
Abstract
Helicobacter pylori and non-H. pylori Helicobacter (NHPH) are associated with gastritis, ulcer, and gastric neoplasia. Because of the impossibility to culture them, diagnosis remains based on microscopic examination and molecular analysis of biopsies. Owing to the lack of data concerning antibiotic resistance of NHPH, infected patients are usually treated using antibiotics, including clarithromycin. Herein, we describe, for the first time a human infection by Helicobacter suis harboring a mutation associated to clarithromycin resistance in H. pylori. Eradication was successful with a metronidazole-based treatment. This observation highlights the benefit to use genotypic detection of resistance to improve therapeutic management of NHPH infections.
Introduction
Since 1984,
As NHPH remain hardly cultivable, few data are available on their resistance to antibiotics. Moreover, as no guidelines on specific antibiotic treatment of NHPH exist, the usual treatment is empirically based on the reference treatment for H. pylori. 4 The standard therapy (amoxicillin and clarithromycin combined with a proton pump inhibitor [PPI]) has resulted in a good relief of symptoms and eradication of the bacterium in children. In contrast, in another reported case, treatment of NHPH infection by clarithromycin, metronidazole, and PPI in a patient with a duodenal ulcer disease had no effect, whereas treatment with metronidazole and tetracycline was successful. 5 From the latter, clarithromycin resistance could be suspected in NHPH. In H. pylori, clarithromycin resistance reaches almost 25% of strains in many countries and is the main risk factor for treatment failure. Clarithromycin resistance is due to a decrease in antibiotic binding to the bacterial ribosome due to three independent single nucleotide mutations within the 23S rRNA peptidyl transferase-encoding region that is, A2143G, A2142G, A2142C. 6 These resistances can be detected either by phenotypic or genotypic methods to adapt the clinical management to avoid therapeutic failures. The sequence similarity between the different Helicobacter species (7.5% sequence divergence on 23S rRNA gene between H. pylori and H. suis) suggests that the mechanism of action and resistance to clarithromycin in H. pylori should be identical in NHPH. 7 Therefore, because the determination of phenotypic resistance to clarithromycin in NHPH remains incompatible with a routine practice, due to the difficulties of culture, detection by molecular techniques of these mutations represents the main test used in routine diagnostic. We describe in this study a clinical case illustrating the benefit to use molecular diagnosis in these infections.
Clinical History and Phylogenic Analysis
A 43-year-old obese woman has beneficiated from a surgical treatment (subtotal gastrectomy, i.e., gastric sleeve). During her preoperative assessment, a gastrointestinal endoscopy was realized with gastric biopsies to detect infection by H. pylori. Fundic and antral gastritis were observed during endoscopy, confirmed by histological analysis (atrophic gastritis with moderate intensity and presence of very long and spiral-shaped bacilli). Bacteriological direct examination after Gram staining of biopsy smear found typically shaped bacilli suggestive of NHPH. Rapid urease test was performed onto the biopsy and was positive. Culture remained negative, even with 2 weeks of incubation on blood medium supplemented with antibiotics under microaerophilic conditions at 37°C. In front of this absence of culture, molecular analysis was performed after DNA extraction of biopsies (amplification of a 1,079 nucleotides-long 16S rDNA fragment). 8 During identification of the bacterial strain present in this biopsy, the more proximal cluster was H. suis (99% of identity). Systematic detection of clarithromycin resistance was performed by PCR (according to previously published method) and found a A2143G mutation associated to clarithromycin-resistant H. pylori. 9 To confirm the presence of a clarithromycin resistance associated mutation produced amplicons were then Sanger sequenced on ABI 3730 (Thermo Fisher Scientific, MA) (Fig. 1). 6 According to this result, patient's management consists in an association of PPI, amoxicillin, and metronidazole for a week (without clarithromycin). Efficacy of this eradication protocol was confirmed by the negativity of the 13 C urea breath test 6 weeks later (<1‰, mass spectrometry after ingestion of HELIKIT®, according to Mayoly Spindler recommendations).
