
Abstract
The aim of this work was to assess the prevalence of carbapenemase-producing and extended-spectrum β-lactamase-producing Enterobacterales (ESBLPE) intestinal carriage among private dwelling residents (PDR) and nursing home residents (NHR) from the catchment area of Hospital Verge de la Cinta (Tortosa. North-Eastern Spain), and to depict clinicoepidemiological features of colonized individuals. Prevalence of ESBLPE carriage amid 762 PDR (0–94 years) who had feces collected for routine culture was 7.3% and 31% among 71 NHR (68–98 years) screened upon hospital admission. The mean age of colonized and noncolonized subjects was 30 and 32.8 years in PDR (p = 0.58) and 85 and 87 years in NHR (p = 0.32). The predominant ESBLPE was CTX-M-15-producing Escherichia coli (42.8% in PDR and 68.2% in NHR [25% and 86.7% belonging to O25b-ST131 clone; p < 0.0001]), followed by CTX-M-9-group- and SHV-producing E. coli and by CTX-M-15-producing Klebsiella pneumoniae. Overall, 72.7% of ESBLPE were multidrug resistant and 46.2% carried transferable quinolone determinants. Institutionalization in a nursing home was a risk factor for ESBLPE and extended-spectrum β-lactamase (ESBL)-producing O25b-ST131 E. coli carriage in individuals over 67 years (odds ratio 7.7 and 14.1). Previous antibiotic use and skin ulcers were significantly associated with ESBLPE carriage in NHR. Age <25 years in PDR and amoxicillin/clavulanate exposure in NHR protected against ESBL-producing O25b-ST131 E. coli colonization. Only two PDR, with known risk factors, bore OXA-48-producing isolates. These results highlight the role of nonhospitalized intestinal carriers, particularly NHR, as ESBLPE reservoirs and the preponderance of CTX-M-15, mainly linked to O25b-ST131 clone, as well as the emergence of carbapenemase-producing Enterobacterales carriers.
Introduction
Infections caused by extended-spectrum β-lactamase (ESBL)-producing Enterobacterales (ESBLPE) and, to a lesser extent, by plasmid-encoded carbapenemase (PC)-producing Enterobacterales (PCPE) are increasingly reported not only in health care settings but also in the community.
Emergence of ESBLPE and PCPE is of major concern, since ESBL and PC confer resistance to broad-spectrum cephalosporins and carbapenems, drugs of choice in the empirical therapy of severe infections produced by Enterobacterales and because the genes codifying them may be transmitted horizontally.1,2 Moreover, as these genes are often located in genetic platforms together with other resistance genes, most ESBLPE and PCPE strains display coresistance to non-β-lactam antibiotics, complicating the treatment of common infections, such as urinary tract infections. 3
The increasing occurrence of ESBLPE in the community, which has been observed since 2000, coincided with the emergence of CTX-M enzymes, first recognized in Europe and South America, which nowadays are the predominant ESBL worldwide and have replaced TEM and SHV variants. 4 Although the distribution of different CTX-M-type enzymes seems to show a certain regional specificity, international travel, immigration, the presence of blaCTX-M genes in highly mobilizable genetic platforms and the existence of these platforms within epidemic high-risk successful clones may have contributed to the universal dissemination of some CTX-M ESBLs. 5
One particularly interesting case is the global rise of CTX-M-15-producing Escherichia coli isolates, which has been mainly attributed to the international spread of O25b-ST131 clone, first described in 2008, and which has become the predominant lineage among extraintestinal pathogenic E. coli isolates. O25b-ST131 E. coli isolates, unlike other extraintestinal isolates belonging to the phylogenetic B2 group, are almost always resistant to fluoroquinolones and often produce ESBL (specially CTX-M-15). In addition, they harbor a number of virulence genes and have been involved in a great variety of community- and health care-acquired infections. 6
Regarding PCPE, they constitute the last and most worrying threat to the effectiveness of antimicrobials. Their emergence seems to be consequence of the generalized use of carbapenems to treat infections caused by ESBLPE. As with ESBLs, the distribution of different PC exhibits great geographic heterogeneity. In Spain, the most prevalent enzyme is OXA-48 and the current epidemiological status corresponds to an endemic situation with interinstitutional and interregional transmission. OXA-48, which was originally identified in Turkey in 2001, has spread worldwide since then, particularly in Asia, North Africa, and Middle East, and is detected predominantly in Klebsiella pneumoniae.7,8 OXA-48 coexists, not seldom, with CTX-M-15, and its dissemination has been facilitated by the location of blaOXA-48 within Tn1999 on a self-conjugative IncL/M plasmid. 8
The gastrointestinal tract is the main reservoir of Enterobacterales and an ecological niche which provides a favorable environment for the interchange of resistance genes between bacteria. 9 Many of the infections due to ESBLPE and PCPE are endogenous and are preceded by intestinal carriage of these multiresistant microorganisms,10–14 but the frequency of community fecal carriers and of circulating enzymes shows a large geographical variability9,15 and recent studies tackling this issue in Spain are scarce.16–20
The aim of this work was to assess the prevalence of intestinal carriers of ESBLPE and PCPE, and particularly of E. coli belonging to the O25b-ST131 clonal group, among nonhospitalized private dwelling residents (PDR) or nursing home residents (NHR) in the Health Region of Terres de l'Ebre (Catalonia. Spain), as well as to determine the involved enzymes and the concomitant antimicrobial resistances and to gain insights into the clinical and epidemiological features of colonized individuals.
