
Abstract
Objective:
Optimal dosing regimens for achieving a positive clinical outcome were simulated for seven antibiotics commonly used to treat bloodstream infections (BSIs) in adults.
Methods and Results:
Pharmacokinetic/pharmacodynamic (PK/PD) modeling was used to simulate 17 regimens, including meropenem, imipenem, cefepime, ceftazidime, piperacillin-tazobactam, tigecycline, and polymyxin B based on patients' characteristics and the antimicrobial resistance data for the main pathogens isolated from blood specimens in Shandong province (China). A regimen for which the cumulative fraction of response (CFR) was 90% or more was considered optimal. For Escherichia coli and Klebsiella pneumoniae, all carbapenem regimens, ceftazidime (2gq8h, 0.5 hr, and 3hr infusion), and piperacillin/tazobactam (4.5gq8h, 3 hr infusion) achieved CFRs above 90%. The meropenem regimen (2gq8h, 3 hr) achieved CFRs above 90% for both ceftriaxone or cefotaxime-resistant (CRO/CTX-R) E. coli and K. pneumoniae. For Pseudomonas aeruginosa, ceftazidime and meropenem (2gq8h, 0.5 hr, and 3 hr infusion) achieved optimal CFRs. None of the β-lactam regimens examined achieved a CFR above 80% for Acinetobacter baumannii. For all examined bacteria, polymyxin B (50 mg q12h) led to a CFR above 90%.
Conclusion:
PK/PD modeling based on local antimicrobial resistance data provides valuable guidance for clinicians for the administration of empirical antibiotic treatments for BSIs.
Introduction
Bloodstream infections (BSI
The increasing rates of drug resistance, multidrug-resistant microorganisms, and serious infections are significant challenges for clinicians. Thus, there is increasing use of population pharmacokinetics with Monte Carlo simulations to address this issue. This approach considers microbiological and pharmacokinetic variabilities to determine the probability that an antibiotic regimen will achieve the maximal microbiological effect, referred to as “pharmacodynamic target attainment.”7–9
The pharmacodynamic parameters associated with sterilization effects vary among different antimicrobial classes. In particular, some antibacterial drugs are considered effective when the free plasma concentration is maintained above the minimum inhibitory concentration (MIC) (fT > MIC) for a sufficient duration of the dosing interval; other drugs are considered effective based on the area under the concentration/time curve (AUC/MIC) or the maximum free drug concentration above the MIC (fCmax/MIC). 7 Several previous pharmacokinetic/pharmacodynamic (PK/PD) studies10–12 were performed based on MIC distributions from large antimicrobial surveillance programs, but did not consider variations of bacterial resistant rates among different sites.
We examined the MIC distributions of Gram-negative bacteria isolated from blood cultures of adults with BSIs in Shandong province from October 2017 to September 2018, as a basis for PK/PD modeling. In particular, we first considered location-specific information to optimize the empiric treatment of Gram-negative bacterial BSIs of adults in China and then determined the probabilities of attaining targeted pharmacodynamic exposures for seven potential intravenous antimicrobials against four bacteria (Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii) collected from the blood cultures.
Methods
Antimicrobials
Seven antimicrobials and 17 dosing regimens were examined, based on their common use for treatment of Gram-negative bacterial infections in China (Table 1). A 30-min infusion was considered as standard infusion (SI), and a 3-hr infusion as prolonged infusion (PI).
Antibiotic Regimens Used in the Monte Carlo Simulations
Microbiology
The microbiologic data for adult BSIs were collected from the Antimicrobial Surveillance Resistance System of Shandong Province (162 hospitals) from October 1, 2017 to September 30, 2018, as obtained by the China Antimicrobial Resistance Surveillance System (CARSS), and are representative of the bacterial BSIs during this period in Shandong province. Blood samples were collected into bilateral double bottles (8–10 mL each) from ∼30% of patients and into unilateral double bottles in the other patients. Appropriate automated blood culture instruments were used during these procedures. Species identification was performed using standard biochemical methodology with the Vitek 2 (bioMérieux, France), MicroScan WalkAway-96 (Siemens), or Phoenix-100 (BD) and/or matrix-assisted laser desorption/ionization (MALDI)-time of flight (TOF) mass spectrometry (MS). One or more positive blood cultures were required for diagnosis of Gram-negative bacteria. The MICs of the examined antimicrobials were determined by agar dilution or an automated system, following instrument specifications and according to guidelines of the Clinical and Laboratory Standards Institute. 13 Identification of strains and antibiotic sensitivity testing were performed by members of the bacterial resistance monitoring network (162 hospitals), and all data were reported to the CARSS each quarter.
