
Abstract
Carbapenemases play important roles in conferring resistance to beta-lactam antibiotics, including the carbapenems. Detection of carbapenemase activity helps to understand the possible mechanism(s) of carbapenem resistance. Identification of carbapenemases is currently being done by various phenotypic methods and molecular methods. However, innovative biochemical and spectrophotometric methods are desirable as they will be easy to perform, affordable, and rapid. A novel chromogenic method called Carba NP test was introduced recently to screen for carbapenemases in clinical isolates of gram-negative pathogens. We adopted this assay (1) to detect the total carbapenemase activity, (2) to discriminate Class A, B, and D carbapenemases with inhibitors, (3) to compare with carbapenemase genotype, and (4) for direct differential diagnosis of carbapenemases in uncultured clinical sample such as tracheal aspirate. The study included 132 purulent tracheal aspirates. All samples were processed and screened by a protocol optimized in our laboratory, which showed good sensitivity and correlation with genotyping and conventional phenotyping. Our protocol not only offers the fastest way to identify the pathogen but also its carbapenemase profile, directly from uncultured clinical samples in less than 4 hr. Our protocol is currently being validated on other types of clinical specimens in our laboratory.
Introduction
The emergence of multidrug resistance (MDR) among gram-negative pathogens is severely hampering the management of infections in the hospitals as well as in the community. Carbapenemases hydrolyze all beta-lactam antibiotics, including carbapenems, and considered an important trait to identify carbapenem resistance in clinical isolates.1,2 Carbapenemase profiling of pathogenic gram-negative bacteria also helps in molecular epidemiology. Laboratory detection of carbapenemase producers has become more challenging due to the emergence of diverse carbapenemases.3,4 Rapid detection and carbapenem sensitivity profiling of these pathogens have become imperative for successful management of infections and also to control dissemination. Antimicrobial susceptibility tests are usually performed on agar plates or in automated systems in a clinical microbiology laboratory. Carbapenemases are not the sole cause of resistance, other mechanisms such as porin loss or increased efflux pump activity in the bacterial membrane may also influence sensitivity to carbapenems.5–8 Therefore, a definite method is required to distinguish enzymatic and nonenzymatic resistance mechanisms for effective management of infection control and epidemic outbreaks.2,9 Phenotypic methods such as the modified Hodge test (MHT) and disk diffusion tests with inhibitors are commonly used in the microbiology laboratory to test the carbapenemase activity of isolated bacterial cultures. However, these methods show lower specificity and sensitivity compared with molecular methods. 10 Identification of the resistance gene is considered the gold standard for confirmation of drug resistance, although economically and technically beyond the reach for many clinical laboratories.3,5 Thus, there has been an unmet need for a simple, affordable, and yet direct demonstration of carbapenemase activity in any given bacterial pathogen. To fill this important gap, the Nordmann group designed and developed a novel yet simple phenotypic method called Carba NP test, for rapid detection of carbapenemases in Enterobacteriaceae. 2 This phenotypic assay is based on a change in pH caused due to hydrolysis of imipenem by carbapenemase present in the cell-free bacterial lysate. Phenol red is used as an indicator to monitor this change in pH, which turns from red (alkaline) to yellow (acid).2,3,11,12 This test has become a boon for rapid identification of carbapenemase activity in gram-negative bacterial pathogens, considering the difficulties in the interpretation of results and false positivity with various other phenotypic methods. Carba NP is a huge improvement over other phenotypic methods with almost 100% sensitivity and its specificity is comparable with molecular methods. 2 Several modifications have been made to this assay to improve its performance characteristics and avoid false negatives.10,13,14 Three major classes of carbapenemases have been reported in gram-negative pathogens. They are grouped according to their amino acid composition and identity. 15 Based on the action of beta-lactamase inhibitors (tazobactam, clavulanic acid, and divalent chelator such as ethylene diamine tetra acetic acid disodium salt [EDTA] and NaCl), Carba NP assay has been modified to identify different classes of carbapenemases in gram-negative bacterial isolates. 12 Later, the “Blue-Carba” test was designed using bromothymol blue as an indicator for direct colony approach. 16 Originally, Carba NP assay was used for members of Enterobacteriaceae isolates, later it was applied to isolates of Acinetobacter sp. with minor changes in inoculum size and lysis conditions. 17 Yet, Carba NP assay has not yet been demonstrated for direct detection of carbapenemase activity in uncultured clinical specimens such as body fluids.
The main objective of this study was to adopt and evaluate the Carba NP assay for the rapid identification and differentiation of carbapenemases on uncultured clinical specimens thus making the result available to the clinician on the same day, for quick therapeutic decisions to be made. In this study, we made some modifications in sample processing and assay protocols. In addition, we validated our protocol directly on uncultured tracheal aspirates also. We included specific inhibitors for differentiating carbapenemases belonging to Class A, B, and D. We monitored the enzyme activity over a period of 2 hr. Eventually, we used a 30-min incubation to measure the carbapenemase activity in all the clinical isolates and uncultured clinical samples as maximum rate of hydrolysis occurred during this period. We believe that these modifications simplify the assay for direct application to clinical samples. The results of the Carba NP test were compared with “carbapenemase” genotyping, phenotyping by VITEK-2, and analyzed for sensitivity and specificity.
Materials and Methods
The study included 132 purulent tracheal aspirates. The tracheal aspirates were the leftover samples provided by the clinical microbiology laboratory of a tertiary care hospital in Hyderabad. After the tracheal aspirates were processed for culture, the remaining fluids of the tracheal aspirates were used in this study. Therefore, these specimens were not collected exclusively for this study. Furthermore, no intervention was done using the results nor was any change in therapy recommended to the clinicians by the investigators. Routine clinical microbiology data related to the species and drug sensitivity (VITEK-2) were blinded and were decoded only after the genotyping and Carba NP analysis were completed.
