
Abstract
With the increasing emergence of drug resistance in enterococci, there have been very limited data on the efficacy of orally available nitrofurantoin and fosfomycin on enterococci causing urinary tract infections (UTIs), particularly for multidrug-resistant (MDR) strains. This study aimed to determine the in vitro effectiveness of these two drugs against the MDR enterococci. A total of 514 phenotypically and genotypically confirmed isolates of enterococci (239, 46.5% Enterococcus faecalis and 275, 53.5% Enterococcus faecium) showed E. faecalis as significantly more resistant (p < 0.05) to ciprofloxacin and high strength gentamicin. Vancomycin resistance was seen in 37 (7.2%) isolates. Of these, 114 (22.18%) isolates (51, 44.73% E. faecalis and 63, 55.26% E. faecium) were MDR. Nitrofurantoin minimum inhibitory concentrations (MICs) for the MDR enterococci varied from 1 to 128 μg/mL (MIC50 8 μg/mL, MIC90 64 μg/mL for E. faecalis), while fosfomycin MICs for the MDR E. faecalis, including vancomycin resistant enterococci (VRE) were in susceptible range (≤64 μg/mL, MIC50 8 μg/mL, MIC90 16 μg/mL). An efficacy ratio of ≥8 for nitrofurantoin was observed in the 39 (76.5%) MDR E. faecalis and 44 (69.8%) MDR E. faecium isolates as against the 50 (98%) E. faecalis isolates for fosfomycin. Although nitrofurantoin has been widely prescribed for the treatment of UTIs for the past several years, it was still found to be active in vitro against the urinary isolates of MDR enterococci, including VRE. As for fosfomycin, it holds robust potential to be used against the urinary MDR enterococci and VRE (E. faecalis).
Introduction
The increasing emergence of drug resistance in enterococci has posed a great challenge in deciding the most appropriate treatment in cases of enterococcal infections. Urinary tract infections (UTIs) are the most common infections caused by enterococci, often being the second most common organism isolated after Escherichia coli (E. coli). 1 Although the majority of UTI caused by enterococci are hospital acquired, 2 the burden of enterococcal UTI in the community is also bothersome. Clinicians are often challenged with the choice of antibiotics to prescribe while treating patients of UTI in the outpatient setting, where oral formulations are preferred over injectable treatments by patients. In this regard, while previously prescribed oral antimicrobials such as aminopenicillins and fluoroquinolones have fallen out of empirical choice for the treatment of UTI, there has been renewed interest in two old drugs, namely, nitrofurantoin and fosfomycin. 3
Nitrofurantoin has been recommended as the first choice therapy for uncomplicated cystitis and pyelonephritis in women by Infectious Diseases Society of America (IDSA) and European Society of Clinical Microbiology and Infectious Diseases (ESCMID). 4 Similarly fosfomycin has been recommended as the first line of treatment for acute uncomplicated UTI in women. 5 It is indicated only for UTI due to E. coli and Enterococcus spp., Enterococcus faecalis in particular. 6 There has been substantial evidence on the efficacy of fosfomycin and nitrofurantoin on E. coli. 7 However, there have been very limited data on the efficacy of these antibiotics on enterococcal infections, particularly for the multidrug-resistant (MDR) strains.3,8 This study was conducted to determine the susceptibility profile of the enterococcal isolates causing UTI from patients attending the outpatient department (OPD) of a tertiary care referral hospital, with emphasis on nitrofurantoin and fosfomycin.
Materials and Methods
Study site and isolates
The study was conducted in the Department of Microbiology, Institute of Medical Sciences, Banaras Hindu University and the allied tertiary care university hospital catering to the needs of a densely populated Indian territory and abutting region of Nepal (Fig. 1). Prospectively obtained urinary isolates of enterococci in the Microbiology laboratory over a period of 10 years (January 2008–December 2017) were considered for this study. The study was approved by the Institute Ethics Committee. Informed consent was obtained from all the subjects before sample collection in the study.

