
Abstract
Streptomycin (STR) is the first antibiotic used in the treatment of tuberculosis (TB) and the earliest antituberculosis drug with acquired resistance developed by Mycobacterium tuberculosis. The high prevalence of such resistance in many parts of the world limits its use for treating multidrug-resistant (MDR) TB. The aims of this study are to characterize of mutations in rpsL, rrs, and gidB genes in MDR M. tuberculosis isolates originating from southern China and to investigate possible relationship between mutations and strain genotypes for precise diagnosis and treatment. Sequences of rpsL, rrs, and gidB genes and the resistance profiles were analyzed for 218 MDR M. tuberculosis isolates. Our study showed that 68.35% of MDR M. tuberculosis isolates were resistant to STR and 89.91% of STR-resistant (STRR) isolates were Beijing lineage strains. Mutations were observed in STRR MDR M. tuberculosis isolates at the following rates: 72.48% in rpsL, 36.91% in rrs, and 15.44% in gidB. Compared with the phenotypic data, the combination of mutations in rpsL, rrs, and gidB has sensitivity and specificity of 96.64% and 100.00%, respectively. The most common mutations in STRR isolates were rpsL128,263 and rrs514,1401, of which rpsL128 showed association with Beijing lineage (p < 0.001). It is noteworthy that a1401g mutation was present in rrs, while MDR M. tuberculosis isolates were resistant to both STR and amikacin. Twenty two novel mutations were found in STRR isolates. These findings could be helpful to develop rapid molecular diagnostic methods and understand STR resistance in China for developing TB precision medicine and disturbance of drug-resistant TB transmission.
Background
Tuberculosis (TB) is still a major public health threat globally today. Multidrug-resistant (MDR) TB defined by resistance to at least two important first-line drugs, isoniazid (INH) and rifampicin (RIF), and extensively drug-resistant (XDR) TB strains, defined as MDR-TB with additional resistance to any fluoroquinolone (FQ) and one of the second-line injectable anti-TB drugs such as amikacin (AMK), capreomycin (CAP), or kanamycin (KAN), are emerging. In 2017, the World Health Organization (WHO) estimated that 558,000 people developed TB that was resistant to RIF, the most effective first-line drug, and of these, 82% (457,560 out of 558,000) were MDR-TB cases worldwide. 1 Among cases of MDR-TB in 2017, 8.5% were XDR-TB. 1 Therefore, effective and rapid tools are required for early diagnosis of MDR-TB and XDR-TB to enable effective treatment and control of transmission of drug-resistant (DR) TB.
The aminoglycoside antibiotic streptomycin (STR), derived from Streptomyces griseus, was the first antibiotic successfully used against Mycobacterium tuberculosis in the 1940s. STR was then used with INH and para-aminosalicylic acid (PAS), which were subsequently discovered as first-line treatment for TB. With the further discovery of pyrazinamide (PZA) and RIF, STR was incorporated in the initial phase of short-course therapy of TB that comprises RIF, PZA, and INH. The role of STR was primarily replaced by that of ethambutol (EMB) later on in 6-month short-course TB therapy. 2 The widely used TB regimens for both treated and new TB patients in China are 2 months of INH, RIF, PZA, and EMB followed by 4 months of INH and RIF (2HRZE/4HR) or 2 months of INH, RIF, PZA, EMB, and STR followed by 6 months of INH and RIF (2HRZES/6HR). 3 It may still have a role in treatment of MDR-TB, although with limitation imposed by the high prevalence of bacillary resistance and drug toxicities, especially regarding the otovestibular and renal systems. One of the main obstacles to treat MDR-TB strain is drug regimen, which is prolonged, poorly effective, expensive, and has serious side effect. However, second-line injectable drugs are the most ambiguous medications in use for MDR-TB strains. 4 Injectable drugs are administered intramuscularly for 4 to 8 months and cause of pain and distress for TB patients. These injectable drugs are associated with side effects and perhaps the most serious problem is permanent hearing loss of people receiving them for MDR-TB.5–7 No new important anti-tuberculosis drugs introduced as alternatives to injectable drugs till now. 7 AMK and STR are to be considered for use in MDR-TB regimens if drug susceptibility testing (DST) results ensure susceptibility. 8 STR is to be considered if DST results ensure susceptibility and AMK is not available or documented resistance. 8 The other two second-line injectable drugs, KAN and CAP are no longer recommended for treatment in MDR-TB regimen. 8 However, STR continues to be an essential component either as the first-line drug or in combination therapy with other drugs for chemotherapy of TB. 9
