealed little or no efficacy: amikacin 16.3%; ampicillin7.7%; and ceftazidime 7.3%. 15
Janahiraman et al. conducted a study on MDR A. baumannii from a tertiary care hospital in Malaysia. They found that of the 64 MDR A. baumannii 80.6% (n = 57) that were resistant to cephalosporins, 66.7 (n = 46) were resistant to carbapenems. 16
Zhao et al. in 2015 determined the resistance rates of Acinetobacter to antibiotics, which were ampicillin (78.5%), cefotetan (76.9%), cefazolin (78.5%), ceftriaxone (75.4%), imipenem (92.3%), gentamicin (87.7%), levofloxacin (80%), nitrofurantoin (78.5%), ampicillin/sulbactam (93.8%), piperacillin/tazobactam (89.2%), ceftazidime (92.3%), cefepime (92.3%), aztreonam (92.3%), ciprofloxacin (98.5%), co-trimoxazole (81.5%), tobramycin (81.5%), cefoperazone (21.5%), and cefoperazone/sulbactam (18.5%). 17
Vaja et al. from Gujarat found that resistance to meropenem was 41.67%, piperacillin-tazobactum (58.34%), amikacin (52.09%), ceftazidime (79.71%), gentamicin (62.5%), and levoflaxacin (68.75%). 18
In our setup, MDR A. baumannii (MDRA) are being encountered very commonly from clinical specimens. We need to curb the injudicious use of the last resort antibiotics—colistin and tigecycline as much as possible. Their use should be limited for only those patients harboring MDRA. For the other patients, strict adherence to the other currently available antibiotics which are efficacious according to the antibiotic susceptibility pattern should be sought. Otherwise the occasional colistin- and tigecycline-resistant isolates that are seen may become an uncontrollable epidemic.
In our study majority isolates were from NBL and blood, followed by pus/pus swabs and tips. Sahu et al. showed that they had maximum isolates from wound swab/pus (48.46%) then tracheal aspirate (16.74%), urine (15.86%), sputum (9.25%), and blood (3.96%). 14 Begum et al. found A. baumannii to be most prevalent in endotracheal tube secretions n = 23 (25.27%), followed by tracheal secretions n = 18 (19.78%) and pus n = 15 (16.48%). 13 In the study by Zhao et al. conducted from 2011 to 2013 most of the strains were isolated from sputum 112 (93.3%), while the others were from endotracheal tube suction, blood, urine, bronchoalveolar lavage, and so on. 17 From Gujarat, Vaja et al. found Acinetobacter species from blood were 24 (50%), pus 15 (31.25%), urine 4 (8.33%), CSF 2 (4.18%), sputum 1 (2.08%), plural fluid 1 (2.08%), and tracheal aspirate 1 (2.08%).
We received maximum isolates from ICU and NICU. Sahu et al. also got many isolates from ICU (47.14%), then from surgical departments (27.75%), medicinal departments (14.54%), and outpatient departments (OPDs) (10.57%). Hundred forty-four (63.44%) isolates were MDR strains. 14 Begum et al. also isolated the maximum A. baumannii from NICU (42.85%), medical ICU (19.78%), and 9.89% from OPD. 13 In the study by Zhao et al., isolates were mainly from respiratory department (21.7%), ICU (16.7%), and emergency department (11.7%). Of these, most of the MDR strains were from ICU (29.7%) and emergency department (20.3%). 17 Vaja et al. out of their 48 isolates had maximum from pediatric 23 (47.94%), surgical 13 (27.08%), medical 05 (10.41%), obstetrics and gynecology 05 (10.41%) tuberculosis (TB), and chest 02 (4.16%). 18
Conclusion
A. baumannii is being routinely isolated from patients in intensive care, especially those who are on ventilator support. Of these the MDR isolates are heading toward resistance to almost all the antibiotics. Minocycline and tigecycline may be used for some time, but they also have severe adverse effects associated with use. We have switched to use of colistin, as a last resort, but for how long? Injudicious use of antibiotics has paved the way for pan-drug-resistant isolates. We need to continuously monitor the isolations and susceptibility pattern of this pathogen. Moving toward antibiotic stewardship is the best and the only approach to reserve antibiotics that may retain efficacy. Otherwise, we may end up in an era where there will be no effective antibiotics.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was taken for this research.