Portion of Indian subcontinent (in map) showing the catchment area of the study center.
Inclusion and exclusion criteria for the enterococcal isolates
Only those isolates were included in the study that met the following requirements; (1) enterococci isolated from the patients with clinical diagnosis of acute UTI, 9 (2) enterococci isolated as a single pathogen from urine of patients attending the OPD of the hospital, (3) colony count of the isolate was ≥103 colony-forming units/mL (cfu/mL) in semiquantitative urine culture, (4) UTI caused by E. faecalis and Enterococcus faecium as the only enterococcal species, and (5) patients in the age group 18–60 years.
Isolates were excluded based on the following criteria: (1) enterococci isolated from urine of catheterized patients, (2) enterococci as a part of mixed flora in urine, (3) cases associated with chronic conditions such as obstructive uropathies, hypertension, diabetes and so on, and (4) enterococci isolated from the urine of pregnant women.
Isolation and presumptive identification of enterococci
Freshly collected midstream urine specimens from the patients along with their clinical details were received in the Microbiology laboratory. The specimens were immediately cultured in a semiquantitative manner on cysteine lactose electrolyte deficient (CLED) agar (HiMedia Laboratories Pvt. Ltd., India) and incubated overnight at 37°C. Presumptive identification of enterococci from the growth on CLED agar on the following day was made with Gram's staining, catalase test, bile esculin hydrolysis, and growth in 6.5% sodium chloride. 10 Confirmation of enterococci was done by the growth at pH 9.6 and hydrolysis of pyrrolidonyl β-naphthylamide broth following the Facklam Collin's classification protocol. 11 Further speciation of the confirmed isolates was done by a host of biochemical tests, including carbohydrate fermentation media containing mannitol, sorbitol, sorbose, arabinose, raffinose, lactose, sucrose (Sigma-Aldrich Chemicals Pvt. Ltd., India), and pyruvate (HiMedia Laboratories Pvt. Ltd.), as per reference. 11
Molecular confirmation of isolates
All the phenotypically identified isolates of enterococci were confirmed as E. faecalis and E. faecium based on polymerase chain reaction amplification of the ddl genes encoding the D-alanine–D-alanine ligases specific for E. faecalis (ddl E. faecalis) and E. faecium (ddl E. faecium) as per reference. 12
Antimicrobial susceptibility testing
Genotypically confirmed E. faecalis and E. faecium isolates were subjected to Kirby-Bauer disc diffusion method with ampicillin (10 μg), ciprofloxacin (5 μg), nitrofurantoin (300 μg), linezolid (30 μg), and high strength gentamicin (120 μg) discs (HiMedia Laboratories Pvt. Ltd.), as per Clinical Laboratory and Standards Institute (CLSI) standards. 13 Presumptive vancomycin resistance was determined with vancomycin agar screen containing 6 μg/mL vancomycin (Sigma-Aldrich Chemicals Pvt. Ltd.). 13 All the enterococcal isolates with presumptive vancomycin resistance were tested with Vancomycin HiComb™ MIC Strip (HiMedia Laboratories Pvt. Ltd.) for determination of vancomycin minimum inhibitory concentration (MIC) ranging from 1 to 256 μg/mL.
Based on the resistance profile, enterococci were specified as MDR if nonsusceptibility to at least one antimicrobial agent in three or more antimicrobial categories was observed. 14
Determination of nitrofurantoin and fosfomycin MIC
MIC of nitrofurantoin was determined with E-strips (HiMedia Laboratories Pvt. Ltd.) for all the MDR enterococci and vancomycin-resistant enterococci (VRE). Nitrofurantoin MIC ≥128 μg/mL was considered as resistant. 13 Etest was also used to determine fosfomycin MIC (HiMedia Laboratories Pvt. Ltd.) for all the MDR E. faecalis, which also included all the vancomycin-resistant E. faecalis isolates. MICs ≤64 μg/mL for fosfomycin was considered as the susceptibility breakpoint.6,13 The MDR E. faecalis isolates were also tested with fosfomycin discs (200 μg; supplemented with 50 μg of glucose-6-phosphate) by the disc diffusion method as per CLSI standards. 13 E. faecalis ATCC 29212 strain was used for quality control (QC) in Etest, vancomycin screen agar and disc diffusion test for high-level gentamicin resistance (HLGR), and Staphylococcus aureus ATCC 25923 was used for QC in disc diffusion test with other antibiotic discs.