Preparation of genomic DNA for genotyping
One hundred fifty microliters of tracheal sample was centrifuged at 5,000 rpm for 10 min and the pellet was suspended in 100 μL of TEX buffer (10 mM Tris-HCl pH 8.5, 1 mM EDTA, 1% [w/v] Triton X-100). The suspension was vortexed to achieve a uniform suspension and centrifuged again at 5,000 rpm for 5 min and this wash was repeated once. Finally, the pellet was resuspended without any clumps in 100 μL of TEX buffer and lysed by heating in a dry bath at 95°C for 15 min. 18 The lysate was centrifuged (5,000 rpm) and the supernatant was used as the DNA template for PCR amplifications. Species identification of Acinetobacter baumannii was done by amplification of 16S–23S rRNA intergenic spacer region (Ab-ITS). Carbapenemase genotyping for blaKPC-2, blaNDM-1, blaOXA-23-like, and blaOXA-51-like was done as described earlier19–22 and the primers used are listed in Table 1. The target gene sequences of Ab-ITS, blaOXA-23-like, and blaOXA-51-like were amplified by multiplex PCR under the following conditions: initial denaturation at 95°C for 10 min, followed by 35 cycles at 94°C for 30 sec, 50°C for 40 sec, and 72°C for 50 sec, and a final extension at 72°C for 5 min. Class B carbapenemase blaNDM-1 was identified after thermocycling under the following conditions: initial denaturation at 95°C for 10 min, followed by 35 cycles of 94°C for 30 sec, 58°C for 40 sec, and 72°C for 50 sec. Class A carbapenemase blaKPC-2 was identified after PCR under the following conditions: initial denaturation at 95°C for 10 min, followed by 35 cycles of 94°C for 30 sec, 55°C for 30 sec, and 72°C for 50 sec. A final extension at 72°C for 10 min was allowed for these two gene targets after the thermocycling. The amplicons were resolved in 2% agarose by electrophoresis and visualized after staining with ethidium bromide for the following amplicons: 501 bp (blaOXA-51-like), 353 bp (blaOXA-23-like), 208 bp (Ab-ITS), 660 bp (blaNDM-1), and 489 bp (blaKPC-2).
Primers Used for Acinetobacter baumannii Species Identification and Carbapenemase Genotyping
Primers used in multiplex PCR to identify A. baumannii species and to screen for various carbapenemase genes.
F, forward primer; KPC, Klebsiella pneumonia carbapenemase; R, reverse primer.
Carba NP assay
The Carba NP assay 12 was performed as described below with some modifications to the original protocol. Tracheal aspirates were processed as follows (Fig. 1): 150 μL of the tracheal aspirate was taken into a 1.5 mL microcentrifuge tube and centrifuged at 10,000 rpm for 5 min. The supernatant was discarded, the pellet was resuspended uniformly in 100 μL of TX buffer by vortex, centrifuged at 5,000 rpm, and this process was repeated twice. The clear colorless pellet was uniformly resuspended in 100 μL of TX lysis buffer (10 mM Tris-HCl pH8.5 and 1% Triton X-100) without any clumps and subjected to vortex in pulses of 30 sec for 2 min, incubated at 37°C for 1 hr for maximum lysis of bacteria, and centrifuged for 5 min at 10,000 rpm. The cell-free supernatant was used for the Carba NP assay. The assay was performed in 96-well microtiter plates. Thirty microliters of cell-free supernatant was mixed with 100 μL of 0.01 mM imipenem, 40 μL of 0.1 mM ZnSO4, and 30 μL of phenol red (0.5% w/v) indicator (pH = 8.5), making the total volume to 200 μL in each well. Five microliters of 3 mM of (EDTA for metallo β-lactamases [MBL]) or 1 μL of 0.06 mM of phenyl boronic acid (PBA for Class A enzymes) or 1 μL of 100 mM of NaCl (for Class D enzymes) was added based on which enzyme was being assayed and the microtiter plate was incubated at 37°C. Rate of hydrolysis was monitored at A546nm and at different time periods of 0, 15, 30, 60, and 120 min. Absorbance values at 30 min were taken into consideration for all subsequent screenings by Carba NP, as maximum hydrolysis by Class A and B enzymes occurs at 30 min. Carbapenemase activity changes the color of phenol red to yellow. Specificity of the Carba NP assay was validated on type strains of Escherichia coli (NCTC 11954), Pseudomonas aeruginosa (NCTC 13437), Klebsiella pneumonia (ATCC BAA-1705, ATCC BAA-2146), and A. baumannii (ATCC 17978+ OXA-23 clone) strains as positive controls and on Staphylococcus aureus (ATCC 25923, ATCC 43300) strains as negative control. The assay mixture contained buffered cell-free extract from these type strains, imipenem, and ZnSO4. When incubated at 37°C, the reaction mixture turned from red to orange or yellow depending on the extent of enzyme activity or remained red if bacterial cell-free extracts did not contain any carbapenemase activity.

Flow diagram for processing of tracheal samples. Color images are available online.
Statistical analyses
All the statistical analyses were performed by MedCalc, Ostend, Belgium; (MedCalc Statistical Software version 15.6.1).