Resistance to STR is mostly due to the chromosomal mutations. Mutation-carrying genes, for instance rpsL and rrs encoding the S12 ribosomal protein and 16S rRNA, respectively, are associated with intermediate or high level of STR resistance.9–14 The most predominant changes are detected at codon 43 and 88 in the rpsL gene as well as in two specific regions of rrs gene (the 530 loop and the 912 loop).9,15 A strong correlation presents between the level of resistance and the position and the type of the mutations.16,17 There is an important association between Beijing strains and the codon K43R in rpsL gene compared with the group of STR-resistant (STRR) non-Beijing clinical strains (p < 0.001). 18 However, recent studies reported that the mutations rate causing drug resistance showed difference among lineages. The Beijing strain family is strongly linked with DR-TB in many settings and showed increased rate of mutation in vitro.19–21 The Beijing genotype strain was most common (up to 90.2% of strains) in China. 11 In addition, mutations in the gidB gene are liable for low level of STR resistance through comparative STRR versus STR-susceptible (STRS) isolate genomic sequences and the resistance profiles revealed by gene knockout. 22 The gidB (Rv3919c) gene encodes an S-adenosylmethionine-dependent 7-methylguanosine (m7G) methyltransferase and methylate the G527 in the 530 loop of the 16S rRNA. The mutation in gidB was found to be linked with the STR resistance due to the gidB mutant and lacked m7G modification by high-performance liquid chromatography analysis of 16S rRNA. 22
Recently, screening for mutations in these three genes is an interesting and promising approach for reliable and rapid diagnosis of STRR TB. In most of the cases, mutations in two genes (rpsL and rrs) have been well recognized as highly specific predictive markers for STR resistance. The type and frequency of STR resistance-associated mutations varied depending on the population and geographical areas. However, previously, several studies showed that the frequency of mutations differs between countries, ranging from 37.7% to 94.6%.9–12,23–25
STR drug resistance in TB is a very serious issue in China. 11 The frequency of resistance to STR reached notable levels (37.3–87.0%) among MDR-TB clinical isolates.11,26–28 Therefore, it is very significant to determine the genes related to the resistance to STR for defining the real usefulness of this drug in treating patients with DR-TB. The objectives of the present study were to characterize mutations in rpsL, rrs, and gidB genes and to analyze possible relationship between genetic mutations and strain genotypes in MDR M. tuberculosis clinical isolates originating from southern China for early effective treatment and disturbance of DR-TB transmission.
Materials and Methods
Ethical statement
The present study was approved by the Ethics Committee of Guangzhou Chest Hospital (GZXK-2016-015). The study methods were performed in accordance with the approved guidelines.
Collection of MDR M. tuberculosis clinical isolates
Two hundred eighteen MDR M. tuberculosis clinical isolates were collected randomly from 400 MDR-TB patients (age range, 17 to 79 years) for the present study during the period from 2016 to 2018 at the biggest TB special hospital, Guangzhou Chest Hospital, in southern China. Each MDR M. tuberculosis clinical isolate was collected from each patient individually. In this study, the M. tuberculosis reference strain (H37Rv ATCC27294T) was used as control.
Drug susceptibility testing
DST was performed for M. tuberculosis clinical isolates using Lowenstein-Jensen (L-J) method recommended by WHO.29,30 The concentrations of drugs (μg/mL) in L-J medium were as follows: INH 0.2, RIF 40.0, STR 4.0, EMB 2.0, rifabutin (RFB) 20.0, moxifloxacin (MOX) 2.0, levofloxacin (LEV) 3.0, AMK 40.0, and prothionamide (PTH) 40.0, and PAS 1.0.29,30 The diluted bacterial suspension of M. tuberculosis clinical isolates was cultured onto L-J medium containing drugs or without drugs and incubated at 37°C for up to 42 days to acquire results. A strain was considered as resistant to a drug when M. tuberculosis growth rate is ≥1% compared to the drug-free control.
DNA isolation of M. tuberculosis strains
Scraped mycobacterial colonies were collected in 400 μL of distilled water and boiled at 100°C for 10 min to inactivate bacteria and release the mycobacterial DNA.31,32 Recovered mycobacterial DNA was immediately used for polymerase chain reaction (PCR) amplification or stored at −20°C until use. 33
PCR amplification and DNA sequencing
Amplification of drug resistance genes; rpsL, rrs, and gidB was performed by PCR using specific primers. The oligonucleotide primers of the above genes conducted for PCR amplification were newly designed in our study (Supplementary Table S1), based on the sequences of the respective genes of the M. tuberculosis H37Rv strains. The PCR products were observed in 0.7–1.0% agarose gels and purified using PCR purification kit and finally, sent out for sequencing. All sequencing data were aligned with the corresponding sequences of M. tuberculosis standard wild-type H37Rv strain (GenBank accession number NC_000962) using ClustalW2 software.