Calculation of efficacy ratio
The efficacy ratio, which is a measurement of how far the measured MIC is from the resistant breakpoint for that drug, 15 was calculated by dividing the “resistant” breakpoint MIC for the particular drug with the measured MIC of the drug.
Calculation of categorical agreement
Categorical agreement for nitrofurantoin and fosfomycin Etest was calculated as the percentage of isolates producing the same category result (susceptible, intermediate, or resistant) compared to the respective disc diffusion method according to the CLSI break points. The error rates were based on the discrepancies in the MIC by Etest that lead to an interpretative or categorical change from the result yielded by the standard method. A categorical agreement of ≥90% was considered acceptable.16,17
Statistical analysis
Antimicrobial resistance profile of E. faecalis and E. faecium isolates were compared with respect to the antibiotics by chi-square test using MedCalc version 16.4.3. Resistance of E. faecalis and E. faecium to nitrofurantoin over the study period was compared by the Fischer's exact test.
Results
A total of 514 cases of enterococcal UTI in the patients attending the OPD were studied. From the cases, 514 consecutive nonduplicate enterococcal isolates, satisfying the defined criteria, were included in the study. Both phenotypic and genotypic methods identified 239 (46.5%) enterococcal isolates as E. faecalis and remaining (275; 53.5%) as E. faecium. Resistance of both the E. faecalis and E. faecium isolates to different antibiotics has been shown in Table 1. The isolates of E. faecalis were significantly more resistant (p < 0.05) to ciprofloxacin and high strength gentamicin as compared to E. faecium. Vancomycin resistance was seen in 37 (7.2%) isolates comprising of 16 E. faecalis and 21 E. faecium. All the enterococcal isolates were susceptible to linezolid.
Antibiotic Resistance Profile of Enterococcal Isolates
Result of vancomycin agar screen.
p < 0.05, chi-square test applied.
Among the total isolates, 114 (22.18%) isolates comprising of 51 E. faecalis (44.73%) and 63 E. faecium (55.26%) met the definition of MDR. These MDR isolates included all the vancomycin-resistant E. faecalis and 16 (76.19%) of the vancomycin-resistant E. faecium isolates. Nitrofurantoin MICs for the MDR enterococci varied from 1 to 128 μg/mL (median MIC value 8 μg/mL). The MIC50 and MIC90 for nitrofurantoin against the MDR E. faecalis were 8 and 64 μg/mL, respectively, whereas the same against the MDR E. faecium were 16 and 64 μg/mL, respectively. Based on the MIC interpretative criteria by CLSI, nitrofurantoin resistance (≥128 μg/mL) and intermediate susceptibility to nitrofurantoin (64 μg/mL) were observed in 2 (5.88%) and 5 (1.96%) of the MDR E. faecium isolates, respectively, and four each of the MDR E. faecalis isolates (Fig. 2). Among the VRE isolates, 2 (12.5%) E. faecalis isolates and 2 (9.5%) E. faecium isolates were resistant to nitrofurantoin. Susceptibility trend (based on the MIC values) of the MDR enterococci over years to nitrofurantoin has been mentioned in Figs. 3 and 4. There was an increasing trend in nitrofurantoin resistance during 2014–2017 compared to 2008–2011 for both E. faecalis and E. faecium, although not significant (p = 0.28 and 0.17, respectively). The efficacy ratio for nitrofurantoin varied from 4 to 128 in both the MDR E. faecalis and MDR E. faecium isolates, which were susceptible to nitrofurantoin as per the calculated MIC values. In addition, among these, for the 39 (76.5%) MDR E. faecalis and 44 (69.8%) MDR E. faecium isolates, an efficacy ratio of ≥8 for nitrofurantoin was observed.