Results
Carbapenemase detection
A total of 132 purulent tracheal aspirates were directly processed for genotyping and Carba NP test. The phenotypic (VITEK-2) data were blinded to us. We screened them initially for the A. baumannii species-specific genetic marker (Ab-ITS), and all positive samples were subjected to carbapenemase genotyping by PCR. Of the 132 purulent tracheal aspirate samples, 103 (78%) samples were positive for Ab-ITS amplicon and hence presumed to be A. baumannii. When we evaluated the performance of the genetic marker Ab-ITS against the reference method VITEK-2, 47(47/103) tracheal aspirates were positive by both PCR and VITEK-2, whereas 56 samples were “false positive” by PCR genotyping as they were not corroborated by VITEK-2. Thus, Ab-ITS PCR showed greater sensitivity (100%) and a negative predictive value of 100% although the specificity (34.12%) was moderate compared with VITEK-2 for identification of A. baumannii (Fig. 2). Carbapenemase genotyping showed blaOXA-51 in 90.29% (93/103) and blaOXA-23 like in 53.3% (55/103) of the clinical samples. blaKPC-2 was detected in 38 samples (38/103, 36.8%) and blaNDM-1 was detected in 49 samples (49/103, 47.5%). The remaining 29 (29/103, 21.9%) Ab-ITS-negative tracheal samples were also genotyped for carbapenemases: 9 (9/29, 31%) contained blaOXA-51 like, 1 sample contained blaOXA-23 like (1/29, 3.4%), 14 (48.2%) showed blaKPC-2, and 10 (10/29, 34.4%) harbored blaNDM-1. We observed that our assay could not detect OXA-23 activity in four samples compared with the genotyping (blaOXA-23 like). Genotypic and phenotypic results of Ab-ITS-positive samples are presented in Table 2 and the carbapenemase genotypes are represented in Fig. 3.
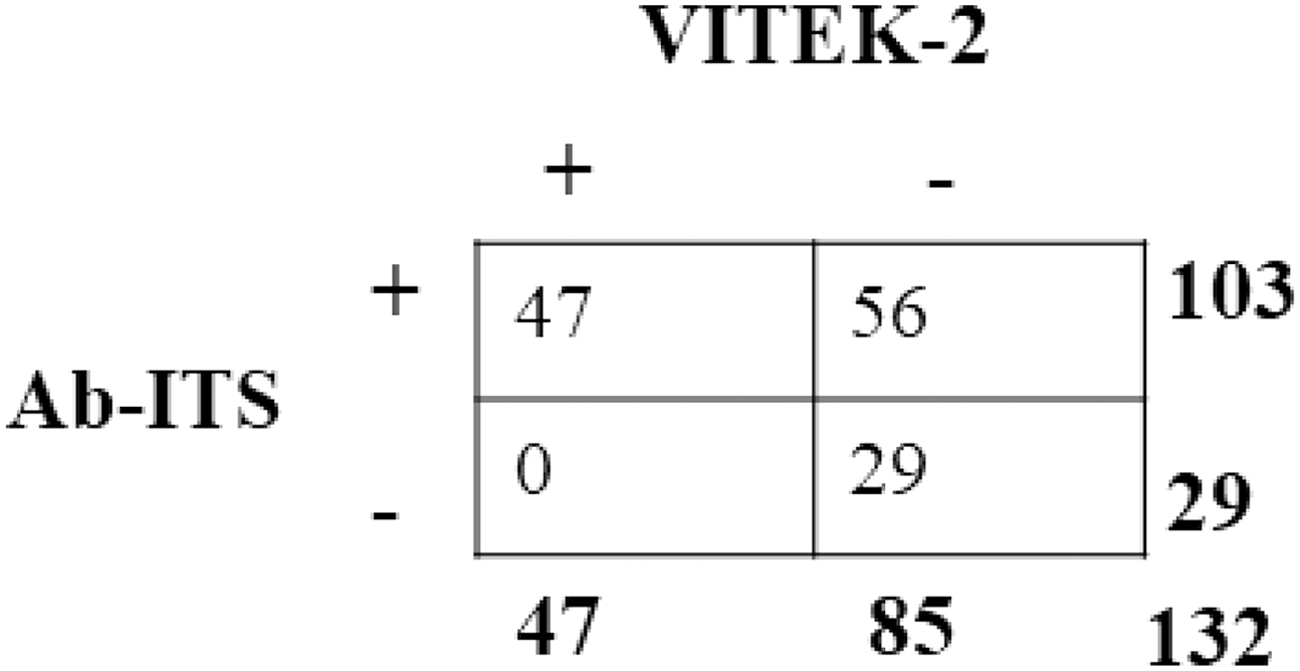
Comparison of species-specific genetic marker (Ab-ITS) versus VITEK-2 in tracheal aspirates. The Ab-ITS PCR had 100% sensitivity, 34.12% specificity, with a PPV of 45.63%, and 100% negative predictive value (MedCalc Statistical Software version 15.6.1). PPV, positive predictive value.
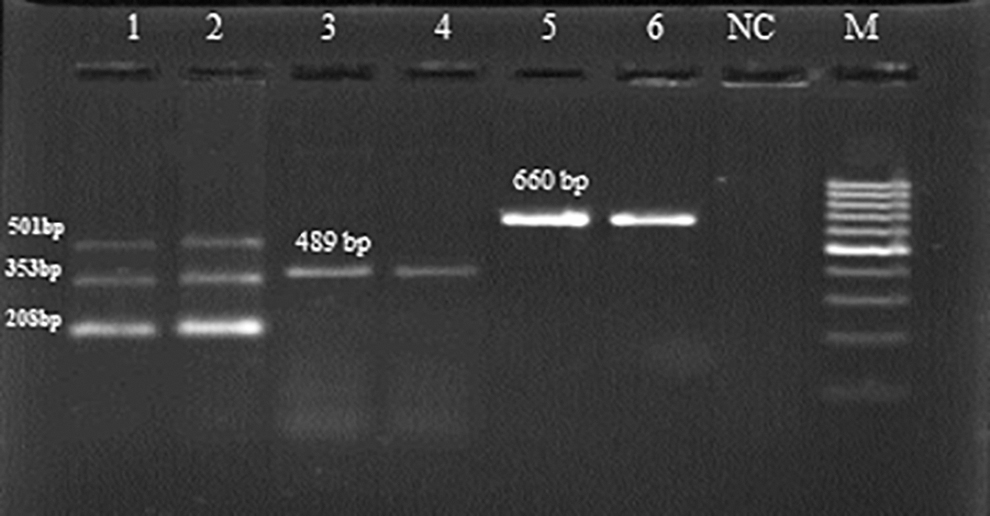
Agarose gel analysis of carbapenemase genotypes. Lane M—molecular marker (100 to 1,000 bp), Lane 1—positive control ATCC 17978+ OXA-23 clone (Triplex PCR Ab-ITS, blaOXA-51 like, blaOXA-23 like), Lane 2—tracheal aspirate positive for Triplex PCR, Lane 3—positive control ATCC BAA-1705 (blaKPC-2), Lane 4—tracheal aspirate positive for blaKPC-2, Lane 5—positive control ATCC BAA-2146 (blaNDM-1), Lane 6—tracheal aspirate positive for blaNDM-1, Lane NC—no DNA target control.