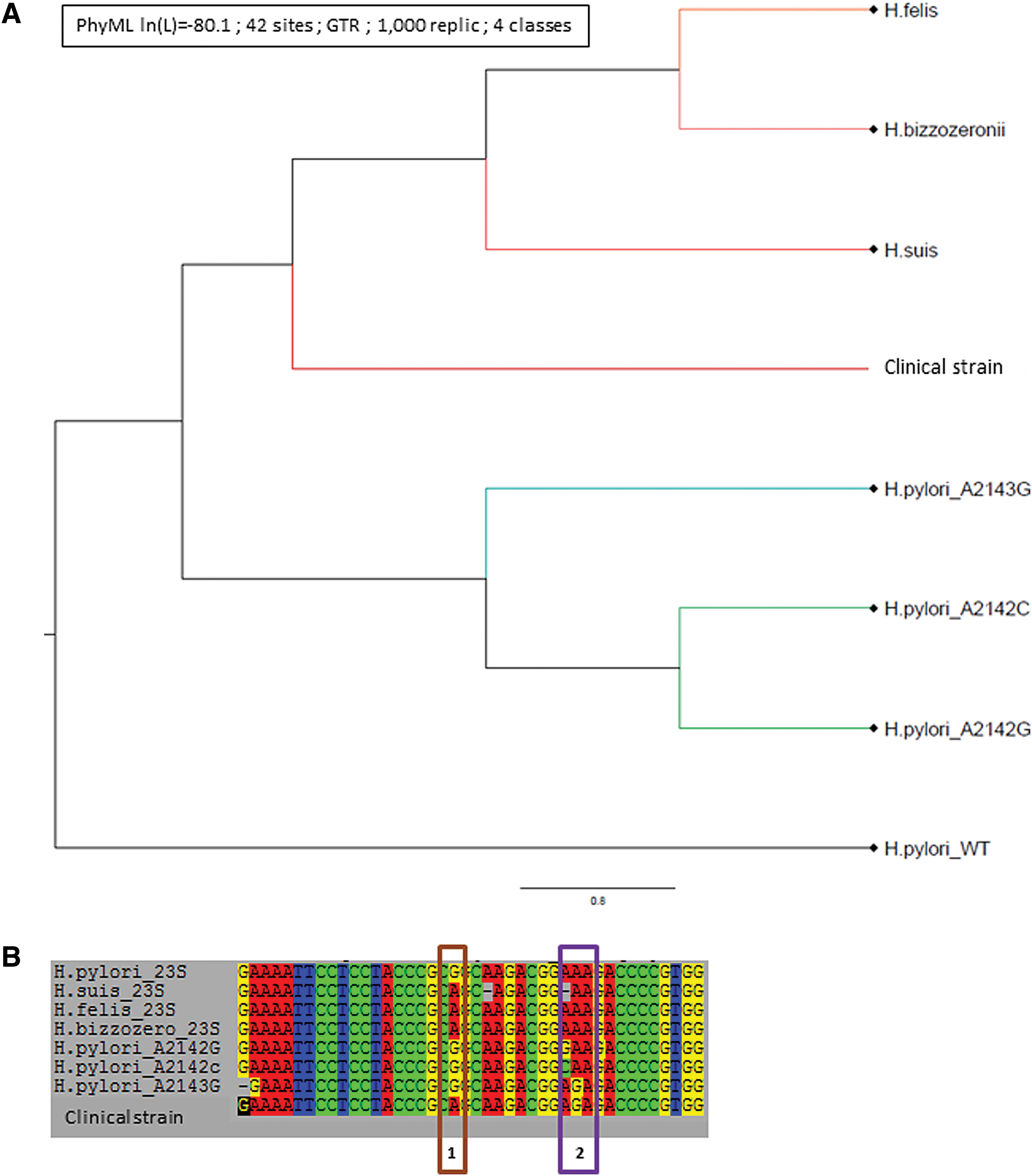
Phylogenic analysis of 23S genes of Helicobacter strains.
The produced sequence was retrospectively analyzed using SeaView Version 4.7 to compare the bacteria strain with the sequences published in the literature. Sequences were deposited onto GenBank (Accession number SAMN12273698).
Discussion
Herein we have described, for the first time in H. suis, the presence of a mutation in the 23s rRNA gene conferring clarithromycin resistance in H. pylori. 6 Even in the absence of direct antibiotic susceptibility testing, due to culture conditions, this genomic data suggested that this clinical strain is clarithromycin resistant. Indeed, initially extensively described in H. pylori, this mutation has also been described in a wide range of different bacterial strain, including gram-positive (Streptococcus, Staphylococcus, …), gram-negative (Enterobacteriaceae, Campylobacter, Neisseria, …) bacteria, but also acid-fast bacilli (Mycobacterium) or intracellular bacteria (Mycoplasma, …). This large repartition suggest that this resistance mutation and mechanism could be almost universal. 10 Indeed, these nucleotides are implicated in the secondary structure of the 30 regions of 23S ribosomal RNA (rRNA) domain V., and described mutations could yield 14/15-membered, 16-membered macrolide, and/or ketolide resistance.11,12
Although the clinical consequences have not been evaluated yet (due to the low prevalence of this mutation), published data on H. pylori have led us, by analogy, not to treat the patient using clarithromycin. In the present case and even if some studies observed a lack of sensitivity for the 13 C urea breath test in infection by H. suis, the patient's results are far below the threshold (<1‰ for a cutoff value of 4‰), indicating a probable success for bacterial eradication. 13 As described and because of the difficulty to efficiently culture NHPH, identification and quantification of resistance to clarithromycin by phenotypic methods remain impossible for routine diagnostic purposes. In this context, genotypic detection of mutations (identified in H. pylori) is the unique possible test in NHPH. This detection has a real impact in the therapeutic management of NHPH-infected patients. Indeed, if these patients represent a small percentage of Helicobacter-infected patients, a potential evolution to gastric ulcer or gastric MALT lymphoma must be considered.
According to the national report of the antibiotic use in veterinary medicine, in France, in 2017, even considering a dramatic decrease, macrolides is the fourth antibiotic family use in swine breeding. This wide use could explain the emergence of NHPH clarithromycin resistance and strengthen the concept of “One Health” in antibioresistance for veterinary and human medicines.
Footnotes
Acknowledgment
The authors thank Jeffrey Ashram for his extensive reviewing of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a grant from the Groupement Interrégional de Recherche Clinique et d'Innovation Sud-Ouest Outre-Mer Hospitalier (APIK-2018).