Nucleotide sequence accession numbers
The nucleotide sequences of the rrs and gidB genes containing novel mutations were deposited in the GenBank database (www.ncbi.nlm.nih.gov) under the following accession numbers: MN645911, MN645912, MN645913, MN645914, MN645915, and MN645916 for the rrs gene mutants and MN645917, MN645918, MN645919, MN645920, MN645921, MN645922, MN645923, MN645924, MN645925, MN645926, MN645927, MN645928, MN645929, and MN645930 for the gidB gene mutants.
PCR assay for identification of Beijing and non-Beijing strains
PCR assay was performed for confirmation of M. tuberculosis strains as well as differentiation between Beijing strains and non-Beijing strains. As previously reported, region spanning genes Rv2816 to Rv2819, including part of Rv2820, are deleted in all Beijing lineage strains of M. tuberculosis strain. 34 So, three sets of PCR primers were used to differentiate between Beijing strains and non-Beijing strains based on the above information. The first set of primers of IS-F: 5′ GCGCCAGGCGCAGGTCGATGC 3′ and IS-R: 5′ GATCAGCGATCGTGGTCCTGC 3′ amplifies a 523 bp PCR product from IS6110, which appeared in all M. tuberculosis isolates. 35 The second set of primers, BJ-F: 5′ACCGAGCTGATCAAACCCG3′ and BJ-R: 5′ATGGCACGGCCGACCTGAATGAACC3′ amplifies a 239 bp PCR product containing region specific part of Rv2819 and part of Rv2820 from the Beijing strains of M. tuberculosis. 34 The third set of primers, nBJ-F: 5′GATCGCTTGTTCTCAGTGCAG3′ and nBJ-R: 5′CGAAGGAGTACCACGTGGAG3′ amplifies a 539 bp PCR product from the Rv2819 gene of non-Beijing strains of M. tuberculosis. 34 The PCR products were observed by electrophoresis on a 2% agarose gels.
Statistical analysis
Sensitivities, specificities, accuracies, and confidence intervals (CI) were calculated using the MedCalc statistical software. Odds ratios (ORs) were also calculated to assess relative risk. A two-sided p-value of <0.05 was considered statistically significant.
Results
Demographic characteristics