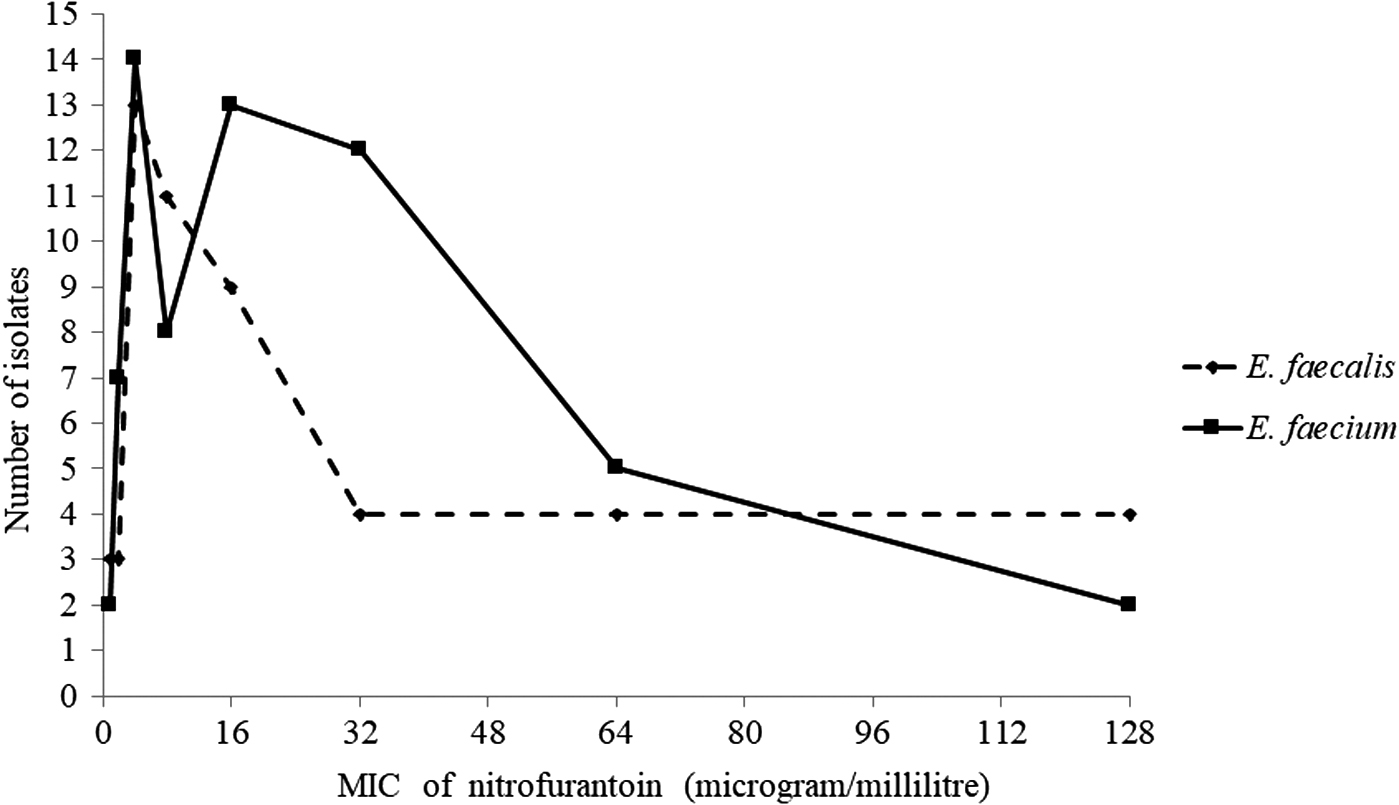
Frequency polygon depicting distribution of nitrofurantoin MICs against Enterococcus spp. MIC, minimum inhibitory concentration.