Correlation of Carba NP Results and Carbapenemase Genotypes of Tracheal Aspirates
Of 103 tracheal aspirates included in this analysis, 10 samples were negative for carbapenemase genotype.
Class D oxacillinase genes.
KPC gene of Class A.
New Delhi metallo beta-lactamase gene of Class B.
Both Class A and Class B genes.
Both Class D and Class B genes.
Both Class D and Class A genes.
Class A, Class B, and Class D genes.
The numbers in the columns on the right represent samples positive for the indicated carbapenemase gene(s).
The columns in this row represent the number of samples that tested positive for the particular Carba NP activity.
Specific inhibitor: PBA for blaKPC-2, EDTA for blaNDM-1, NaCl for blaOXA-51 and blaOXA-23
Four tracheal samples did not show measurable Carba NP (OXA-23) inhibition with NaCl and another four samples did not show any combined activity of blaOXA-23-like, blaNDM-1, and blaKPC-2.
PBA, phenyl boronic acid.
Validation of Carba NP assay
Our Carba NP test results showed absolute correlation to our carbapenemase genotype results. Initially, the rate of hydrolysis of imipenem was monitored for 2 h at different intervals, that is, 0, 15, 30, 60, and 120 min with and without the appropriate carbapenemase inhibitor. EDTA (3 mM) was used as inhibitor for Class B (MBL) carbapenemases, NaCl for Class D (oxacillinases [OXA]), and PBA was used as specific inhibitor of Class A type (K. pneumonia carbapenemase [KPC]) enzymes. Carba NP assay results (Table 3) were interpreted as follows: (1) if the color turned from red to orange or yellow in the presence of EDTA and 100 mM of NaCl, whereas wells containing PBA remained red in color, the isolate carried Class A enzyme group (represented by KPC in this study); (2) if the color in the wells turned from red to orange or yellow in the presence of PBA and 100 mM of NaCl, whereas wells containing EDTA remained red in color, the isolate was MBL producer belonging to Class B (represented by NDM-1 in this study); (3) if the color in the wells turned from red to orange or yellow in the presence of PBA and EDTA, whereas wells containing NaCl remained red, the isolate was oxacillinase producer belonging to Class D (represented by OXA-51 and OXA-23 in this study); and (4) if the color of the wells remained red under all the above conditions, the isolate was considered a noncarbapenemase producer. Assay results were categorized based on the genotypes as reference in four different ways such as: all positive (Group I), Class D positive and others negative (Group II), Class B negative and others positive (Group III), and Class A negative and others positive (Group IV). For screening of carbapenemase activity and to determine the carbapenemase profile in the tracheal aspirates, endpoint for the assay was kept as 30 min at 37°C as default and the absorbance measured at 546 nm as maximum rate of hydrolysis was seen in 30 min. Carba NP results of all four groups were noted as A546 and are presented in Fig. 4.

Profiling of carbapenemases of Acinetobacter baumannii from tracheal aspirates. Inhibition profile of carbapenemases of A. baumannii from tracheal aspirates. The effect of inhibitors (control, EDTA, PBA, and NaCl) on carbapenemase activity in tracheal aspirates was determined as follows. The cell-free supernatant was incubated at 37°C without (control) and with different inhibitors (test) for 0–2 hr and the color change was monitored at 546 nm at 0, 15, 30, 60, and 120 min and grouped as Group I: blaKPC-2 (+), blaNDM-1(+) and blaOXA-51 like(+), blaOXA-23 like (+); Group II: blaKPC-2 (−) and blaNDM-1 (−) but blaOXA-51 like and blaOXA-23 like (+); Group III: blaKPC-2 (+) and blaOXA-51 like, blaOXA-23 like (+) but blaNDM-1 (−); and Group IV: blaNDM-1 (+) and blaOXA-51 like, blaOXA-23 like (+) but blaKPC-2 (−).The error bars represent standard deviation of mean of A546nm from three separate experiments for each group. EDTA, ethylene diamine tetra acetic acid disodium salt; PBA, phenyl boronic acid. Color images are available online.
Modified Carba NP Test and Interpretation of Results with Inhibitors to Discriminate Different Classes of Carbapenemases
Cell-free extracts obtained from tracheal aspirates were assayed for carbapenemase activity as described under the Materials and Methods section over a period of 0–2 hr with appropriate inhibitors and the change in absorbance was recorded at 546 nm.
EDTA, ethylenediaminetetraacetic acid.
