
Abstract
The emergence of carbapenem-resistant Klebsiella pneumoniae (CRKP) has posed a great threat to public health. Among 133 nonduplicated CRKP isolates collected between September 2016 and November 2017 in a tertiary hospital in China, 89 (89/133, 66.9%) and 31 (31/133, 23.3%) were positive for blaNDM-5 and blaKPC-2. Multilocus sequence typing (MLST) and pulsed-field gel electrophoresis (PFGE) revealed that ST290 represented the majority of NDM-5 producers (67/89, 75.3%) and PFGE cluster E accounted for 50 (50/67, 74.6%) ST290 isolates from the burn ward, suggesting that K. pneumoniae ST290 clone carrying blaNDM-5 resulted in an outbreak in this hospital. Whole genome sequencing of the plasmid carrying blaNDM-5 showed that the resistance gene blaNDM-5 was located in a ∼49 kb multireplicon plasmid with a peculiar insertion of ISKpn19 of the IncX3-type plasmid. To the best of our knowledge, this is the first report of outbreak of K. pneumoniae ST290 clone carrying blaNDM-5.
Introduction
Over the past few decades, the emergence of carbapenem-resistant Klebsiella pneumoniae (CRKP) has posed an increasing threat to public health worldwide.1–4 The main mechanism of carbapenem resistance is the production of carbapenemases. Of note, KPC-2-producing K. pneumoniae ST11 has been demonstrated to be a predominant epidemic clone in China. 5 NDM-5, a variant of NDM-1, was first found in an Escherichia coli isolate ST648 from a patient in the United Kingdom with a history of hospitalization in India. 6 Since then, NDM-5-producing E. coli has attracted extensive attention.7–14 However, the occurrence of blaNDM-5-harboring K. pneumoniae was sporadic. In this study, we aim to describe the first outbreak caused by a novel ST290 clone of K. pneumoniae carrying blaNDM-5 with intrahospital transmission.
Materials and Methods
Bacterial isolates and antimicrobial susceptibility testing
A total of 133 nonduplicated CRKP isolates were collected at Hwa Mei Hospital, University of Chinese Academy of Sciences in the east of China, between 2016 and 2017. These isolates, from different sources of specimens from clinical departments, were identified by Vitek 2 Compact (bioMérieux, France). Antimicrobial susceptibility testing was conducted using the Vitek-AST-GN16 card according to the manufacturer's instructions. The minimum inhibitory concentrations of imipenem and ertapenem against the bacteria were validated by disk diffusion testing. The results were interpreted according to Clinical and Laboratory Standard Institute Breakpoints (CLSI-2018). 15 E. coli ATCC25922 was applied as a quality control isolate.
Phenotypic and genotypic determinations
Phenotypic detection to confirm carbapenemase production was determined using Modified Carbapenem Inactivation Method (mCIM) and ethylenediaminetetraacetic acid-Modified Carbapenem Inactivation Method (eCIM), which are recommended by CLSI. Multiplex PCR for carbapenemase genes including blaKPC, blaGES, blaSPM, blaIMP, blaVIM, blaOXA, and blaNDM was performed after phenotypic characterization as previously described.16,17 Positive amplification products were sent for Sanger sequencing by TSINGKE Co. (Hangzhou, China).
Homology analysis
Pulsed-field gel electrophoresis (PFGE) was performed to demonstrate the phylogenetic relatedness of the NDM-5-producing K. pneumoniae isolates. The DNA fragments from tested bacteria underwent electrophoresis by XbaI-PFGE (CHEF Mapper™; Bio-Rad) and band profiles were then compared by BioNumerics software with the Dice coefficient with 1.5% band tolerance and 1.5% optimization. Clusters were defined as DNA patterns sharing ≥80% similarity. The universal standard strain H9812 was referred to as the size marker.
Multilocus sequence typing (MLST) was applied to determine sequence types (STs) of the targets through sequencing of seven housekeeping genes of K. pneumoniae (gapA, infB, mdh, pgi, phoE, rpoB, and tonB). The different sequences present within the bacteria were assigned as distinct alleles representing the allelic profile or specific ST at the loci for each isolate.