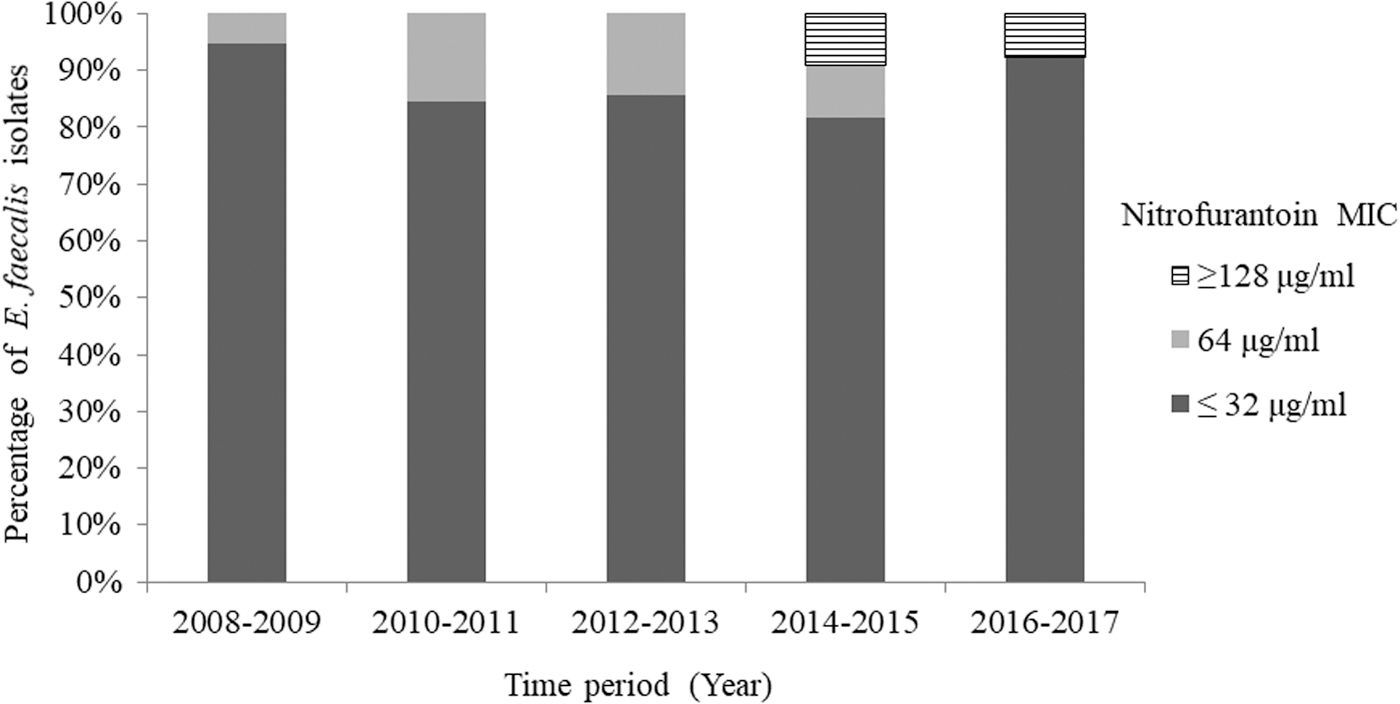
Trend in nitrofurantoin resistance in Enterococcus faecalis over the study period (2008–2017).

Trend in nitrofurantoin resistance in Enterococcus faecium over the study period (2008–2017).
Fosfomycin MICs for all the MDR isolates of E. faecalis were in susceptible range (≤64 μg/mL) and varied from 2 to 64 μg/mL (median MIC value 8 μg/mL). The MIC50 and MIC90 for fosfomycin against the MDR E. faecalis were 8 and 16 μg/mL, respectively. Frequency of the isolates with different fosfomycin MIC values has been shown in Fig. 5. All the 16 vancomycin-resistant E. faecalis were susceptible to fosfomycin. No difference in the fosfomycin susceptibility results was observed between the Etest and the disc diffusion methods. There was 100% categorical agreement between both the tests (Table 2). The efficacy ratio for fosfomycin ranged from 4 to 128 in the MDR E. faecalis isolates, with efficacy ratio of ≥8 observed in 50 (98%) of the isolates.

