
Abstract
Background:
Infectious complications (IC) caused by bacterial strains often impede anticancer therapy. The study aimed to retrospectively analyze bacterial IC that could help predict the risk and optimize the empirical treatment for bacterial infections in pediatric cancer patients.
Patients and Methods:
Over a 72-month period, all-in 5,599 children with cancer: 2,441 patients with hematological malignancy (HM including acute leukemias, Hodgkin and non-Hodgkin lymphomas [NHLs], and Langerhans cell histiocytosis) and 3,158 with solid tumors (STs including central nervous system tumors, neuroblastoma, Wilms' tumor, soft tissue sarcoma, germ cell tumors, Ewing sarcoma, osteosarcoma, hepatoblastoma, and others) were enrolled into the study. Episodes of bacterial infectious complications (EBICs) confirmed by microbiological findings were reported by each hospital and analyzed centrally.
Results:
At least 1 EBIC was diagnosed in 2,155 (36.8%) children (1,281 [59.4%] with HM and 874 [40.6%] with ST; p < 0.001). All-in 4,860 EBICs were diagnosed including 62.2% episodes in children with HM and 37.8% in children with ST (p < 0.001). Having analyzed the source of infections, blood stream infections predominated, apart from NHL patients in whom the most common type was gut infections. The profile of bacteria strains was different in HM and ST groups (p < 0.001). However, in both groups the most common Gram-negative pathogen was Enterobacteriaceae, with the rate being higher in the HM group. Among Gram-negative strains low susceptibility to ceftazidime, whereas among Enterococcus spp. low susceptibility to vancomycin was noticed. The rate of multidrug-resistant (MDR) pathogens was high, especially for Gram negatives (47.7% vs. 23.9%; p < 0.001). The survival after infections was comparable for HM and ST patients (p = 0.215).
Conclusions:
The risk of bacterial IC in HM patients was higher than in the ST group. The high rate of MDR strains was detected in pediatric cancer patients, especially in those with HM.
Background
Chemotherapy for cancer in children is one of the most intensive treatment modalities in medicine. Therefore, infectious complications (ICs) are an important cause of treatment-related morbidity and mortality in this group of patients, despite prophylactic measures. 1
Children with malignancies, both hematological ones and with solid tumors (STs), are exposed to viral, bacterial, and fungal infections owing to an impairment of immune system resulting from the disease itself and from intensive chemotherapy. The majority of IC is caused by invasive bacterial infections (BIs). Thus, aggressive approach based on prompt in-hospital evaluation, diagnostic procedures, and administration of broad-spectrum intravenous antibiotics have been universally recommended. Although empirical antibiotic therapy reduces mortality, it also results in an increasing problem of drug-resistant strains among both Gram-negative and Gram-positive bacteria.2,3 Finally, a group of six multidrug-resistant (MDR) organisms against which limited therapeutic options were available, was labeled ESKAPE pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp.). 4 The problem of MDR bacteria is extremely important in patients with profound, long-lasting neutropenia treated with intensive chemotherapy, as is the case in cancer patients. These pathogens are usually resistant to standard empirical treatment and in severely immunocompromised patients may easily lead to a life-threatening infection or even death. 5 However, infections etiology varies with cancer type, chemotherapy regimen, and evolves over time. 6 The knowledge of the current prevalence, types, and risk factors related to different malignancies and clinical outcomes will allow for determination of optimal prevention and empirical treatment strategies.
The aim of this study was to evaluate the prevalence, epidemiology, profile of microbial strains, and types of BIs and its susceptibility patterns in pediatric cancer patients with hematological malignancies (HMs) and STs in Polish pediatric hematology and oncology centers over a 6-year period.
Patients and Methods
Patients
From January 1, 2012 to December 31, 2017 all-in newly diagnosed 5,599 children and adolescents <18 years treated for cancer in Polish pediatric hematology and oncology centers were enrolled into the retrospective study. All patients were treated according to currently used chemotherapy regimens. Children undergoing hematopoietic stem cell transplantation were censored at the day of transplantation.