Among 218 MDR M. tuberculosis clinical isolates, 154 (70.64%) patients were male and 64 (29.36%) were female. The TB patients were the majority in the age group of 25–44 years. In addition, 74 (33.94%) were new cases of TB patients and 144 (66.06%) were previously treated (Supplementary Table S2). All TB cases were human immunodeficiency virus negative.
Drug-resistant profiles
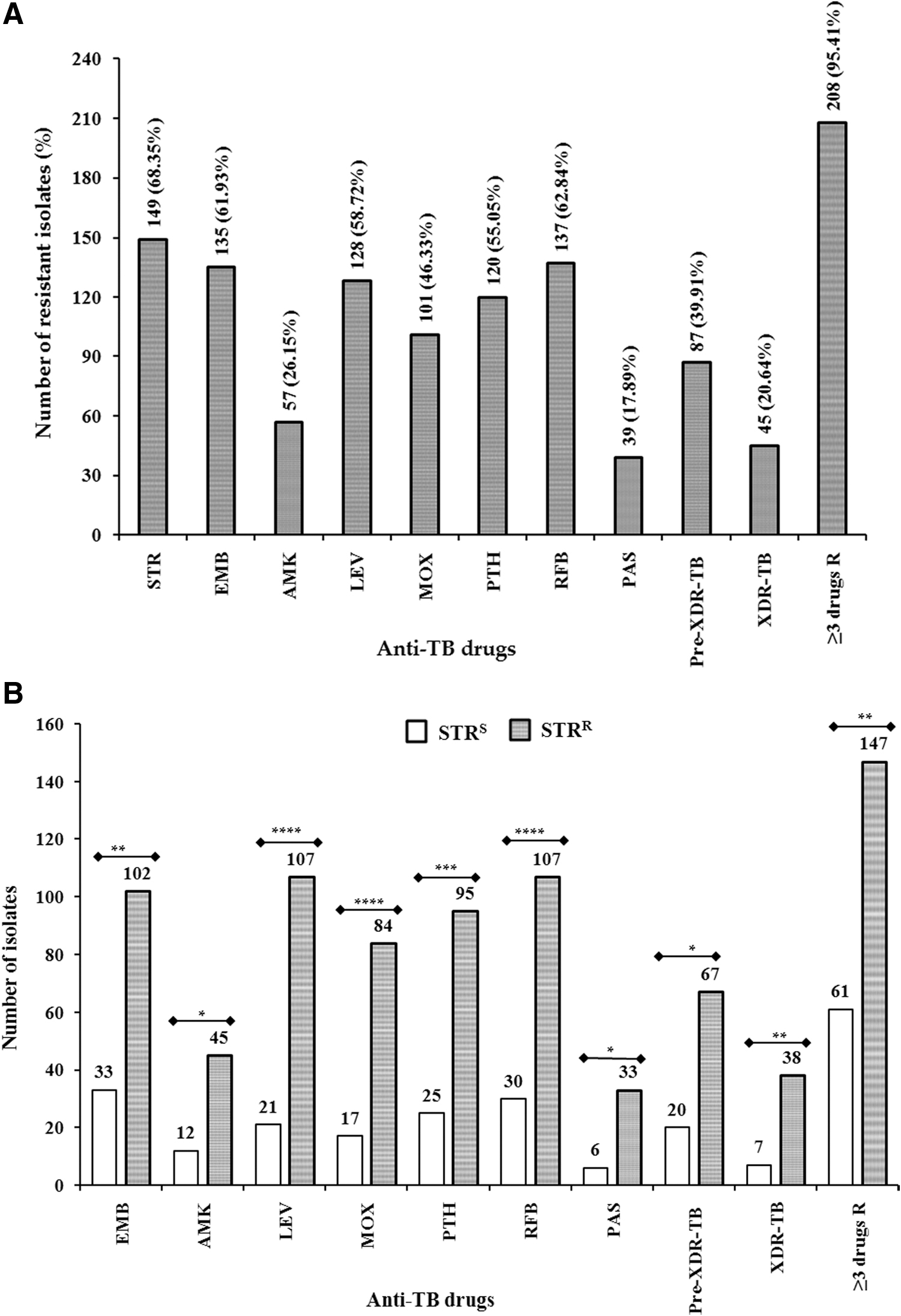
Among 218 MDR M. tuberculosis clinical isolates, 149 isolates were STRR and 69 isolates were STRS, but resistant to other first- and second-line drugs. Drug susceptibility profiles are shown in Fig. 1A. Resistant to EMB, AMK, LEV, MOX, PTH, RFB, PAS, pre-XDR (defined as MDR-TB with additional resistance to FQ or a second-line injectable drug such as AMK, KAN, or CAP), XDR, and ≥3 drugs was observed in 61.93%, 26.15%, 58.72%, 46.33%, 55.05%, 62.84%, 17.89%, 39.91%, 20.64%, and 95.41% of the DR isolates, respectively. Data analysis revealed a significant association between STR-resistant isolates and resistant isolates to EMB (OR, 2.37; 95% CI, 1.32–4.25), AMK (OR, 2.06; 95% CI, 1.01–4.20), LEV (OR, 5.82; 95% CI, 3.12–10.88), MOX (OR 3.95; 95% CI, 2.09–7.47), PTH (OR 3.10; 95% CI, 1.71–5.61), RFB (OR 3.31; 95% CI, 1.83–6.00), PAS (OR 2.84; 95% CI, 1.13–7.14), pre-XDR (OR 2.00; 95% CI, 1.09–3.69), XDR (OR 3.03; 95% CI, 1.28–7.19), and ≥3 drugs (OR 9.64; 95% CI, 1.99–46.71) (Fig. 1B).
Drug resistance patterns:
Mutations in rpsL gene
Both STRR and STRS MDR M. tuberculosis clinical isolates were analyzed for mutations in the three genes rrs, rpsL, and gidB (Table 1). Mutations in the rpsL gene were detected in 108 (72.48%; 108/149) of the STRR and none of the STRS isolates. Among 218 MDR M. tuberculosis clinical isolates, five types of mutations were found in the rpsL gene. Eighty-nine isolates (59.73%; 89/149) were a128g (K43R) transition mutations and one isolate was a128c (K43T) transversion mutation. A synonymous mutation T39T was found coexisted with nonsynonymous mutation K43R in the rpsL gene. Seventeen isolates (11.41%; 17/149) were a transition mutation a263g (K88R) (Fig. 2) and one isolate was a transversion mutation a263c (K88T). Another one isolate had silent c117t (T39T) mutation. Of the STRR MDR M. tuberculosis clinical isolates, 27.52% had no mutations in the rpsL gene.