Materials and Methods
Study design, setting, and patients
This prospective prevalence survey was conducted between the October 1, 2016 and the March 31, 2017 at the Microbiology Laboratory of Hospital de Tortosa Verge de la Cinta (a second-level public teaching hospital with 215 beds situated in the city of Tortosa-South Catalonia, Spain). This laboratory provides assistance to patients attending either the referral hospital or any of the 35 associated primary health care centers of the Health Region Terres de l'Ebre (∼180,000 citizens).
Seven hundred sixty-two PDR (mean age 32 years; range 0–94 years; 53.3% females) whose feces were submitted to the microbiology laboratory for routine stool culture due to suspected gastrointestinal infection and 71 NHR (mean age 86.5 years; range 68–98 years; 70.4% females), from whom rectal swabs were collected <24 hours upon their admission to hospital to screen for multidrug-resistant organisms, according to the standing protocols, were included in the study.
Data for interesting clinical and epidemiological variables from all NHR and from colonized PDR, who provided informed consent, were obtained from their clinical records and from personal interviews with the aid of a structured ad-hoc questionnaire. The current study was approved by the Institutional Review Board of the Hospital.
Microbiological methods
Fecal samples and rectal swabs were seeded onto the selective chromogenic media CHROMagar ESBL biplate (BBL) and CromID CARBA SMART Agar (CARB/OXA; bioMérieux, Marcy l'Étoile, France). Rectal swabs were also inoculated into thioglycolate enrichment broth (bioMérieux) and were subcultured on chromogenic agar plates after overnight incubation. Colonies growing on any of the chromogenic media were further identified at species level using matrix-assisted laser desorption/ionization-time of flight mass spectrometry (Bruker-Daltonics) and were subjected to antimicrobial susceptibility testing employing commercial broth microdilution panels (MicroScan; Beckman) and gradient strips (E-test; bioMérieux), whose results were interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines.
Presumptive phenotypic detection of ESBL was assessed by the double-disk synergy test performed with amoxicillin/clavulanic acid disks placed 30 mm apart from cefotaxime, ceftazidime, cefepime, and aztreonam disks in all isolates showing decreased susceptibility to broad-spectrum cephalosporins
ESBL and PC genotypic characterization was accomplished by conventional polymerase chain reaction (PCR) using specific primers for blaTEM, blaSHV, blaCTX-M, blaVIM, blaKPC, blaNDM, blaOXA-48, and blaIMP and subsequent sequencing.21,22 Investigation of blaGES, blaVEB, blaBEL, blaPER, and blaSFO was performed at the National Reference Laboratory on Antimicrobial Resistance (Centro Nacional de Microbiología. Instituto de Salud Carlos III) 23 in the only isolate that was presumptively classified as ESBL producer and was negative for CTX-M, SHV, and TEM-type ESBLs. Detection of blaOXA-1 in all isolates and of transferable quinolone resistance determinants in those with a ciprofloxacin MIC above the ecological cutoff value proposed by EUCAST (0.064 mg/L for E. coli and 0.125 mg/L for K. pneumoniae) was carried out by PCR (blaOXA-1, qnrA, qnrB, qnrS) or PCR followed by sequencing (aac (6′)-Ib-cr). 24
Ascription of E. coli isolates to O25b-ST131 clone was performed by the allele-specific PCR described by Clermont et al. 25
Statistical analysis
The results of categorical variables were expressed as percentages and their corresponding 95% confidence interval (CI), and those of quantitative variables as measures of central tendency (mean) and dispersion (standard deviation [SD]). Differences in proportions and between means were compared using either the chi-square test or Fisher's exact test and the Student's t test, respectively, and were considered significant when p ≤ 0.05. The association between eventual risk factors and colonization status was assessed by means of odds ratio (OR) and was considered significant if the entire 95% CI was above 1.