Plasmid depicting
The PCR product of the plasmid DNA extracted and purified from K. pneumoniae ST290 carrying blaNDM-5 was completely sequenced by Illumina MiSeq platform. The gaps between the contigs were closed for assembling, and the relative position of contigs was determined in the mapping procedure. Open reading frames (ORFs) were predicted and annotated by RAST server. 18 Sequences comparison and alignment was performed by MEGA 5.01. 19
Results
Isolate characteristics and antimicrobial susceptibility testing
Among 133 CRKP isolates, variety of clinical specimens was involved as follows: wound (48/133, 36.1%), blood (27/133, 20.3%), sputum (36/133, 27.1%), catheter (10/133, 7.5%), drain fluid (8/133, 6.0%), urine (3/133, 2.2%), and bronchial lavage (1/133, 0.8%). The majority of isolates were retrieved from patients on the burn ward (68/133, 51.1%), followed by intensive care unit (ICU; 27/133, 20.3%), emergency intensive care unit (EICU; 7/133, 5.3%), and other wards (31/133; 23.3%). The average age of patients infected or colonized by these bacteria was 51.4 ± 16.3 years. The results of antimicrobial susceptibility testing in Table 1 showed that these isolates displayed high resistance to most antibiotics including carbapenems, cephalosporins, and β-lactamase inhibitors. However, ST290 K. pneumoniae strains tended to be more susceptible to fluoroquinolones, aminoglycosides, and tigecycline. In addition, low resistance levels to tigecycline were noted for ST290 and ST11 strains (5.9% and 0%, respectively) compared with that of ST15 (72.7%), and 13.2% of ST290 strains exhibited quite low resistance rates to aztreonam, one member of the monobactams that could not be hydrolyzed by NDM, a type of metallo-β-lactamase (MBL). 20
The Amounts and Percentages of Distinct Sequence Types of Carbapenem-Resistant Klebsiella pneumoniae Isolates Resistant to Different Antibiotics
The breakpoint of TGC was interpreted by FDA criteria.
FDA, U.S. Food and Drug Administration; IPM, imipenem; ETP, ertapenem; CRO, ceftriaxone; FEP, cefepime; FOX, cefoxitin; CIP, ciprofloxacin; LEV, levofloxacin; GM, gentamicin; AK, amikacin; TOB, tobramycin; ATM, aztreonam; TGC, tigecycline; TZP, piperacillin/tazobactam; R, resistant; ST(-), ST type undetected with blaNDM-5 positive.
Phenotypic and genotypic profiles
A total of 120 (120/133, 90.2%) CRKP isolates were found by mCIM to produce carbapenemases. The addition of testing by eCIM was recommended to detect MBL. Eighty-nine (89/133, 66.9%) and 31 (31/133, 23.3%) carbapenemase-producing isolates were confirmed to be positive for blaNDM-5 and blaKPC-2, respectively. The remaining 13 (13/133, 9.8%) isolates were negative by mCIM, excluding the false-negative results, implying that other intrinsic or acquired mechanisms, such as porin loss or AmpC enzyme hyperproduction, might be responsible for resistance to carbapenems among these isolates.
Genetic relatedness
Homology analysis was carried out to elucidate the genetic relatedness of carbapenem-resistant isolates. MLST revealed that ST290 was the most common sequence type of NDM-5 producers (67/89, 75.3%), followed by ST11 (10/89, 11.2%) and ST15 (10/89, 11.2%).
PFGE revealed seven distinct clusters (cluster A to cluster G), centered on the burn ward, ICU, and EICU. Fifty (50/67, 74.6%) ST290 clones belonging to cluster E were collected from patients on the burn ward, which shed light on the diffusional clonal lineage (Fig. 1). In addition, strains 1083 and 1084 shared the same PFGE profile but across two different STs, as did strains 1068 and 1082. Critically, the relatedness depicted in PFGE demonstrated the evidence for potentially transferable competency of blaNDM-5, which was a suggestive of an association with mobile genetic components.

A dendrogram of PFGE profiles of 94 CRKP isolates. The adjacent information shown on the right represents number of strains, ST type, NDM-5 presence, specimen type, department (Burn: the burn ward; ICU, intensive care unit; EICU, emergency intensive care unit), and cluster, respectively. CRKP, carbapenem-resistant Klebsiella pneumoniae; PFGE, pulsed-field gel electrophoresis.
Plasmid sequence analysis of blaNDM-5
To explore the core principle of transmission, complete sequencing of plasmid possessing blaNDM-5 was carried out after extraction. The plasmid carrying the blaNDM-5 is 49,021 bp in size, and is designated as pNDM5-LDR (GenBank:MK308632). It belongs to the IncX3 group and other than blaNDM-5, the plasmid does not harbor any other resistance genes. blaNDM-5 was located in the downstream of a truncated transposase ISAba125 that was disrupted by the insertion of IS5 with the opposite orientation. There are 51 putative ORFs included within the plasmid (Fig. 2). BLASTN search (GenBank) showed that pNDM5-LDR highly matched with the following plasmids pNDM5_020001, pNDM-HK2998, pNDM-HK3218, and pNDM-HK3473 (99% identity and 94% coverage), identified from E. coli SCEC020001, K. pneumoniae CRE2998, E. coli CRE3218, Enterobacter cloacae CRE3473, respectively. Apart from the plasmid scaffolds typical of IncX3 plasmids, ISKpn19, a sort of IS element, was found inserted particularly into pNDM5-LDR in this study. This kind of element probably enhanced expression of the blaNDM-5 carbapenem-hydrolyzing gene or provided the promoter sequences for blaNDM-5 expression. 21 Thus, the horizontal transmission of blaNDM-5 by IncX3 plasmid highlights the need for extensive attention.