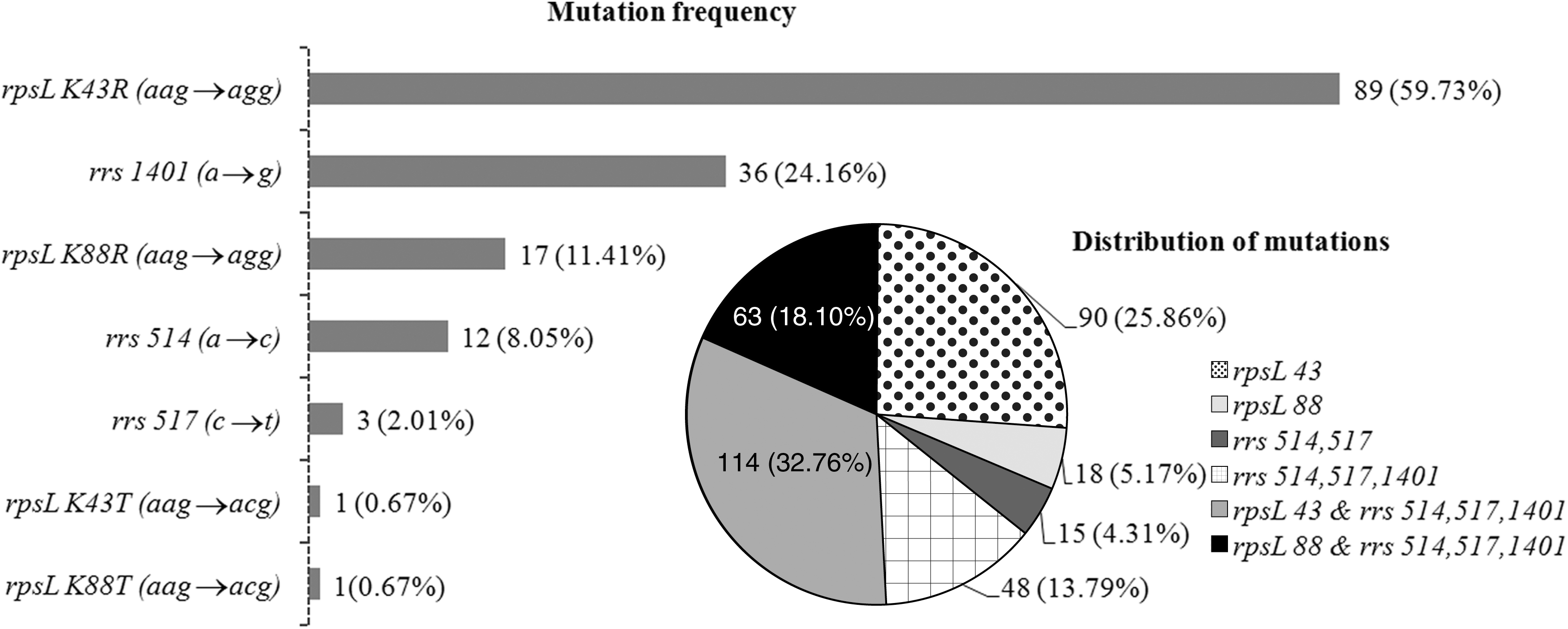
Frequency and distribution of mutations derived from the results of sequencing assay. The histogram represents the frequency of individual mutations. Pie chart depicts the distribution of these mutations.
Mutations in the rpsL, rrs, and gidB Genes Among 218 Multidrug-Resistant Mycobacterium tuberculosis Clinical Isolates
Novel mutations are underlined.
Lineage-specific polymorphisms were not included.
A synonymous mutation.
STR, streptomycin; STRR, STR-resistant; STRS, STR-susceptible; WT, wild type.
Mutations in rrs gene
Fifty-five STRR MDR M. tuberculosis clinical isolates (36.91%; 55/149 isolates) carried 10 different types of mutations in the rrs gene (Table 1). Among them, the most frequent mutations were a1401g and occurred in 36 (24.16%; 36/149) STRR MDR M. tuberculosis clinical isolates, while a514c were identified in 12 (8.05%; 12/149) STRR MDR M. tuberculosis clinical isolates and three STRR MDR M. tuberculosis clinical isolates had c517t mutations (Fig. 2). Notably, six novel mutations were found in the rrs gene (Table 1). Furthermore, 28 (18.79%; 28/149) STRR MDR M. tuberculosis clinical isolates carried mutations in rrs with rpsL gene. Of the STRR MDR M. tuberculosis clinical isolates, 63.09% had no mutations in rrs gene. None of the STRS MDR M. tuberculosis clinical isolates carried mutations in rrs gene.