Uniform, standard antimicrobial prophylaxis was applied to all patients, including co-trimoxazole (15 mg/kg p.o. three times weekly) against Pneumocystis jiroveci and nonpharmacological prophylaxis, that is, hand hygiene before contact with the patient, use of maximal sterile barrier precautions with central line placement, and prompt removal of lines when they are no longer necessary.7,8 When clinical symptoms suggesting infection occurred, laboratory and microbiological tests (blood cultures and cultures from other sites, that is, from skin lesions, urine, stool if focal signs, and/or symptoms were present) were performed and empirical antibiotic therapy was started immediately. 9 Changes in antibiotic regimens, mostly caused by persistent fever or infectious parameters, were made according to antibiograms or according to empirical intensified antibiotic treatment strategies.
Methods
Episodes of bacterial infectious complications (EBICs) were retrospectively annually reported by each hospital and data were analyzed centrally. Standard-of-care diagnostic tests, including collection of microbiological samples (blood cultures, urine cultures, and soft tissue swabs), were ordered at the discretion of treating physicians. Only patients with clinical symptoms of infection confirmed by microbiological finding (microbiologically documented infections) were enrolled in the study. All microbiological findings in patients without clinically documented infection were excluded from the analysis. Isolated strains were divided into Gram-positive (Clostridiaceae, Enterococcaceae, Staphylococcaceae, and Streptococcaceae) and Gram-negative (Enterobacteriaceae, Pseudomonadaceae, i.e., P. aeruginosa, Moraxellaceae, i.e., Acinetobacter spp.) bacterial families. The analyzed BIs were divided into clinical types: bloodstream infections (BSIs), defined as one or more positive blood cultures associated with systemic signs of infection 10 ; gut infections (GIs), defined as the onset of loose stools the severity of which prompted health care providers to initiate a diagnostic evaluation 9 ; urinary tract infections (UTIs), being the presence of localized genitourinary symptoms and a urine culture with an identified urinary pathogen; and skin and soft tissue infections (SSTIs), being microbiologically confirmed infections of the layers of the skin and underlying soft tissues. 11 Clostridium difficile infection (CDI) required a positive stool test result for toxigenic C. difficile or its toxins in patient with diarrhea. Bacterial strains were subjected to in vitro antibiotic susceptibility testing with disk diffusion method and interpreted as per European Committee on Antimicrobial Susceptibility Testing (EUCAST) recommendations. Any isolate that exhibited acquired resistance to at least one agent in three or more antimicrobial categories was defined as MDR. The analyzed mechanisms of antibiotic resistance included ESBLs (extended-spectrum β-lactamases: bacteria-producing ESBL), MBL (metallo-β-lactamase-producing bacteria detected by phenotypic-based method), AmpC (AmpC β-lactamases: bacteria-producing chromosomal cephalosporinase AmpC type detected by disk diffusion method using ceftazidime, cefotaxime, and ceftriaxone), KPC (K. pneumoniae carbapenemase, Enterobacteriaceae or Pseudomonadaceae-producing carbapenemase KPC type detected by phenotypic-based method), MRS (methicillin-resistant staphylococci), HLAR+ (high-level aminoglycoside resistance in Enterococci detected by growth-based assays), or VRE (vancomycin-resistant Enterococci). 12 In all malignancy types, the index of bacterial infection (IBI) was calculated as a ratio of patients with at least one BI to all patients diagnosed with this disease in an analyzed period of time. 5
Statistics
Data were analyzed using Statistica Package ver. 10 (StatSoft Poland). Two-sided p < 0.05 were considered significant. Categorical variables were compared with chi-square test or Fisher's exact test depending on the number of episodes per comparison group. Continuous variables following a non-normal distribution were described as median with interquartile ranges and compared using the Mann–Whitney U test for two groups or Kruskal–Wallis test for more than two groups. Time to infection was defined as a time from the day of cancer diagnosis to the day of infection manifestation. The Kaplan–Meier method was used to determine infection-related mortality (IRM) and probability of overall survival (pOS). IRM was defined as death that could be attributed to ICs of either an immediate or underlying cause. The pOS was defined as the observed probability of surviving after cancer diagnosis in patients diagnosed with IC.