A total of 132 tracheal aspirates were included in this study. Phenotypic data of these clinical samples were blinded to our laboratory and the results were decoded after genotyping and Carba NP assays. Those samples identified as A. baumannii (n = 103) were separated from those that were not A. baumannii (n = 29). All samples were processed as described earlier. Results of carbapenemase genotyping and Carba NP assay of A. baumannii-positive tracheal aspirates (n = 103) were compared with VITEK-2 results for statistical analysis. Eighty-five samples were positive for both Carba NP and carbapenemase PCR, whereas eight samples were carbapenemase PCR positive but did not show any carbapenemase activity. Sensitivity (91.4%), specificity (100%), positive predictive value (PPV, 100%), and negative predictive value (55.5%) were calculated and are presented (Fig. 5). Twenty-nine of the 132 samples (29/132), which were negative by Ab-ITS PCR, were investigated separately to characterize the carbapenemase genotype and carbapenemase by Carba NP. Of these, 12 (12/29) samples showed good correlation between genotype and Carba NP assays. The sensitivity (100%) and specificity (94.12%) data from those 29 samples that did not contain A. baumannii are presented separately (Fig. 6). Carba NP assay when compared with carbapenemase phenotyping in tracheal aspirates showed good correlation. The Carba NP assay had 100% sensitivity, 36% specificity, with a PPV of 62.3%, and 100% negative predictive value. Thirty-two samples were (“false”) positive in Carba NP, but they were negative in VITEK-2. This apparently is due to the superior sensitivity of Carba NP assay over that of VITEK-2's carbapenemase assay (Fig. 7) as these 32 samples were confirmed to be positive for carbapenemase genotypes.
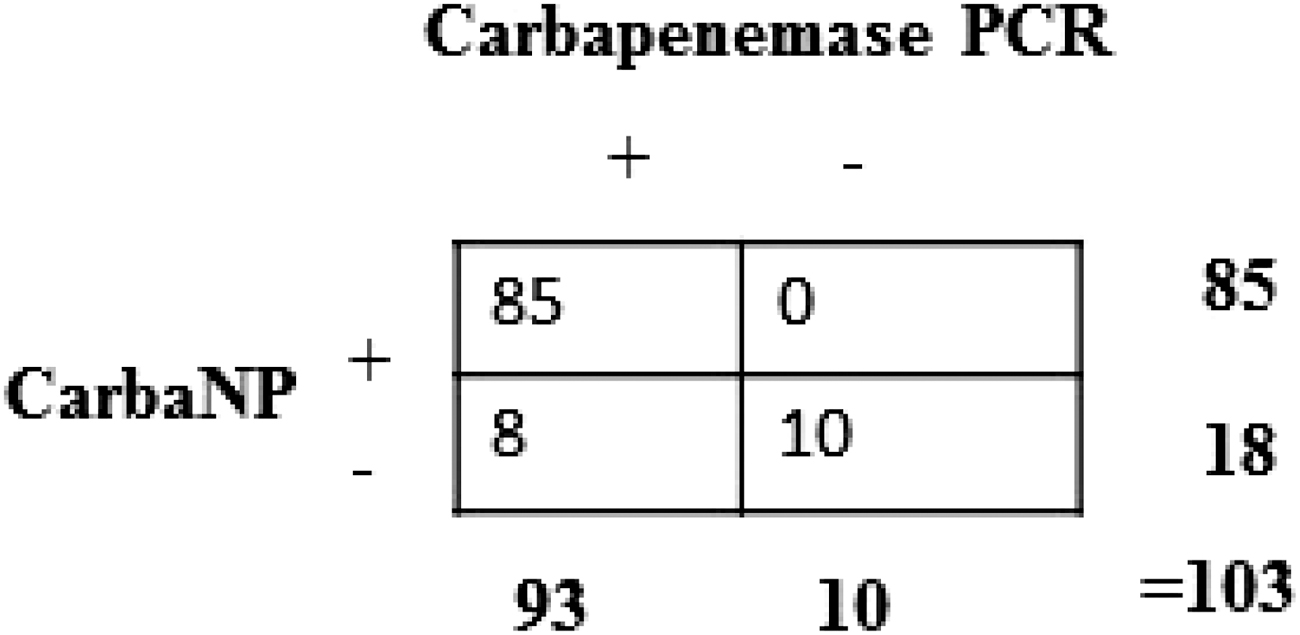
Comparison of Carba NP assay versus carbapenemase genotyping in tracheal aspirates containing A. baumannii (Ab-ITS positive). The Carba NP assay had 91.4% sensitivity, 100% specificity, with a PPV of 100% and 55.5% negative predictive value (MedCalc Statistical Software version 15.6.1). This analysis considered only the Ab-ITS-positive samples (103/132) and 29 samples were Ab-ITS negative.
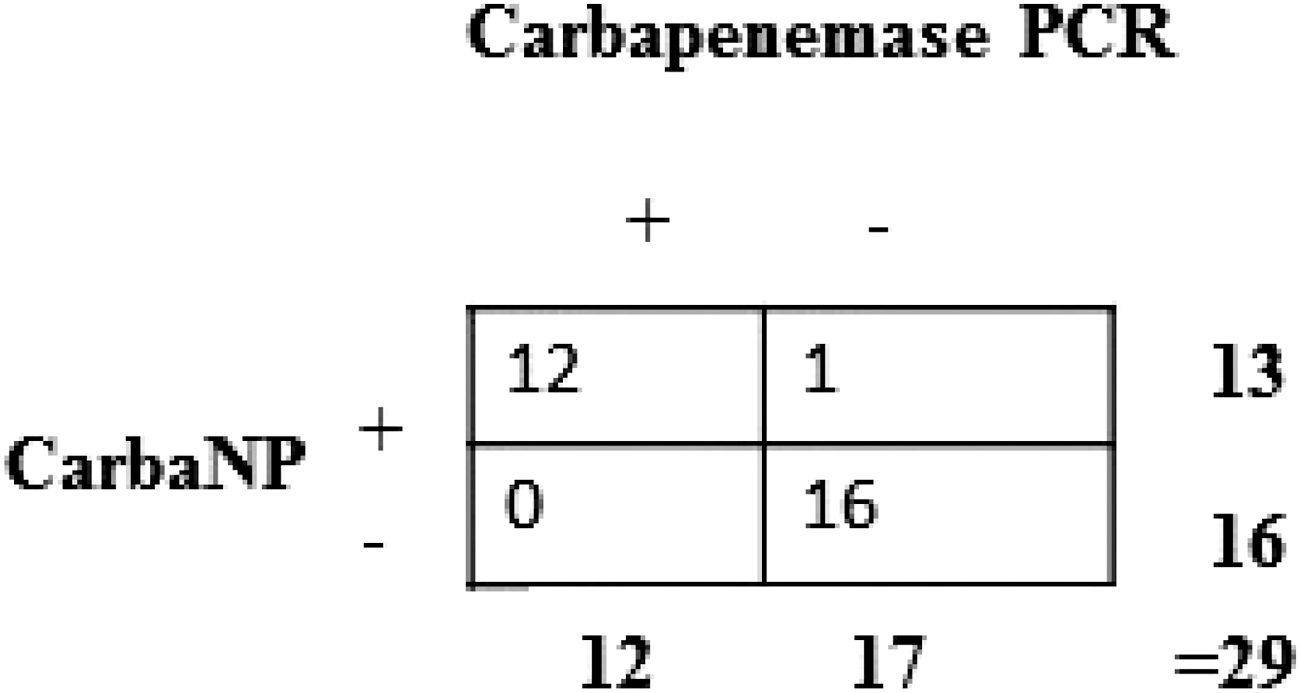
Comparison of Carba NP assay versus carbapenemase genotyping by PCR in tracheal aspirates not containing A. baumannii (Ab-ITS negative). The Carba NP assay had 100% sensitivity, 94.12% specificity, with a PPV of 92.31% and 100% negative predictive value (MedCalc Statistical Software version 15.6.1).This analysis included only the Ab-ITS-positive samples (103/132) and did not include 29 samples that were Ab-ITS negative.