The MIC distributions of the selected antimicrobials for the target pathogens were analyzed by WHONET 5.6 software. Only the first isolate of a given species from a patient was analyzed according to CLSI M-39. 14 MICs ranged from 0.06 mg/L to 128 mg/L for all antibiotics. A MIC less than 0.06 mg/L was classified as 0.06 mg/L, and a MIC greater than 128 mg/L as 128 mg/L.
PK/PD modeling
Pharmacokinetic data were obtained from infected or critically ill adult patients with adequate renal function (estimated glomerular filtration rate [eGFR] ≥50 mL/min/1.73 m2). Some of the studies included patients with eGFRs below 50 mL/min/1.73 m2; for these studies, these patients were excluded from the analysis and pharmacokinetic parameters were recalculated. All pharmacokinetic parameters are expressed as mean ± standard deviations (Table 2).8,12,15–19 Monte Carlo simulations of 5,000 cases were used to estimate the steady-state drug concentration/time profile of each regimen. The methodology used to simulate bactericidal exposures was described in detail previously. 12 In brief, mean and standard deviations of total body clearance (ClT, L/h), volume of the central compartment (Vd1, L), transfer rate constant from the central to peripheral compartment (k12, h−1), transfer rate constant from the peripheral to central compartment (k21, h−1), and fraction unbound drug (%) were used as input variables for a two-compartment model, with constant intravenous input and output with first-order kinetics. The input parameters were assumed to have log-normal distributions, except for the fraction unbound, which was assumed to have a uniform distribution over the specified range.
Pharmacokinetic Parameters Used in the Monte Carlo Simulations
ClT, total body clearance; Vd1, volume of distribution in the central compartment; k12, transfer rate constant from central compartment to peripheral compartment; k21, transfer rate constant from peripheral compartment to central compartment.
The probability of target attainment (PTA), defined as the probability that a simulated patient achieves the pharmacodynamic goal, was calculated for MIC values from 0.06 mg/L to 128 mg/L. The MIC distributions of a given population of bacteria were then used to obtain a single estimate of the PTA for these bacteria, termed the “cumulative fraction of response” (CFR). Pharmacodynamic exposures were simulated as free drug (f) for the β-lactams and polymyxin B, and as total drug for tigecycline. The fAUC0–24h value for polymyxin B was derived as described in a previous pharmacokinetic study. 19 For comparisons, the pharmacodynamic targets of each antimicrobial were: 40% fT > MIC for carbapenems; 50% fT > MIC for all other β-lactams; AUC0–24h/MIC of 6.96 for tigecycline; and fAUC0–24h/MIC of 10 for polymyxin B.12,20 A regimen for which the CFR was 90% or more was defined as optimal. 21
Statistical analysis
SPSS version 17.0 (SPSS, Inc.) was used for statistical analysis. Continuous variables are presented as mean and standard deviations. The chi-square test was used to compare the CFRs of different groups (categorical variables). A difference was considered statistically significant when the two-tailed p value was below 0.05.
Results
There were 12,253 nonduplicated bacteria isolated from blood specimens of adult patients (15–65 years old) with BSIs from the Antimicrobial Surveillance Resistance System of Shandong province between October 2017 and September 2018. Gram-negative bacteria accounted for 62.32% (n = 7636) of the isolates and included 4049 strains of E. coli, 1644 strains of K. pneumoniae, 436 strains of P. aeruginosa, 284 strains of Enterobacter cloacae, 251 strains of A. baumannii, 101 strains of Proteus mirabilis, 80 strains of Enterobacter aerogenes, 78 strains of Serratia marcescens, 68 strains of Stenotrophomonas maltophilia, 52 strains of Klebsiella oxytoca, and 593 isolates of other species.