Results
Demographics
During the 72-month study period, 5,599 patients with cancer were subdivided according to underlying disease into HM group (n = 2,441; 43.6%): acute lymphoblastic leukemia (ALL; n = 1,289; 23.0%), acute myeloid leukemia (AML; n = 250; 4.5%), non-Hodgkin lymphoma (NHL; n = 352; 6.3%), Hodgkin lymphoma (n = 371; 6.6%), Langerhans cell histiocytosis (n = 113; 2.0%), and other (n = 66; 1.2%); and ST group (n = 3158; 56.4%): central nervous system tumors (CNS-T; n = 1,082; 19.3%), neuroblastoma (NBL; n = 485; 8.7%), Wilms tumor (WT; n = 314; 5.7%), soft tissue sarcoma (STS; n = 236; 4.2%), germ cell tumors (n = 205; 3.6%), Ewing sarcoma (n = 80; 1.4%), osteosarcoma (OS; n = 71; 1.3%), hepatoblastoma (HBL; n = 61; 1.1%), and other (n = 624; 11.1%).
Prevalence
IC occurred in 2,155 children (38.5%; 956 girls, 1,199 boys) at age 0.01–19.1 (median = 5.1) years, including 1,281 (52.5%) with HM and 874 (27.7%; p < 0.001) with ST. Among HM patients suffering from BIs those with ALL prevailed—805/1,289 (62.5%), of newly diagnosed ALL patients, AML—178/250 (71.2%), and NHL—180/352 (51.1%), whereas others were less commonly observed. Within ST group with BI patients treated for CNS-T—267/1,082 (24.7%), NBL—169/485 (34.8%), and STS—150/236 (63.6%) predominated (Table 1). Of all children diagnosed with BI during anticancer therapy, 1,146 (53.2%) had one episode, 409 (19.0%) had two, 263 (12.2%) had three, 132 (6.1%) had four, and 205 (9.5%) had five or more episodes during the study.
Incidence of Bacterial Infections According to Cancer Type
p-Value compares hematological malignancies and solid tumors group.
ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; BI, bacterial infections; CNS-T, central nervous system tumors; ES, Ewing sarcoma; GCT, germ cell tumors; HBL, hepatoblastoma; HD, Hodgkin lymphoma; IBI, index of bacterial infection; LCH, Langerhans cell histiocytosis; NBL, neuroblastoma; NHL, non-Hodgkin lymphoma; OS, osteosarcoma; STS, soft tissue sarcoma; WT, Wilms' tumor.
Frequencies
In the studied group of 2,155 cancer patients, 4,860 EBICs were diagnosed including 3,022 (62.2%; median = 2.4 episodes of BI per patient; IBI was 0.5) episodes in children with HM and 1,838 (37.8%; median = 2.4 episodes of BI per patient; IBI was 0.3) in children with ST (p < 0.001).
Among 805 ALL patients with at least one BI, there were 1,844 EBICs (median = 2.3 episodes per patient with BI; IBI = 0.6), whereas within 178 AML patients there were 547 EBICs (median = 3.1 episodes; IBI = 0.7) and in the NHL group of 180 patients there were 380 EBICs (median = 2.1 episodes; IBI = 0.5).
Of 267 patients with CNS-T, diagnosed with at least one BI, 620 EBICs occurred (median = 2.3 episodes per patients with BI; IBI was 0.25). Within the NBL group, there were 368 episodes in 169 patients (median = 2.2 episodes; IBI = 0.35), whereas in the STS group there were 340 EBICs in 150 patients (median = 2.3 episodes; IBI = 0.64) (Table 1).
Time to infection
Median time to development of Gram-positive and Gram-negative BI was significantly different in HM and ST groups (p < 0.001), that is, 98 days to Gram-positive and 131 days to Gram-negative infection in the HM group versus 170 days to Gram-positive and 163 days to Gram-negative infection in the ST group. The summary of median time to various BIs is presented in Table 2.
Time to Bacterial Infections Episodes Caused by Different Bacteria with Respect to Underlying Cancer Type
Significant differences are given in bold.