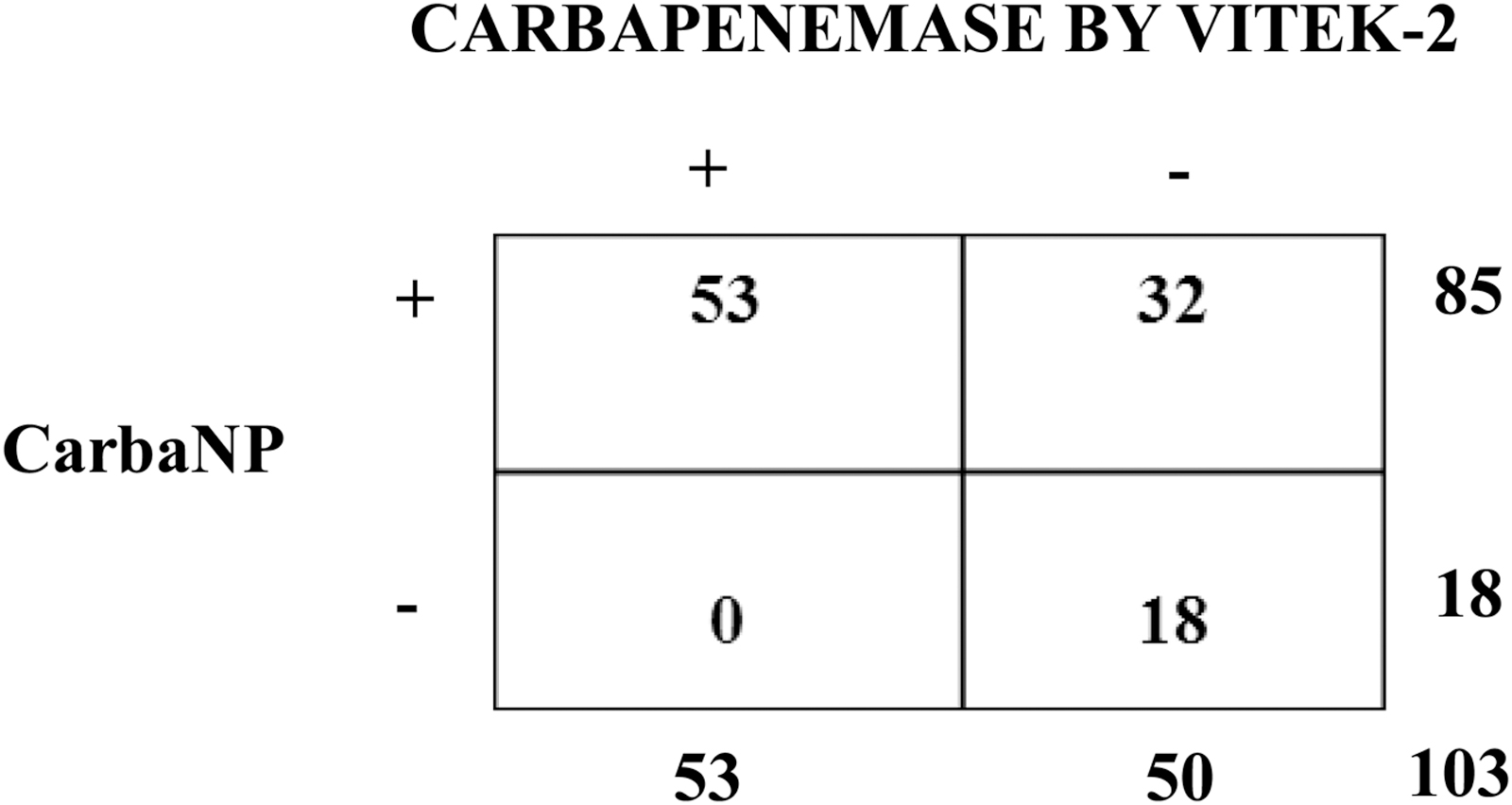
Comparison of Carba NP assay versus carbapenemase phenotyping by VITEK-2 in tracheal aspirates containing A. baumannii (Ab-ITS positive). The Carba NP assay had 100% sensitivity, 36% specificity, with a PPV of 62.3% and 100% negative predictive value. This analysis considered only the Ab-ITS-positive samples (103/132) and 29 samples were Ab-ITS negative.