We focused on the two major species of Enterobacteriaceae (E. coli and K. pneumoniae) and the two major species of nonfermenting bacteria (P. aeruginosa and A. baumannii), which accounted for 83.97% of all infections by Gram-negative bacteria. Monitoring for extended-spectrum beta-lactamases (ESBLs) is not mandatory in Shandong province. Thus, we analyzed data on ceftriaxone and cefotaxime resistance in cases infected with E. coli or K. pneumoniae because of the known presence of third-generation cephalosporin-resistant isolates in this region. Drug sensitivity tests for ceftriaxone and cefotaxime were performed for 3,704 strains of E. coli (resistance rate: 52.3%) and 1,463 strains of K. pneumoniae (resistance rate: 24.7%). Table 3 shows the resistance rates of the targeted bacteria to all studied antibiotics. Figure 1 shows the distributions of MIC values for all studied antibiotics against the targeted bacteria.
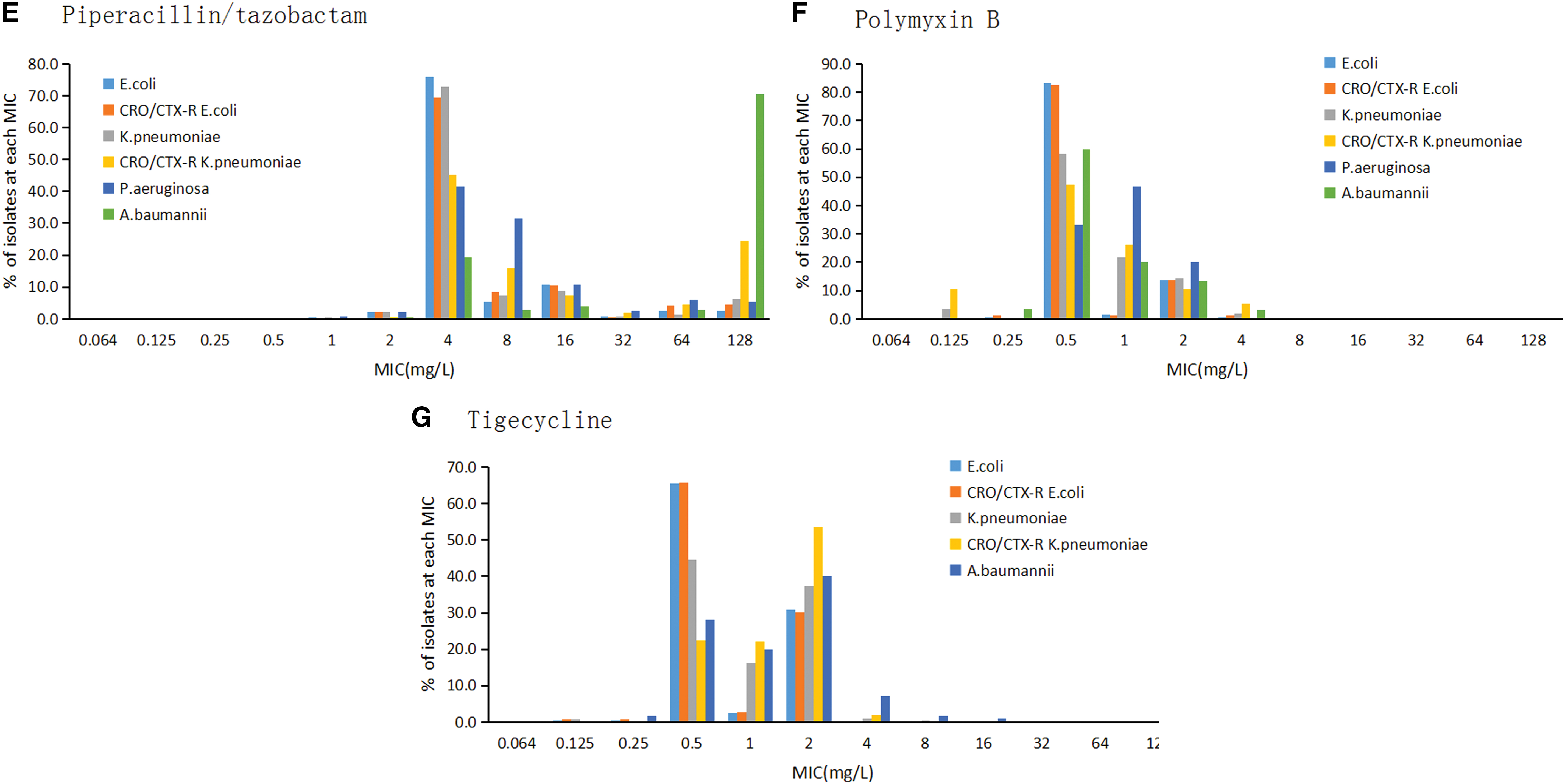
MICs for selected antimicrobials against different isolates of Escherichia coli (Colored in wathet), CRO/CTX-R E. coli (orange), K. pneumonia (gray), CRO/CTX-R Klebsiella pneumonia (yellow), Pseudomonas aeruginosa (mazarinet), and Acinetobacter baumannii (green). The selected antimicrobials included Cefepime
Resistance of Escherichia coli, CRO/CTX-R E. coli, Klebsiella pneumoniae, CRO/CTX-R K. pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii to Different Antibiotics
ND, not determined.