Sites of BI
According to the source of BI in the analyzed group, BSI 1,895 of 4,860 (39.0%) and GI 1,516 of 4,860 (31.2%) episodes predominated, whereas UTI were found in 1,037 of 4,860 (21.3%) and SSTI only in 184 of 4,860 (3.8%) episodes. Other isolation sites were responsible for 228 of 4,860 (4.7%) BI episodes. The isolation sites were different in the HM than in the ST group (p < 0.001) and are summarized in Table 3. The most common isolation sites in the HM group were BSI 1,227 of 3,022 (40.6%) and GI 1,024 of 3,022 (33.9%), whereas in the ST group also BSI 668 of 1,838 (36.3%) and UTI 497 of 1,838 (27.0%) was reported. Contrary to the rest of the analyzed group, in NHL patients the most common type of infection was GI, but not BSI (38.2% and 31.5%, respectively) like in other HM patients, where BSIs were predominant. Similarly, within the ST group only in WT patients the most common site of infection was GI, not BSI (37.8% and 28.9%, respectively).
Type of Bacterial Infection Episodes According to Cancer Type
BSI, bloodstream infection; EBIC, episodes of bacterial infectious complication; GI, gut infection; SSTI, skin and soft tissue infection; UTI, urinary tract infection.
Profile of bacterial strains
In the analyzed cohort of patients, the profile of bacterial strains was different in the HM and ST groups (p < 0.001). In both groups, the most common Gram-negative pathogen was Enterobacteriaceae, but the rate was higher in the HM group (46.5% vs. 41.4%). The predominant strain of Gram-positive bacteria in both groups was Staphylococcaceae, with a higher rate in the ST group (22.1 vs. 17.9%). The second most common Gram-negative pathogen was Pseudomonadaceae found in 7.3% of isolates in the HM group and in 6.2% of isolates in the ST group. Other commonly diagnosed Gram-positive pathogens were Clostridiaceae (12.7% in HM and 15.1% in ST group) and Enterococcaceae (7.3% and 6.3%, respectively). The summary of all diagnosed pathogens in different subgroups of cancer patients is given in Table 4 and the profile of selected bacterial strains in Table 5.
Profile of Bacterial Infections According to Cancer Type
Bacterial Pathogens Found in Cancer Patients by Site of Isolation
Antibiotic susceptibility pattern
The antimicrobial sensitivity pattern of Gram-positive and Gram-negative bacterial strains in both HM and ST patients is given in Table 6. Susceptibility of Gram-negative strains to ceftazidime was low, especially among Enterobacter spp. (36.2% in HM and 52.8% in ST patients), Klebsiella spp. (40.6% in HM and 52.0% in ST), and Acinetobacter spp. (54.5% in HM and 68.8% in ST). The sensitivity rates of all Gram-negative bacteria to amikacin and meropenem were high, with no major differences between HM and ST patients. Most bacteria among Enterobacteriaceae were sensitive to meropenem. However, meropenem resistance has emerged in P. aeruginosa (24.1% in HM and 20.0% in ST) and Acinetobacter spp. (20.8% in HM and 31.2% in ST). Gram-positive bacteria, especially Enterococcus spp. and coagulase-negative Staphylococci were often resistant to many antibiotics, including penicillin and ampicillin. However, none of coagulase-negative Staphylococci and Streptococcus spp. was resistant to vancomycin, whereas Enterococcus spp. were only moderately susceptible to vancomycin, that is, 49.6% in HM and 65.8% in ST patients and S. aureus found in HM patients was highly vancomycin resistant, that is, 54.5%.
Antibiotic Sensitivity Pattern of Gram-Negative (A; C) and Gram-Positive (B; D) Strains in Hematological Malignancies (A; B) and Solid Tumors (C; D) Patients
MDR pathogens
The rate of MDR pathogens was significantly higher for Gram-negative than Gram-positive strains (47.7% vs. 23.9% respectively; p < 0.001). For all isolates, MDR bacteria were more often found in HM than in ST group, that is, 27.3% in HM versus 19.0% in ST group were Gram positive (p = 0.001) and 51.2% in HM versus 40.8% in ST group were Gram negative (p = 0.002). In the HM group, within 350 EBICs caused by MDR Gram-positive strains, MRS+ (66.0%) strains and VRE+ (21.1%) or HLAR+ (8.6%) Enterococci predominated. Within 895 MDR Gram-negative EBICs, the most common were ESBL+ (82.9%) or AmpC+ (9.7%) Enterobacteriaceae and MBL+ (4.7%) Enterobacteriaceae or Pseudomonadaceae. In the ST group, 167 MDR Gram-positive bacteria were found including MRS+ (72.5%) Staphylococci and VRE+ (18.0%) Enterococci. In 391 MDR Gram-negative episodes, ESBL+ (79.3%) or AmpC+ (14.8%) Enterobacteriaceae and KPC-producing (3.3%) Pseudomonas (Fig. 1) predominated.