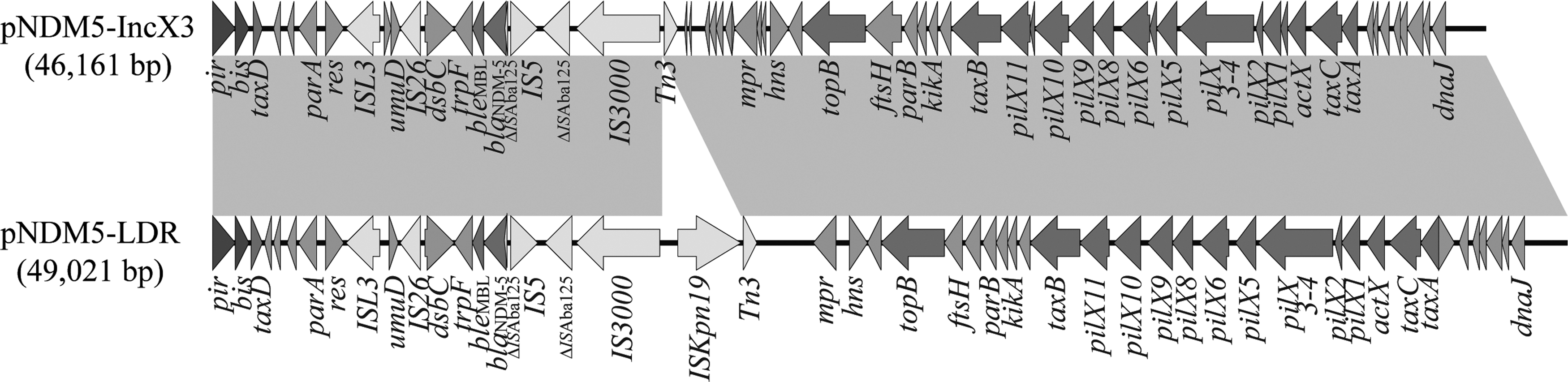
A schematic map of the plasmid structure, including comparison of IncX3 plasmid pNDM5-LDR and representative plasmid pNDM5-IncX3. ORFs are indicated by arrows. Sequences of shared homology between two plasmids are marked by gray shading. Different arrows are representative of replicons, plasmid backbone genes, mobile elements, the resistant gene, and plasmid transfer genes. ORF, open reading frame.
Discussion
To our knowledge, this is the first study to describe the transmission of this particular K. pneumoniae ST290 clone. Although blaNDM-5 has been identified in K. pneumoniae isolates involving ST147, ST709, ST45, ST14, and ST16 types in several countries such as the Netherlands, the Middle East, China, Japan, and Korea,22–26 there are only two reports that blaNDM-5-harboring K. pneumoniae ST2266 and ST16 were considered to be possible transmission events in New Zealand and Denmark, respectively.27,28 As shown in the literature, K. pneumoniae ST11-producing KPC-2-type carbapenemase is a dominant epidemic clone in China. 5 However, in this study, blaNDM-5-harboring K. pneumoniae ST290 was the predominant clone. Moreover, little data are available for sequence type 290 (ST290) in humans. Only one CRKP isolate of ST290 all over the world was isolated from patients in a neonatal unit, 29 but expressing blaNDM-1. Our study is the first report of transmission of blaNDM-5-harboring K. pneumoniae belonging to ST290.
ST290 was the endemic clonal lineage carrying blaNDM-5 in the burn ward at this center, whereas ST11 occurred mainly in other departments such as in the ICU. It was also observed that there were several isolates of ST290 that were blaNDM-5 negative; this was also found in the burn ward (Table 2). We speculated that this specific strain could differ from the other ST290 clones at a genetic level or some minor mutations might act on the bacteria in the course of evolution. Similarly, although it shows the excellent concordance between PFGE and MLST, occasional “discrepancies” remain, we suspected that this rare event could be the result of intergenomic recombination involving the loci detected or insertion/deletion of different mobile genetic elements.
The Primary Distribution of Distinct Sequence Types Harboring blaNDM-5
Two isolates were positive for blaNDM-5, of which STs could not be detected (unlisted in the table).
ICU, intensive care unit; EICU, emergency intensive care unit; ST, sequence type.
In the setting of the burn ward, in which patients are seriously vulnerable to infection, with an impaired skin barrier and multiple invasive procedures such as mechanical ventilation, the risk of hospital-associated infections caused by multidrug-resistant bacteria increases sharply. The wide use of carbapenems as the last-line therapeutic choice for severe infections might contribute to this new outbreak of clonal spread carrying the carbapenemase gene blaNDM-5.
Conclusion
This study describes the first outbreak of blaNDM-5-harboring K. pneumoniae ST290 in China. The epidemiology of Class B carbapenemases like NDM in local regions should be monitored closely to detect early indications of this emerging threat to public health.
Ethics Statement
The Ethics Committee of Hwa Mei Hospital, University of Chinese Academy of Sciences exempted this research for review because the study focused on bacteria.
Footnotes
Acknowledgments
The authors thank their colleagues from the first affiliated hospital of Wenzhou Medical University for participating in the whole research and the excellent technical assistance provided by Liang Chen. The authors also express their gratitude to the editors of the Journal and suggested reviewers for reading the article and the comments.
Disclosure Statement
No competing financial interests exist.