Frequency polygon depicting distribution of fosfomycin MICs against E. faecalis.
Agreement Between Etest and Disc Diffusion Methods for Susceptibility Testing for Nitrofurantoin and Fosfomycin
Discussion
Enterococcus has long been heralded as a dominant pathogen in UTIs. Although UTIs due to Enterococcus spp is mostly encountered among the hospitalized patients, 2 several studies have particularly emphasized its impact on the community acquired culture proven infections.18,19 In a recent surveillance report of acute community acquired urinary tract bacterial infections published from India, Enterococcus spp was reported as the third most common etiological agent (11.77% of the total urinary isolates) after E. coli and S. aureus. 20 In another study, E. faecalis was the second most common organism causing UTI among the women in the reproductive age group in the Gynecology OPD. 21 As most of the UTI caused by enterococci arise from patient's endogenous flora, 1 they could also contribute to the bulk of community acquired UTI.
Management of enterococcal UTI has become challenging with limited therapeutic options available to treat the MDR strains. This study revealed considerable antimicrobial resistance in enterococci with 22.18% of the total isolates as MDR, exhibiting notable resistance to ampicillin (49.03%), high-strength gentamicin (49.22%), and ciprofloxacin (90.08%). Among the oral therapeutic options available for treatment of UTI in outpatient settings, fluoroquinolones have been regarded as an important alternative since long. However, for the empirical treatment of enterococcal UTI, fluoroquinolones are no longer effective especially in regions where resistance rates are above 10%. 22 High rates of resistance to ampicillin and HLG have also limited their synergistic use for treatment. Similar studies from the subcontinent and elsewhere have reported alarming resistance of enterococci against these drugs.1,8,18–21 In a study on the community acquired enterococcal UTI by Goel et al. from north India, HLGR was noticed in 32.7% and 47.6% of the E. faecalis and E. faecium, respectively. 23 Consequently, the options remaining for treatment of uncomplicated enterococcal UTI through oral route are nitrofurantoin and fosfomycin. While there have been very limited data on in vitro activity of nitrofurantoin especially against VRE, there have also been insufficient data for susceptibility of enterococci to fosfomycin. 3 The current study probably provides the largest data on the in vitro activity of these two drugs against the MDR enterococci based on the MIC.
Increasing emergence of the VRE causing UTI is a great concern particularly due to the increased cost and mortality associated with it. In addition, limited therapeutic options for the VRE isolates aggravate the problem. In this regard, nitrofurantoin, fosfomycin, and doxycycline are the available options for VRE UTI, that can be administered orally. 24 The present study showed nitrofurantoin resistance rates of 15.37% for enterococcci and 10.81% for the VRE. Along with this, nitrofurantoin was almost equally active in vitro in the MDR enterococci as in the non-MDR enterococcal isolates. There have been reports of low or no resistance to nitrofurantoin in literature owing to the multiple sites of action of the drug. 3 In addition, nitrofurantoin has been reported to have lesser side effects. 3 Resistance rates in enterococci have varied from 6% to 17% in India. 3 Among the few studies, 100% susceptibility rates have been found for both nitrofurantoin and fosfomycin, even for VRE when tested by the disc diffusion method. 25 Similarly, no significant resistance to nitrofurantoin has been found in any of the vancomycin-resistant E. faecalis isolated from urine samples in another study. 26 Another study reported resistance rates of 1.5% to nitrofurantoin in the E. faecalis and 39.4% in the E. faecium while 2.3% resistance in the E. faecalis to fosfomycin. 27 Only one isolate of the E. faecalis (1.3%) with intermediate susceptibility and five isolates (6.7%) with resistance to fosfomycin was reported in one of the studies by the disc diffusion method. 28 No resistance to fosfomycin in VRE has been reported from urine in another similar study. 27 As mainly mutations are responsible for fosfomycin resistance, rapid development is unlikely. 29 However, it was evident from this study that there has been an increase in the nitrofurantoin resistance over the years in both E. faecalis and E. faecium. A similar trend in nitrofurantoin resistance has also been observed in another recent study over a period of 10 years. 26 A judicious and prudent use of nitrofurantoin is the need of the hour, even though relatively lower rates of resistance has been reported amidst widespread use of this drug for UTI. Nitrofurantoin resistance is primarily caused by mutations in the genes encoding the nitroreductases, namely nfsA and nfsB. There has been recent report of clinically proven nitrofurantoin resistance mediated by the efflux pumps. 30 Although not within the scope of this study, this emerging nitrofurantoin resistance in enterococci should be studied for the most probable mechanisms of resistance owing to the ability of these plasmid-mediated efflux pump genes for widespread dissemination.