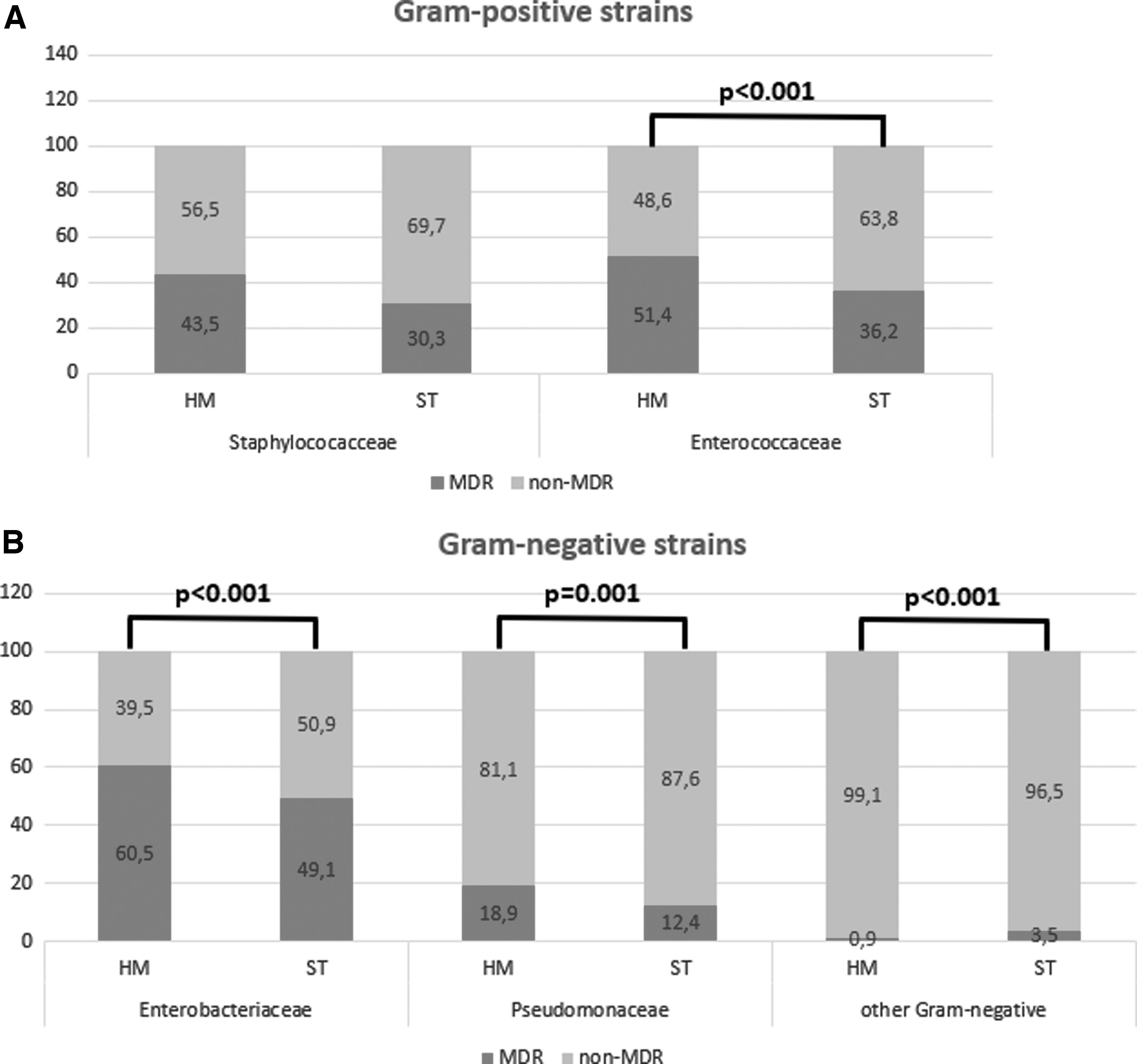
Rate of MDR strains in different bacterial infections.