Table 4 shows the CFRs of all species for each antibiotic regimen based on the Monte Carlo simulations. The CFRs of E. coli and K. pneumoniae to piperacillin/tazobactam, ceftazidime, cefepime, and meropenem were significantly higher than those of CRO/CTX-R E. coli and CRO/CTX-R K. pneumoniae to these same drugs (p < 0.05 for all comparisons). However, E. coli and CRO/CTX-R E. coli had similar CFRs to imipenem, tigecycline, and polymyxin B. For imipenem and polymyxin B, the CFRs were significantly greater for K. pneumoniae than CRO/CTX-R K. pneumoniae (p < 0.05 for all comparisons). In response to all carbapenems, polymyxin B, and high-dose tigecycline (200 mg followed by 100 mg every 12 hr), E. coli and K. pneumoniae showed CFRs greater than 90%. In addition, K. pneumoniae had a CFR of 90.64% in response to ceftazidime (2 g every 8 hr with SI or PI) and a CFR of 94.20% in response to piperacillin/tazobactam (4.5 g every 8 hr with PI). For β-lactam regimens, PI led to slightly greater CFRs than did SI.
Cumulative Fraction of Response for Different Antibiotic Regimens Against Isolates of E. coli, CRO/CTX-R E. coli, K. pneumoniae, CRO/CTX-R K. pneumoniae, P. aeruginosa, and A. baumannii Based on Monte Carlo Simulations
fT > MIC, portion of dosing interval during which free drug concentration is maintained above the MIC. The chi-square test was used to compare CFRs of total E. coli versus CRO/CTX-R E. coli, and of total K. pneumoniae versus CRO/CTX-R K. pneumoniae.
Bold values indicate that differences were significant at p < 0.05.
All antibiotics were simulated as 0.5-hr infusions unless noted.
CFR is reported as a percentage of 5,000 simulated patients.
Pharmacodynamic target: 50% fT > MIC.
Pharmacodynamic target: 40% fT > MIC.
Pharmacodynamic target: AUC0–24h/MIC ≥6.96.
Pharmacodynamic target: fAUC0–24h/MIC ≥10.
AUC, area under the drug concentration/time curve; MIC, minimum inhibitory concentration; NA, no data available.