Interestingly, in vitro resistance to fosfomycin owing to the loss of transporters is more common than the actual in vivo resistance. 29 Fosfomycin MIC for all the MDR (including vancomycin resistant) E. faecalis isolates was in the susceptible range in the present study. This overwhelming susceptibility to fosfomycin against the urinary E. faecalis could be attributed to the limited use of fosfomycin in our community and hospitals.
We compared the relative in vitro activity of nitrofurantoin and fosfomycin for treating enterococcal UTI by measuring efficacy ratio for each isolate in addition to the resistant breakpoint MIC. Efficacy ratio of ≥8 for fosfomycin was calculated in 98% E. faecalis isolates, while efficacy ratio for nitrofurantoin was ≥8 in only 76.5% E. faecalis isolates. As a drug with a high efficacy ratio is believed to be more active in vitro than a drug with a lower efficacy ratio, 15 fosfomycin was found to be more active than nitrofurantoin against the urinary MDR E. faecalis. However, it is emphasized that in vitro activity of these two drugs presented in this study adds to the scarce susceptibility data available in the literature to help the clinicians in deciding the appropriate oral therapy for uncomplicated enterococcal UTI.
As molecular mechanism of resistance was not studied, clinical efficacy of these drugs could not be ascertained. There have been reports of discrepancies in fosfomycin resistance between high frequencies of in vitro mutations and actual rates of clinical resistance, which is universally low. 29 Nevertheless, the activities of both the drugs against enterococci support the widely reported low level of resistance to nitrofurantoin and fosfomycin in other organisms.3,5,21,23
There have been issues with the antimicrobial susceptibility testing methods with fosfomycin due to the requirement of glucose-6-phosphate, lack of an approved broth dilution method, and the requirement of the cumbersome agar dilution and disc diffusion methods. 6 The study preferred Etest for determining fosfomycin MIC and also used fosfomycin disc diffusion test over agar dilution method against E. faecalis. The CLSI approved agar dilution method is restricted to research settings and is one of the potential factors for limited use of fosfomycin. 6 Fosfomycin MICs by Etest correlated well with the result of fosfomycin disc diffusion with 100% categorical agreement as per the CLSI susceptibility break point. The use of Etest in this study could be affirmed with the study by Hirsch et al., which suggested that Etest could be used for enterococcal isolates to accurately measure the MICs. 6 However, the inability to perform the agar dilution test for fosfomycin for all the isolates was one of the limitations of this study. Furthermore, the study was based on in vitro susceptibility testing of the isolates. Evaluation of clinical response to these drugs in the patients with enterococcal UTI could better predict the actual situation.
Conclusion
Although nitrofurantoin has been widely prescribed for the treatment of UTIs for past several years, it is still found to be active against the urinary isolates of MDR enterococci, including VRE. As for fosfomycin, it holds robust potential to be used against the urinary MDR and vancomycin-resistant E. faecalis, but should be judiciously prescribed as a reserved drug in light of its safety profile and current recommendations.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors thank Banaras Hindu University for providing basic infrastructure and laboratory grant (R/Dev/D/Upgradation of IMS/5015/7746 to T.B.).