Survival of pediatric cancer patients with IC
Thirty-day IRM during the 6-year study period was 4.5% and was comparable for HM and ST groups (4.2% and 4.9%, respectively; p = 0.529). Five-year pOS of cancer patients with BI was 88.1 ± 0.1% and was comparable for both cancer groups, that is, 91.5 ± 0.9% for HM and 83.5 ± 1.5% for ST group (p = 0.215).
Discussion
Studies addressing ICs associated with pediatric malignancies other than acute leukemias are very limited. This study evaluated ICs in 2,155 patients, including 1,281 treated for HM and 874 treated for ST over a 6-year period. To the best of our knowledge, this is the largest cohort of children and adolescents treated for cancer providing characteristics of BIs. Even if the study design was unique, some comparisons with other studies are possible.
In general, our study suggests that the frequency of bacterial IC in our retrospective cohort was high, especially when compared with adult cohort, but similar to other childhood cohorts reported in the literature,6,9,13–15 especially for HM group. In the study, we found IBI of 0.5 for HM group and 0.3 for ST group. As expected, the incidence and rate of EBICs was the highest in AML patients, followed by ALL patients. There are articles proving that IC in adult cancer patients with HM differ from those with ST and the frequency of EBICs, especially BSI, is lower in patients with ST than with HM. 16 Similarly, we found that the prevalence and frequency of IC was significantly lower in the ST group compared with the HM group.
Similar to the data from other studies,17–19 our results confirmed that the most common type of infection found in our cohort was BSI. One-third (39.0%) of all patients in our cohort developed at least one BSI during the therapy. It appears that line care efforts and the line maintenance bundles did not reduce the risk of BSI. This is supported by the fact that only half of the pathogens that caused BSI in our population were traditional skin bacteria. In contrast, the rest of bacterial strains identified in BSI of our patients were bacteria commonly found in the oral cavity and gastrointestinal tract. These findings highlight and support the hypothesis that the origin of BSI may be the translocation of bacteria across the mucosal barriers damaged by cytotoxic chemotherapy regimens. 17
Enteritis was the second most common type of EBIC in our study. However, in NHL and WT patients GI, rather than BSI, prevailed. It is related to the etiological spectrum of these illnesses that is unique to the population of younger children. 9 Nevertheless, both Enterobacteriaceae and Clostridiaceae originate from GI following mucositis and may result from the administration of systemic broad-spectrum antibiotics causing damage to the normal enteric microbiome and leading to reduction in microbial diversity. 15 Our data provide new insights into incidence of GI in pediatric cancer patients and stress the need for caution in the usage of broad-spectrum antibiotics.
Our principal result was to identify the etiology of MDI in our cohort. Unlike the other studies considering ICs mainly in HM patients,20–22 we found Gram-negative strains, especially Enterobacteriaceae, but not Gram-positive agents, the most common bacterial pathogen responsible for EBIC, especially GI, in all cancer patients. Similar results were reported by Caniza et al. and explained by the exposure to broad-spectrum antibiotic therapy causing a shift in the normal flora to pathogenic Gram-negative bacteria especially in children with chemotherapy-induced mucositis, which disrupts the anatomic barrier of the mucosa and allows entry of microorganisms to the submucosa. 23
In our study, Gram-positive bacteria predominated only in selected patients with ST, that is, NBL, WT, and HBL. In these patients, we also noticed a higher rate of CDI than in other subgroups, which is the reason for Gram-positive predominance. It is possibly related to the younger age of patients with this cancer type, whereas younger age is also regarded to be an important risk factor of CDI. 24 The type of malignancy and applied chemotherapy can also influence a predisposition for CDI; however until now, no clear relationship between the type of cancer and the risk of CDI has been described.24,25
Of interest, we found a higher rate of Streptococcal infections, mainly BSI, in AML patients than in all other groups. It is especially important owing to intensity of AML chemotherapy with expected chemotherapy-induced neutropenia of >7 days and Gram-positive prophylaxis recommendations, which are not standardized. 1 The incidence of Streptococcaceae infections is significantly higher after therapeutic regimens that included high-dose cytarabine. Furthermore, Streptococcal bacteremia occurred more often during episodes of neutropenia. 26 Both, treatment with high-dose cytarabine and severe prolonged neutropenia, occur in AML patients.