Mutations in gidB gene
Mutations in the gidB gene were found at a frequency of 15.44% (23/149) among STRR MDR M. tuberculosis clinical isolates. Furthermore, eight (5.36%, 8/149) STRR MDR M. tuberculosis clinical isolates that had seven mutations in the gidB gene coincided with rrs gene. Of the 218 MDR M. tuberculosis clinical isolates, two different substitutions, which are a276c (E92D) and a615g (A205A) mutations, were identified in the gidB gene, including 179 MDR M. tuberculosis clinical isolates and 17 MDR M. tuberculosis clinical isolates, respectively. These two substitution mutations are lineage marker, representing Beijing strain and Central Asian (CAS) strain. Thus, a276c and a615g mutations were found in both STRR and STRS isolates and not included in Tables 1 and 2. Moreover, there were 23 STRR MDR M. tuberculosis clinical isolates that had 19 different types of mutations, including 17 nonsynonymous mutations and 2 frame-shift mutations. Of them, 16 mutations were identified as novel (Table 1). Mutations t64g, g98del, and g227c in gidB gene were identified coexisting with a change at codon 43 in the rpsL gene. In addition, another two mutations t272g and t583c were found coexisting with a change at codon 88 in the same gene.
The Evaluation Between DNA Analysis and Phenotypic Drug Susceptibility Testing
The diagnostic performance of DNA sequencing in comparison with drug susceptibility testing was analyzed after excluding synonymous mutations.
Lineage-specific polymorphisms and mutations not likely to cause STR resistance were excluded.
CI, confidence intervals.
Prediction of STRR in MDR M. tuberculosis clinical isolates based on DNA sequencing
To assess the performance of DNA sequencing to predict STR resistance, the genotypic and phenotypic data for all 218 MDR M. tuberculosis clinical isolates were compared (Table 2). Using phenotypic outcomes as the reference, mutation detection in the rpsL gene exhibited a sensitivity of 72.48% (95% CI, 64.57–79.47%) and a specificity of 100.00% (95% CI, 94.79–100.00%). When rpsL, rrs, and gidB mutations were evaluated together, the assay sensitivity increased to 96.64% (95% CI, 92.34–98.90%) and a specificity of 100.00% (95% CI, 94.79–100.00%). In addition, combination of three mutations at rpsL128, 263, and rrs514 or 1401 exhibited with 79.87% (95% CI, 72.52–85.98%) sensitivity, 100.00% (95% CI, 94.79–100.00%) specificity, and 86.24% (95% CI, 80.94–90.52%) accuracy (Table 2).
Genotypes and mutations in rpsL, rrs, and gidB genes
The distributions of different mutation types in rpsL, rrs, and gidB genes between Beijing and non-Beijing genotypes among 218 MDR M. tuberculosis clinical isolates are summarized in Table 3. Statistical analysis revealed that only significantly statistical difference was found in the mutated site rpsL128 (p < 0.001) and gidB104 (p = 0.03) between Beijing and non-Beijing genotypes.
Mutations Within rpsL, rrs, and gidB Versus Beijing and Non-Beijing Strains Genotypes
p < 0.001.