Results
Prevalence of ESBLPE, bacterial species, and enzymes identified
Overall prevalence of ESBLPE intestinal carriage amid PDR was 7.3% (95% CI: 5.6–9.4%) with no significant statistical differences between men (9%; 95% CI: 6.2–12.5%) and women (5.9%; 95% CI: 3.8–8.6%; p = 0.07) or within distinct age groups (Table 1) except for the 5–15 years group that exhibited a significant lower prevalence when compared with rest of the age groups. The mean age of colonized and noncolonized PDR was 30 (SD 29.1) and 32.8 (SD 29.8) years, respectively (p = 0.58), and 50.6 (SD 21) and 46 (SD 25.9) years when we considered only subjects over 5 years (p = 0.33). Enteropathogenic bacteria (Salmonella enterica, Campylobacter spp. Yersinia enterocolitica, Aeromonas spp.) were recovered from the stools of 11% of PDR (10.8% of ESBLPE intestinal carriers and 14.9% of noncarriers).
Prevalence of Extended-Spectrum β-Lactamase-Producing Enterobacterales Intestinal Carriage Among Individuals Living in Private Dwellings (Overall Data and Data Stratified by Age Group)
CI, confidence interval.
Intestinal colonization by ESBLPE among NHR (31%; 95% CI: 20.5–43.1%) was significantly higher than among PDR over 67 years of age (5.5%; 95% CI: 2.2–10.9%; p < 0.0001). In fact, in individuals 68 years of age or over, institutionalization in a nursing home was significantly associated with ESBLPE carriage (OR 7.7; 95% CI: 3.1–19.3%). The mean age of colonized and noncolonized NHR was 85 (SD 6.2) and 87 years (SD 5.9), respectively (p = 0.32).
A total of 78 ESBLPE were recovered from the same number of patients (56 PDR and 22 NHR). No patient was colonized by more than one ESBLPE or by an ESBLPE and a PCPE simultaneously. E. coli accounted for the 91% (n = 71) of ESBL-producing isolates and K. pneumoniae for the remaining 9% (n = 7).
The distribution of the different enzymes identified in ESBLPE isolates recovered from PDR and NHR are shown in Tables 2 and 3, respectively. CTX-M-15 was the only ESBL identified in K. pneumoniae isolates, whereas E. coli isolates carried CTX-M-15, CTX-M-9 group, SHV, and TEM group enzymes. A single E. coli isolate displayed a resistant phenotype consistent with ESBL production but the enzyme could not be characterized, since PCR for CTX-M, SHV, GES, VEB, BEL, PER, and SFO groups were negative and sequencing of the product obtained from blaTEM PCR amplification revealed that it only produced TEM-1. CTX-M enzymes were predominant both in PDR (82.1%) and in NHR (81.8%).
Distribution of Bacterial Species and Extended-Spectrum β-Lactamase Type Among Colonized Patients Living in Private Dwellings
PCR for CTX-M, SHV, GES, VEB, BEL, PER, and SFO groups negative. PCR and sequencing of TEM-group revealed only production of TEM-1.
PCR, polymerase chain reaction.