Analysis of CRO/CTX-R E. coli indicated that all carbapenems, polymyxin B, and high-dose tigecycline achieved CFRs greater than 90%. For CRO/CTX-R K. pneumoniae, meropenem (2 g every 8 hr with PI), polymyxin B, and high-dose tigecycline achieved CFRs greater than 90%. For P. aeruginosa, ceftazidime (2 g every 8 hr), meropenem (2 g every 8 hr with SI or PI), polymyxin B, and high-dose tigecycline achieved CFRs greater than 90%, but all imipenem, piperacillin/tazobactam, and cefepime regimens had CFRs below 90%. Because of the high MICs of all β-lactams against A. baumannii, none of tested β-lactam regimens (regardless of dose) achieved a CFR above 80%. However, for A. baumannii, the CFR to polymyxin B was 93.51%, the CFR to high-dose tigecycline was 90.95%, and the CFR to meropenem (2 g every 8 hr with PI) was 76.6%. For meropenem (2 g every 8 hr), PI resulted in a 29.87% greater CFR compared with SI.
Discussion
Successful clinical treatment of BSIs requires appropriate clinical experience and knowledge of the local prevalence rates of drug-resistant species. The prevalence of antibiotic-resistant Gram-negative pathogens has greatly increased in the Asia-Pacific region.22,23 Thus, it is essential that clinicians who are administering empirical antibiotic treatment consider local and recent data on antimicrobial resistance. Our study analyzed empirical antibiotic monotherapies for BSIs caused by the four major species of Gram-negative bacteria using Monte Carlo simulations to model in vivo antibiotic pharmacodynamics.
Our assessments of E. coli and K. pneumoniae collected from blood specimens suggested that most of the studied broad-spectrum β-lactams (except cefepime) were effective. Consistent with previous findings in an Asian population, 11 we found that all standard imipenem and meropenem regimens achieved CFRs greater than 90% for treatment of E. coli and K. pneumoniae. Ceftazidime (2 g every 8 hr with SI or PI) and piperacillin/tazobactam (4.5 g every 8 hr with PI) also achieved CFRs greater than 90%. These results suggest that clinicians considering a standard regimen of carbapenems or ceftazidime and piperacillin/tazobactam should increase the dose or infusion time to cover this population of Enterobacteriaceae, except when ESBL-producing or carbapenem-resistant Enterobacteriaceae (CRE) are endemic to the hospital.
For treatment of CRO/CTX-R E. coli, all carbapenems and polymyxin B regimens achieved the optimal CFRs (>90%). The MICs of carbapenems for CRO/CTX-R K. pneumoniae were much higher than those for CRO/CTX-R E. coli. Meropenem (2 g every 8 hr with PI), polymyxin B, and high-dose tigecycline regimens achieved CFRs greater than 90%. The China Antimicrobial Surveillance Network (CHINET) indicated a marked increase of K. pneumoniae resistance to carbapenems from 2005 (2.4% to 2.6%) to 2014 (10.5% to 13.4%). 24 Our data indicated that 1.41% of E. coli and 4.04% of K. pneumoniae were carbapenem resistant. Cefepime regimens and tigecycline with standard dosing (100 mg followed by 50 mg every 12 hr) achieved the lowest CFRs against E. coli and K. pneumoniae. Thus, we urge caution when using cefepime as empiric monotherapy for BSIs due to Enterobacteriaceae.