Discussion
Carbapenemase activity is an important attribute of drug resistance in gram-negative bacteria. The massive dissemination of carbapenemase producers among Enterobacteriaceae demands that methods quickly determine the microbial species and also that the drug sensitivity profile should be made available in the microbiology laboratory. High sensitivity and specificity together with a rapid workflow have become mandatory to devise therapeutic strategies to treat dangerous pathogens and to control their spread.11,12 Application of Carba NP in this study shows that it is capable of rapidly detecting different carbapenemases in gram-negative pathogens and allows to make distinction between enzymatic and nonenzymatic mechanisms of carbapenem resistance. The adaptation of Carba NP method showed multiple advantages over the other phenotypic screening methods. Carba NP has high sensitivity, specificity and is easily available for prompt identification of carbapenemases.11,23 The original Carba NP test was validated on clinical isolates of various enterobacterial species and subsequently on clinical isolates of A. baumannii.2,17 Recently, the assay was adopted to detect “carbapenemase” activity in spiked blood cultures. 24 This method eliminates false positives compared with boronic acid synergy test, the MHT, and drastically reduces time compared with the disc diffusion/E-test methods.25,26 The carbapenem inactivation method (CIM), and the modified CIM reported recently require at least 24–72 hr for results even though it is economical.5,27 Rapidec Carba NP test kit (BioMérieux, France), Neo-Rapid Carb screen kit, and Rapid Carb Blue screen (ROSCO Diagnostics Denmark) are commercial kits available for screening clinical isolates for carbapenemase activity.14,28,29 MALDI-TOF MS is an effective method compared with the Rapidec Carba NP test kit to discriminate between carbapenemase and noncarbapenemase producers.30,31 As an alternative to molecular assay, antibody-based methods such as lateral flow immunoassay have been developed for detection of carbapenemases. Lateral flow assays yield results from cultured isolates within 15 min with 100% sensitivity and specificity.32,33 The manual versions of rapid colorimetric assays include manual Carba NP CLSI method, manual Blue Carba, and modified Carba NP, requiring reagent preparation compared with ready-to-use kit methods.16,29,34 These Carba NP tests available till date help to reduce the time taken to identify carbapenemase activity in clinical isolates. However, the full potential of the test could be realized only when the test is applicable directly to uncultured clinical samples so that therapeutic decisions can be made quickly. We attempted to fulfill this gap. We have simplified the cell-free extract preparation and validated it directly on purulent tracheal aspirates to detect, quantitate, and also differentially demonstrate various carbapenemase activities using specific inhibitors. Remarkable correlation was observed in our study between the genotypic test results (PCR) and Carba NP assay results. Carba NP assay showed good sensitivity (91.4%) and specificity (100%) when it was applied directly to uncultured tracheal aspirate samples in this study. One observation made in this study is the relatively lower sensitivity of our Carba NP test to detect blaOXA-23 like (20/24) phenotype. We presume this could be due to poor expression of the blaOXA-23 like gene in these isolates and this would be investigated separately. This probably will impact the results of Carba NP test if the isolates contain only blaOXA-23like as the Carba NP test would not detect them. These “false-negative” results could be resolved by a qRT-PCR of the blaOXA-23 like transcript. The Carba NP method greatly reduces cost and labor with excellent accuracy in results even with uncultured tracheal aspirates. The convenience of Carba NP test is notable as it does not require any specialized equipment and needs a short hands-on time to perform and requires only a single colony from the agar plate or 150 μL of the tracheal aspirate. It is easily scalable to a high-throughput format for a large number of gram-negative isolates and adaptable in any laboratory. The low cost of reagents used in this study (<1 US $ per sample) compared with most of the commercially available kits 35 (@ US $ 2.4–8.6 per sample) makes them economically viable even in resource-poor countries. Advantages of our Carba NP assay are highlighted in a comparison of the characteristics of our Carba NP assay with other assays (Table 4).
Characteristics of Our Assay Versus Other Carba NP Assays
ACB, Acinetobacter calcoaceticus-baumannii complex; BCT, β Carba test; BYG, BYG Carba test; CIM, carbapenem inactivation method; mCIM, modified carbapenem inactivation method; NRCK, Neo-Rapid Carb screen kit; RCNP, Rapidec Carba NP.
Our assay can be used for rapid differential diagnosis of carbapenemases directly in clinical samples. Blindfolding the tracheal aspirate (n = 132) samples for the genotyping/Carba NP screening by the microbiology laboratory shows that our Carba NP test format is applicable and adaptable as a routine in a clinical microbiology laboratory. Remarkable correlation between genotyping and Carba NP test results shows that this colorimetric assay is reliable and accurate. We fixed 30 min as endpoint for all Carba NP screening assays as maximum hydrolysis was completed by this time. Inclusion of inhibitors seems to be an attractive option to narrow down the drug sensitivity profile compared with expensive, time-consuming disc diffusion or E-test. In tracheal aspirates, Class D enzymes (blaOXA-23 like and blaOXA-51like), Class B (blaNDM-1), and Class A (blaKPC-2) were screened to correlate with phenotyping results along with species identification. The data from these genotypings were used to evaluate the merit of the Carba NP test for differentiating various classes of carbapenemases. We introduced certain modifications to Nordmann's protocol 2 to make it more user-friendly and to apply it directly to uncultured tracheal aspirates. These modifications include the following: (1) the extraction buffer, that is, TX buffer (10 mM Tris-HCl pH 8.5, Triton X-100, 1% w/v) used for bacterial cell lysis, (2) extraction was performed by vigorous pulse vortexing and incubation at 37°C for 1 hr for cell lysis, and (3) rate of imipenem hydrolysis was monitored at 546 nm for different time periods: 0, 15, 30, 60, and 120 min and we found that maximum hydrolysis occurred in the first 30 min. This assay clearly differentiated various classes of carbapenemases in uncultured clinical samples. It is possible that our method could have picked up carbapenemase activity from gram-negative bacteria other than A. baumannii.