Distribution of Bacterial Species and Extended-Spectrum β-Lactamase Type Among Colonized Patients Institutionalized in Nursing Homes
CTX-M-15 was the most common ESBL identified in isolates from PDR (53.6%), followed by CTX-M-14 (19.6%) and SHV-7 (7.1%). We could not find significant differences when comparing the distribution of the different types of ESBLs between the distinct age groups within the PDR cohort. CTX-M-15 was also the most frequent enzyme among ESBLPE from NHR (72.7%) followed by SHV-5 (13.6%). The frequency of production of CTX-M-15 and SHV group ESBLs was higher in isolates from NHR than from PDR and the opposite happened with CTX-M-9 group and TEM group enzymes, although differences did not reach statistical significance. CTX-M-15-producing E. coli was the preponderant ESBLPE among PDR (42.8%) and NHR (68.2%) with an overall prevalence of 3.5% and 21.1%, respectively.
Prevalence of ESBL-producing E. coli isolates belonging to the O25b-ST131 clonal group
Prevalence of ESBL-producing E. coli ascribed to O25b-ST131 clonal group among the PDR cohort is shown in Table 1; the overall prevalence was 0.92% (7/762; 95% CI: 0.37–1.88%). Prevalence among NHR was 19.7% (14/71; 95% CI: 11.2–30.8%) and only 1.56% (2/18; 95% CI: 0.19–5.53%) amid PDR over 67 years of age (OR 14.08; 95% CI: 3.09–66.7; p < 0.0001). 90.5% (19/21) of O25b-ST131 E. coli isolates produced CTX-M-15 and the remaining two produced CTX-M-14. The O25b-ST131 isolates accounted for 14% (7/50) of all ESBL-producing E. coli in the PDR cohort and for 66.7% (14/21) in the NHR cohort (p < 0.001), whereas the figures amid CTX-M-15-producing E. coli isolates were 25% (6/24) and 86.7% (13/15; p < 0.001), respectively.
Resistance phenotypes and presence of transferable quinolone-resistant determinants among ESBLPE
Distribution of resistance to amoxicillin/clavulanate and to different non β-lactam antimicrobials, of resistance patterns and occurrence of non-ESBL and transferable quinolone-resistant determinants among our ESBLPE isolates are shown in Table 4.
Occurrence of Plasmid-Encoded Nonextended-Spectrum β-Lactamases, Antimicrobial Drug Resistance, Non-β-Lactam Resistance Phenotypes and Transferable Quinolone Resistance Determinants in Extended-Spectrum β-Lactamase-Producing Enterobacterales Isolates
PCR for CTX-M, SHV, GES, VEB, BEL, PER, and SFO groups negative. PCR and sequencing of TEM-group revealed only production of TEM-1.
Ag: aminoglycosides; Cip, ciprofloxacin; Cot, cotrimoxazole.
Up to 89.6% of ESBLPE isolates were resistant to ciprofloxacin, 72.7% were multidrug resistant (additional resistance to two or more non-β-lactam antimicrobials), and 46.2% carried transferable quinolone-resistant determinants, being aac(6′)Ib-cr the most prevalent. All isolates were susceptible to imipenem, ertapenem, ceftolozane/tazobactam (MIC50 0.4 mg/L; MIC90 0.7 mg/L) and ceftazidime/avibactam (MIC50 0.125 mg/L; MIC90 0.4 mg/L). Regarding CTX-M-15-producing E. coli isolates, the presence of aac(6′)Ib-cr and resistance to almost all antimicrobials were more frequent among those belonging to O25b-ST131 clonal group (Fig. 1).