In the study, we also examined the spectrum of susceptibility patterns of Gram-negative and Gram-positive strains. High level of resistance in Gram-negative bacteria was noted for third-generation cephalosporines and piperacillin-tazobactam, whereas these antibiotics represent the first-line empirical therapy for febrile neutropenia in our antibiotic policy. On the contrary, aminoglycosides and carbapenems had good activity, but the level of resistance to these agents can only increase as their use has been on the rise. The situation with P. aeruginosa and Acinetobacter spp. is especially grim because of a decreased rate of susceptibility to meropenem. Among Gram-positive bacteria almost all excluding Enterococcus spp. and S. aureus found in HM patients were sensitive to vancomycin. However, empirical use of vancomycin in case of prolonged neutropenic fever is not recommended and should only be used in cases when a Gram-positive infection is suspected.
The most important observation is that the overall proportion of resistant strains was 37.1% for all cancer patients, including those with ST. Growing antimicrobial resistance, especially among Gram-negative strains, has emerged as a serious threat to children with cancer. 27 The MDR BIs have limited therapeutic options, whereas their rate among infection etiologies is rising. 28 Given high incidence of BI and high mortality associated with Gram-negative pathogens in hematology patients, the impact of antibiotic resistance is particularly worrisome in this setting. 29 In our study, despite the higher rate of MDR strains among HM than among ST patients, the profile of resistance was comparable including ESBL/AmpC/MBL Enterobacteriaceae, VRE Enterococci, and MRS Staphylococci labeled as ESKAPE pathogens. However, reported antimicrobial resistance rates are higher than given in the literature.6,30 The ECIL-4 review reported than a median 34% of Enterobacteriaceae were ESBL producers, ranging from 16% to 44% in different countries. 30 It is well proven that MDR pathogens are significantly more likely to be resistant to empirical antibiotic therapy applied in cancer patients.
Of interest, we found a relatively early occurrence of IC caused by Pseudomonadaceae in patients with ST compared with other Gram-negative and also Gram-positive bacteria. It may be associated with high-intensity chemotherapy protocols used in pediatric ST patients that result in longer periods of severe neutropenia and longer duration of hospitalization, whereas P. aeruginosa infections are usually hospital-acquired ones. 31
The limitations of this study include its retrospective nature and the fact that we enrolled only MDI, without only clinically confirmed infections or fever of unknown origin, whereas etiology of BI is usually proven in BSI, but significantly less frequently found in pneumonia or typhlitis. The study has important strengths. It is the first nation-wide study focusing on all MDI bacterial ICs in all cancer patients, including not only HM but also comparable number of ST ones, underrepresented in the literature. Moreover, the large sample size enables unique analysis and makes our data more applicable to other PHO centers. Contrary to many studies, we analyzed all identified bacterial strains, rather than focusing on specific pathogen or infection site. In case of the absence of local epidemiological data, our results may be used to optimize the prophylactic strategies and effective empirical therapies in different groups of pediatric cancer patients.
Conclusions
To conclude, our study suggests that the incidence of IC in our retrospective cohort of pediatric cancer patients was as high as previous epidemiological studies reported. In addition, patients with HM are at a higher risk of bacterial IC that those with ST. In our cohort, Gram-negative pathogens were predominant, whereas blood stream infections were the most frequent type of MDI. The alarming rate of MDR bacteria, especially within Gram-negative strains, is the major concern for children with cancer.
Footnotes
Authors' Contributions
O.Z.S., J.W., and J.S. were responsible for concept of study and design. O.Z.S. was major contributor in writing the article. All authors contributed toward data collection, data analysis, critical revision of the article, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Availability of Data and Material
The datasets generated and analyzed during this study are not publicly available but are available from the corresponding author on reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.