Discussion
To the best of our knowledge, the present report represents one of the largest studies regarding MDR M. tuberculosis and STRR MDR M. tuberculosis clinical isolates in southern China. Among 218 MDR M. tuberculosis clinical isolates, 39.91% isolates were pre-XDR, 20.64% isolates were XDR, and 68.35% isolates had resistance to STR. Of the 149 STRR MDR M. tuberculosis clinical isolates, 44.97% and 25.50% isolates were pre-XDR- and XDR-TB strains, respectively. Several studies in different countries have reported that overall rates of STRR clinical isolates were ranging from 63.8% to 82.2%.10,11,15,18,25,36–39 The high frequencies of STR resistance and its obvious side effect strongly suggest that STR susceptibility testing is highly needed before considering it for the treatment of TB patients. STR resistance is associated with mutations in rpsL, rrs, and gidB genes.9,15 The present findings reported that 96.64% isolates were mutations in the rpsL, rrs, and gidB genes in STRR MDR M. tuberculosis clinical isolates. The frequency of mutations within the rpsL, rrs, and gidB genes associated with STR resistance reached notable levels (37.7–83.7%) among STRR M. tuberculosis clinical isolates.9,12,18,23 On the contrary, eight STRR isolates had a novel silent mutation at amino acid position 121 (K12K) in the rpsL gene and no nonsynonymous mutation was found in any of the STRR clinical isolates in northern India. 40 In the same study, no mutation was detected in the rrs gene. 40 In contrast, China, Republic of Korea, Singapore, and Latvia have reported the highest frequencies mutations, with 94.6%, 84.3%, 95.1%, and 84.8%, respectively.11,15,25,38
Regarding the genes associated with STR resistance, our study showed that 72.48% had mutations in rpsL gene in STRR MDR M. tuberculosis clinical isolates from southern China, consistent with the data from 64.71% in Republic of Korea, 15 and 78.26% in Beijing, China, 11 but higher than the findings from 63.63% in Thailand, 18 50% in Poland, 9 31.25% in Iran, 12 and 24.64% in Spain 23 (Table 4). The most common mutation found at codon 43 (K43R) predominated. Our present study confirmed mutation at codon 43 in rpsL gene occurred in 60.40% (90/149 isolates) of STRR MDR M. tuberculosis clinical isolates. A synonymous mutation (T39T) in rpsL gene coexisted with nonsynonymous mutation (K43R) was detected in a STRR clinical isolate. The frequency of rpsL gene mutations at codon 43 differed significantly among different geographical regions ranging from 11.6% to 64.4% in STRR M. tuberculosis clinical isolates.23,39 Beijing strain predominating areas exhibited the foremost frequencies of mutation at codon 43 (a128g).9,11 Our finding showed that this mutation was associated with Beijing lineage strain, consistent with the previous studies.11,25 The three mutations K88R, K88Q, and K88T at codon 88 were detected in STRR M. tuberculosis clinical isolates.18,25 Existence of the K88R mutation in the rpsL gene was not significantly associated with Beijing clinical strains (p = 0.730). 18 In the present study, two nonsynonymous mutations were found in rpsL gene at codon 88: K88R was detected in 17 STRR isolates, and K88T was detected in 1 STRR isolates. There was no significant association between K88R mutation and Beijing strains compared with the group of STRR non-Beijing isolates (p = 0.25). No STRS clinical isolates having mutations in the rpsL gene were observed.
Comparison Mutation Frequency of Three Genes rpsL, rrs, and gidB in Streptomycin-Resistant Isolates Documented in Different Countries
Lineage-specific polymorphisms and mutations not likely associated with resistance were excluded.
For rrs, we found that 36.91% of the STRR MDR M. tuberculosis clinical isolates harbored rrs mutations in the present study, which presented a higher rate in comparison with other prior studies as having rates ranging from 3.5% to 21.9% (Table 4).9,11,12,18,39 In contrast, the highest frequency mutations (44%) in the rrs gene were found in Iran. 12 Several studies revealed that alterations in the rrs gene were found in two highly mutable regions known as the 530 loop (514a→c; 517c→t) and the 912 loop (906a→g; 907a→t). 9 Alterations in the 530 loop region were observed in 8.05% (a514c) and 2.0% (c517t) of the STRR MDR M. tuberculosis clinical isolates. The 912 loop region showed one type of substitution, a908c in the present study, which has only been described by Wang et al. 41
It is very important to note that our results showed that mutation a1401g was present in 24.16% (36/149) MDR M. tuberculosis clinical isolates resistant to both STR and AMK. This suggests delineation of such mutation is helpful to guide the choice of aminoglycoside in the treatment of MDR M. tuberculosis patients with bacillary resistance to STR. Furthermore, six novel mutations with accession numbers, g12c (MN645911), c181g (MN645912), c310t (MN645913), c1274t (MN645914), t1465c (MN645915), and t1491c (MN645916) in the rrs gene were observed in STRR MDR M. tuberculosis clinical isolates. Two of these mutations were accompanied with mutations in rpsL or rrs. The role of these mutations remained unclear and required further exploration.
A substitution a276c in the gidB gene occurred in all Beijing family strains, suggesting that this mutation was Beijing lineage-specific marker. 25 Zhao et al. 11 reported that the mutation a615g was found in the CAS strain beside Beijing family. Other mutations were found scattering within the gidB gene, appearing in STRR MDR M. tuberculosis clinical isolates. Mutations in the gidB gene were found with 19 different mutations in 15.44% of the STRR MDR M. tuberculosis clinical isolates. Similar frequencies of mutations were found from Poland, 9 but higher than the findings from Thailand, 18 Myanmar, 39 and Beijing, China 11 (Table 4). Of the 19 mutations found, 17 were nonsynonymous, and the remaining two were deletion mutations. Interestingly, none STRS MDR M. tuberculosis clinical isolate here showed mutation in gidB gene. To the best of our knowledge, novel mutations with accession numbers, Y22D (MN645917), E24D (MN645918), A27P (MN645919), G34A (MN645920), L35P (MN645921), R43G (MN645922), C52R (MN645923), G76A (MN645924), L91R (MN645925), A119D (MN645926), R137W (MN645927), A138P (MN645928), V171G (MN645929), Y195H (MN645930), W45Stop, and c85del, were identified within gidB gene in STRR MDR M. tuberculosis clinical isolates. Some of them were accompanied with mutations either in rrs or rpsL gene. In contrast, the alteration in gidB L16R, A27P, 33 frameshift, G34A, L35P, W45Stop, A119D, R137W, occurred in STRR MDR M. tuberculosis clinical isolates without additional mutations in rrs or rpsL gene, which possibly play important roles in STR resistance.