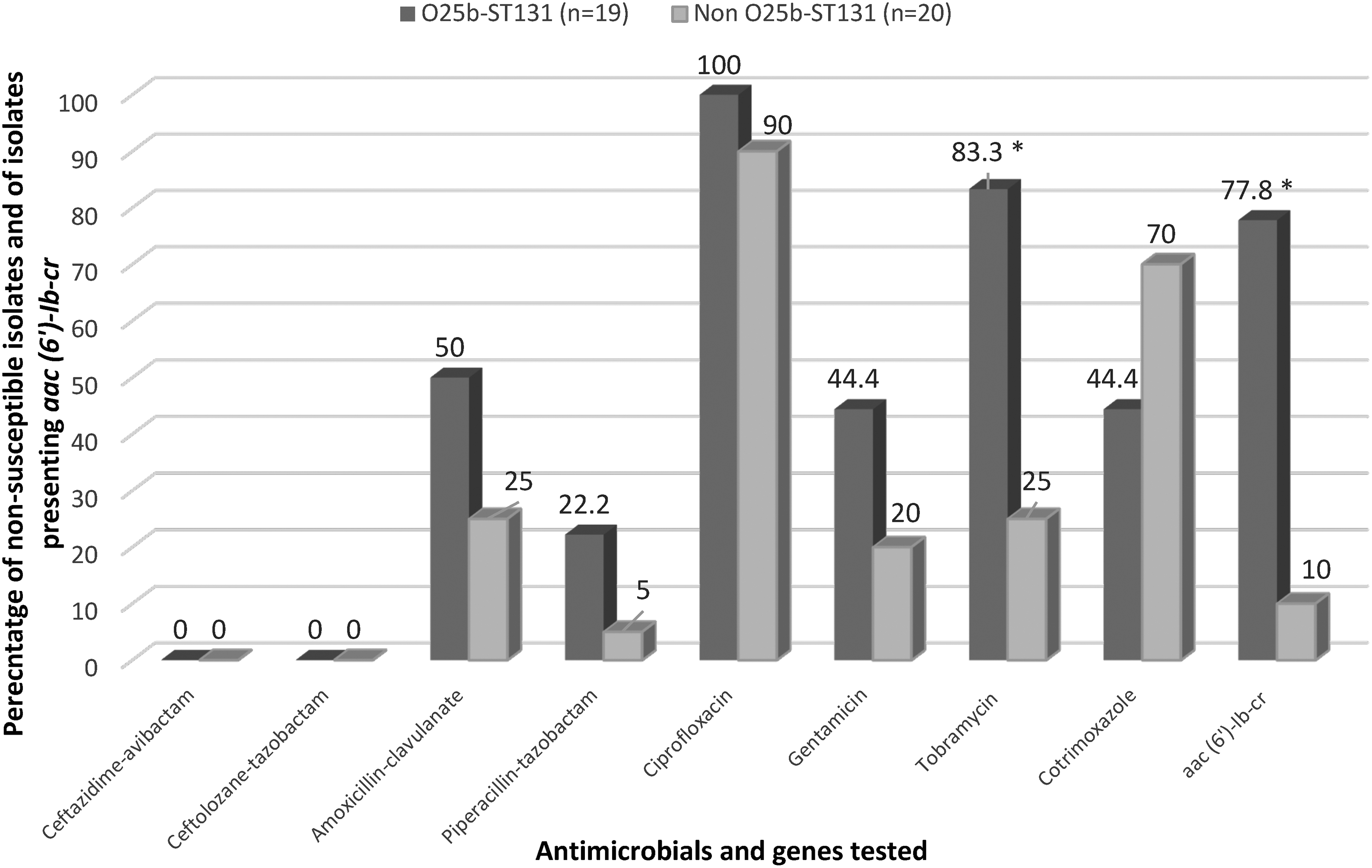
Percentage of resistance to different antimicrobials and of the presence of aac (6′)-Ib-cr gene among CTX-M-15-producing Escherichia coli isolates according to their adscription to O25b-ST131 clonal group. *Statistically significant differences when comparing O25b-ST131 and non-O25b-ST131 isolates (p < 0.001).
Epidemiological features of ESBLPE intestinal carriers
Antimicrobial exposure to antibiotics in the previous year (63.3%), contact with farm animals or pets (50%), and travel or relationship with subjects having traveled to countries with high ESBLPE prevalence (44.9%) were the most common features among colonized PDR. Up to 33.3% of PDR intestinal carriers presented none of the classic known risk factors for multidrug-resistant microorganisms' colonization, of which 87% referred usual contact with animals or some relationship with countries with high ESBLPE prevalence. Unfortunately, clinical and epidemiological information from noncolonized PDR was not available, since due to logistical constraints we decided to interview or to seek informed consent to consult clinical records only from colonized patients.
The distribution of clinical and epidemiological variables potentially associated with ESBLPE colonization among the NHR cohort are depicted in Table 5. Among the studied variables, only prior antibiotic therapy and presence of skin ulcers were significantly associated with ESBLPE carriage, although history of contact with animals showed a trend toward significance (p = 0.09).
Distribution of Clinical and Epidemiological Features Among Nursing Home Residents
ESBLPE, extended-spectrum β-lactamase-producing Enterobacterales; OR, odds ratio.