There is an increasing worldwide focus on nonfermenting bacteria, mainly A. baumannii and P. aeruginosa, because multidrug resistance is common in these species. 25 Our results indicate high treatment success for BSIs due to P. aeruginosa. In particular, ceftazidime (2 g every 8 hr) and meropenem (2 g every 8 hr with SI or PI), polymyxin B, and high-dose tigecycline were all effective empirical treatments. For A. baumannii, none of the tested regimens achieved an optimal CFR, except the polymyxin B regimen and the high-dose tigecycline regimen. Higher doses with PIs of β-lactams slightly improved CFRs. Combination therapy, or selection of other antimicrobials with different mechanisms of action, may be required to address the high level of A. baumannii resistance in this region. 26
Compared with other studies in the Asia-Pacific region, 11 our results indicated lower CFRs for carbapenems in the treatment of Enterobacteriaceae, but higher CFRs for carbapenems against nonfermenting bacteria. In accordance with some other global data,11,12,27 a high-dose β-lactam regimen with PI increased the CFRs of all agents, but it was less effective against A. baumannii and P. aeruginosa due to the increasing resistance of these species. Moreover, we did not simulate imipenem regimens with PI, because this drug is not suitable for PI due to its low stability in solution and high central nervous system toxicity at higher doses. 28 In contrast to our results, a recent multicenter randomized controlled trial reported no significant survival benefit from PI relative to SI. 29
We found that tigecycline, which is mainly used for treatment of complicated skin, soft-tissue, and intra-abdominal infections in adults, had low CFRs against Gram-negative bacteria. Remarkably, due to its rapid movement from the bloodstream into tissues after administration, peak tigecycline serum levels are low (0.63–1.4 μg/mL) after standard dosing (100 mg followed by 50 mg every 12 hr). 30 Thus, its use for BSIs caused by organisms with a MIC of 1 μg/mL seems questionable. 6 In line with another study, 31 a high-dose tigecycline regimen (200 mg followed by 100 mg every 12 hr) was reported as a reasonable strategy for BSIs and other severe infections by CRE. More prospective studies are needed to determine the clinical benefit and safety of PI of β-lactams and high-dose tigecycline, especially for infections by CRE and nonfermenting Gram-negative bacteria. 6
Polymyxins (colistin and polymyxin B) are often considered the treatment of last resort for carbapenem-resistant organisms. 32 We found that polymyxin B (50 mg every 12 hr) led to a CFR above 90% for all targeted bacteria. For carbapenem-resistant organisms in vitro, polymyxin/carbapenem combinations have synergistic effects and greater bactericidal activity than polymyxins alone, especially for A. baumannii. 33 However, the use of polymyxin-combination regimens remains controversial. A randomized controlled superiority trial recently demonstrated that addition of meropenem to colistin (relative to colistin monotherapy) did not improve clinical outcomes in patients with severe A. baumannii infections. 34 Future randomized trials are needed to compare the efficacies of different antibiotic regimens for the treatment of infections by carbapenem-resistant organisms if the incidence continues to increase.
We used Monte Carlo simulations to compare the pharmacodynamic profiles of commonly used antimicrobial agents against adult BSIs due to Gram-negative bacteria based on local microbiological data. Because only limited pharmacokinetic data are available for Chinese individuals, we used the data of patients with adequate renal function (eGFR ≥50 mL/min/1.73 m2) worldwide. We utilized Monte Carlo simulation to predict clinical success, similar to other studies,12,27 without considering factors such as host status and use of combination therapies, because these may lead to different outcomes in clinical practice. Furthermore, the number of strains monitored for polymyxin B susceptibility was small compared with the total number of strains, and it is unknown whether the MIC distribution reflects overall drug resistance. Finally, more prospective studies are needed to evaluate the treatment efficacies of the applied antimicrobial regimens.
Conclusion
Our results indicate that carbapenem, ceftazidime, and piperacillin/tazobactam regimens have high probabilities of achieving efficient control of adult BSIs caused by E. coli and K. pneumoniae, except for CRO/CTX-R isolates. Standard-dose carbapenem regimens are effective against CRO/CTX-R E. coli, and a high-dose carbapenem regimen with PI should be considered for CRO/CTX-R K. pneumoniae. Caution should be exercised when treating BSIs with standard doses of cefepime and tigecycline. A. baumannii has a high rate of resistance to most of the drugs studied here, and this also poses a serious challenge to clinicians. Polymyxin B and a high-dose regimen of tigecycline should be considered as last resorts for treatment of multidrug-resistant Gram-negative bacteria. Thus, it is critical to be aware of local data on resistance and MIC distributions, so that the optimal dosing regimens can be given to patients with BSIs.
Footnotes
Acknowledgments
The authors thank all members of the Antimicrobial Surveillance Resistance System of Shandong Province for providing bacterial data, and Professor Yonghong Xiao (First Affiliated Hospital, College of Medicine, Zhejiang University) for technical support.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was funded by a research grant from the Science and Technology Project of Jinan, Shandong province, P.R. China (201805018).