As we wanted to study carbapenemase activity of only A. baumannii, we calculated the sensitivity and specificity of our assay only on those tracheal aspirates that were confirmed by Ab-ITS PCR. The sensitivity and specificity of this assay were found to be remarkable when compared with VITEK-2: a sensitivity of 100%, a specificity of 36%, with a PPV of 62.3%, and a negative predictive value of 100% (Fig. 7). The apparently poor specificity and PPV of our Carba NP assay are due to the “false-positive” samples (32/103) that were reported as “polymicrobial gram-negative” and ignored as they contained other gram-negative bacteria by the Advanced Expert System of VITEK-2. This may be a limitation of the Advanced Expert System of VITEK-2. When we recalculate after excluding these polymicrobial samples, the sensitivity (100%) and specificity (100%) become absolute in comparison with VITEK-2 results. The validation and corroboration of our Carba NP assay essentially come from the carbapenemase genotyping results. We are validating our protocol on other types of clinical samples currently and also for other gram-negative pathogens. Our assay could also play an important role in characterization of isolates and monitoring their spread. This Carba NP test offers an economical and faster way to profile the carbapenemases in uncultured tracheal aspirates than even molecular techniques. We hope it will become a valuable and useful tool in clinical microbiology screening and to study the epidemiology of carbapenemase producers. 12
Conclusion
We propose the following algorithm to screen uncultured clinical samples directly for carbapenemase activity
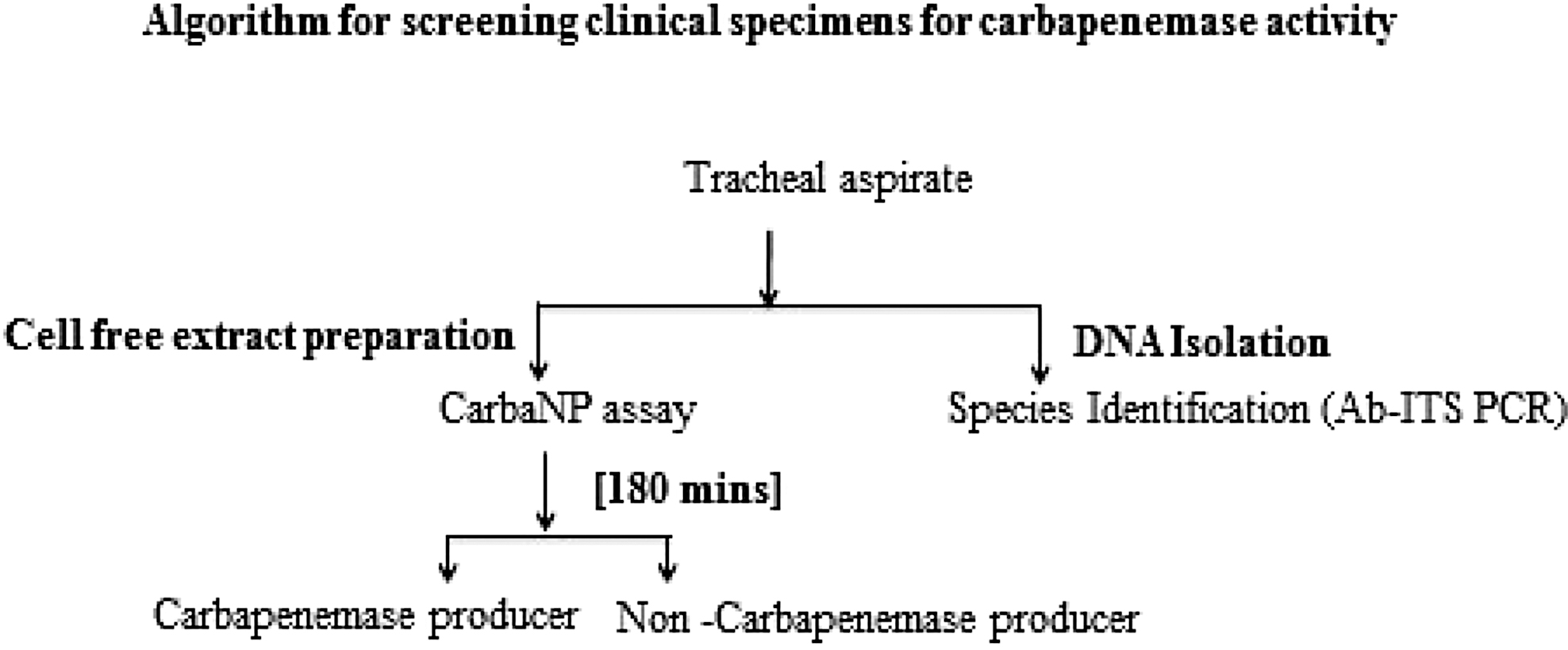
This algorithm (the assay time would be only 30 min for quick screening of total carbapenemase activity) will enable quick identification of carbapenemases for proper infection control measures. The conventional microbiology results are made available in 3–4 days for species identification and drug sensitivity profile. Our protocol, which includes a simple one-step PCR for species identification and Carba NP test for determination of carbapenemase activity, promises to make the same information available to the clinician precisely in less than 4 hr. This is potentially a remarkable improvement and it is hoped that this will revolutionize the way MDR will be identified and used for the management of patients and to control its spread in the society.
Footnotes
Acknowledgment
We gratefully acknowledge the Clinical Microbiology Department at Gleneagles Global Hospitals for providing the clinical isolates as required.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was fully supported by Global Medical Education Research and Foundation (GMERF), Hyderabad, as part of the graduate studies of Swathi CH and did not receive research grants from any funding agency.