Compared with the phenotypic data, the sensitivity for detecting STR resistance by DNA sequencing of rpsL was 72.48%, consistent with the data from 69.50% in Myanmar, 39 64.71% in Republic of Korea, 15 but lower than the findings from 78.26% in Beijing, China, 11 and higher than the findings from 24.64% in Spain, 23 50% in Poland, 9 63.63% in Thailand, 18 and 31.25% in Iran. 12 It can be presumed that the nature of mutations in the rpsL gene is highly related to different geographical regions and genotypes, which is similar with the earlier report that the tendency for acquiring DR mutations combats depending on lineages. 20 However, the combination of mutations in rpsL, rrs, and gidB improved the sensitivity to 96.64%, but unchanged the specificity (100.00%), similar with the data from Singapore, 25 Beijing, China, 11 and Latvia, 38 but higher than the findings from Spain, 23 Poland, 9 Mexico, 10 and Iran. 12 We deduced that the combination of mutations in the three genes rpsL, rrs, and gidB were the best current diagnosis predictors for STR resistance among STRR MDR M. tuberculosis clinical isolates. The combination of three mutations rpsL128 and 263 as well as rrs514 or rrs1401 showed the sensitivity of 79.87%, specificity of 100.0%, and accuracy of 86.24%, respectively, for the detection of STR resistance. Zhao et al. 11 reported similar findings. These three mutations rpsL128 and 263 as well as rrs514 or rrs1401 were also good diagnosis predictors of STR resistance among STRR MDR M. tuberculosis clinical isolates.
Conclusions
In summary, our study showed that the majority of STRR MDR M. tuberculosis clinical isolates (96.64%) were mutations in rpsL, rrs, and gidB genes which underscore their importance in the development of STR resistance. The most dominant mutations occurred at rpsL 128, 263, and rrs514 or 1401 position. Several novel mutations (6 mutations in rrs and 16 mutations in gidB) were also identified. The a1401g mutation in rrs gene was notably present in about 24% of MDR clinical isolates with cross resistance between STR and AMK. Thus, sequence analysis of these mutations likely helps to guide the use of STR (or perhaps another aminoglycoside) in the treatment of MDR-TB to achieve success and curtail transmission. Five STRR MDR M. tuberculosis clinical isolates had no known mutation within rpsL, rrs, and gidB genes. Therefore, these five STRR MDR M. tuberculosis clinical isolates could be attributed to find out mutations outside of the three genes or other resistance mechanism (e.g., drug efflux pumps).
Footnotes
Acknowledgments
The study is sponsored by Science and Technology Innovation Leader of Guangdong Province (2016TX03R095, to T.Z.), by CAS-TWAS President's PhD Fellowship Program (to M.M.I., and C.C.) and UCAS Fellowship Program (to H.M.A.H.) for international PhD students.
Disclosure Statement
No competing financial interests exist.
Authors' Contributions
Conceptualization, T.Z., M.M.I., and Y.T.; Methodology, M.M.I., H.M.A.H., and Zy.L.; Validation, C.C. and Zl.L.; Formal analysis, S.W., Xy.C., Y.L., and Y.G.; Investigation Xs.C. and L.G.; Writing—original draft preparation, M.M.I. and T.Z.; Writing—review and editing, X.L., S.T., J.L., W.W.Y., N.Z., and T.Z.; Supervision, T.Z.; Project administration, T.Z.; Funding acquisition, T.Z. All authors read carefully and approved the final article.
Funding Information
This work was supported by the National Mega-project of China for Main Infectious Diseases (2017ZX10302301-003-002) and for Innovative Drugs (2019ZX09721001-003-003), by Key-Area Research and Development Program of Guangdong Province (2019B110233003), by the Public Research and Capacity Building Project of Guangdong Provenience (2017A020212004). The founders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.