With regard to ESBL-producing E. coli intestinal carriers, after stratification on the basis of the type of residence, the variables that were significantly associated with colonization by O25b-ST131 clonal group were age over 25 years in PDR (p = 0.05) and amoxicillin/clavulanate exposure, which was a protective factor, in NHR (p = 0.02). Nevertheless, masculine gender appeared to behave as a risk factor for O25b-ST131 carriage in PDR (p = 0.097) (Table 6).
Distribution of Clinical and Epidemiological Features Among Patients Colonized by O25b-ST131 and Non-O25b-ST131 Extended-Spectrum β-Lactamase-Producing Escherichia coli Isolates After Stratifying by Type of Residence
PCPE intestinal carriers
Two PCPE (E. coli and Klebsiella oxytoca producing OXA-48) were isolated from the feces of two PDR (prevalence 0.26%; 95% CI: 0.03–0.94%) and none from rectal swabs of NHR.
E. coli producing OXA-48 was recovered from a 3-year-old boy, whose mother was colonized by the same strain, having traveled to Morocco. The isolate was resistant to amoxicillin, amoxicillin/clavulanate, and piperacillin/tazobactam, and susceptible to broad-spectrum cephalosporins, ertapenem (MIC ≤0.5 mg/L), and imipenem (MIC 2 mg/L). K. oxytoca producing OXA-48 was recovered from a 58-year-old male who had been discharged from a tertiary hospital 3 months earlier and who was being treated with immunosuppressants. The isolate was resistant to amoxicillin, amoxicillin/clavulanate, and piperacillin/tazobactam, intermediate to ertapenem (MIC 1 mg/L) and ciprofloxacin (MIC 1 mg/L) and susceptible to broad-spectrum cephalosporins and imipenem (MIC ≤1 mg/L).
Discussion
A considerable number of infections due to ESBLPE and PCPE are preceded by intestinal colonization. Nevertheless, the prevalence of ESBLPE and PCPE intestinal carriers and the distribution of involved enzymes differ greatly between different countries and even regions and also between different settings. 15 Thus, availability of local information on this issue may be of capital importance for selecting appropriate empirical antimicrobial therapy and for applying infection control measures when indicated.
The present study, aimed at assessing the current situation in nonhospitalized individuals of our Health Region, yielded a prevalence of ESBLPE intestinal carriers of 7.3% among PDR and of 31% among NHR. The prevalence among PDR is similar to that reported in other surveys conducted in outpatients in Spain in the last decade,16,18,19 although, as those studies did not differentiate between patients coming from nursing homes and those coming from their own homes, we presume that the prevalence in the latter group should actually be lower than in our series.
In spite of having not found significant differences between prevalence among PDR of distinct age groups (except for the 5–15 years group in which prevalence was of only 1%), the higher rates of carriage occurred in children under 5 years (9.7%) and adults between 16 and 50 years (9.8%), whereas the rate in patients older than 65 years was 6.7%. Indeed, the mean age of colonized PDR was 30 years, very similar to that of noncolonized and much lower than the mean age of ESBLPE carriers reported in other studies, which was around 65 years.18–20
Two recent works have alerted about the rapid increase in ESBLPE carriage among children in France (4.8% in 2010 vs. 10.2% in 2015) 26 and Sweden (2.6% in 2010 vs. 16.8 in 2016), 27 and a prospective follow-up study conducted in a cohort of 125 healthy neonates in Northern Spain found a prevalence of 24%. 17 The aforementioned results highlight the role of infants as reservoirs of ESBLPE in the community and the major challenge that treatment of infections in this population may represent.
Frequency of ESBLPE fecal carriers among NHR (31%) was almost six times higher than among PDR of the same age, indicating that NHR (more prone to suffer from comorbidities, mobility problems, functional and cognitive disorders, and to be exposed to antimicrobials) constitute important reservoirs of ESBLPE in our setting. These results contrast with those published in Sweden 28 and in the Netherlands, 29 which showed a very similar frequency of intestinal colonization among elderly living in their own homes and those institutionalized in nursing homes/long-term care facilities.
We have not been able to find data on the current situation in Spanish facilities, although colonization rates among NHR vary substantially between different countries and institutions, ranging from 1.9% in a multicenter study carried out in France to 40% in North Ireland.30–33 This variability may reflect differences in the colonization pressure, in the ratio of nurses to residents, in the compliance of basic hygienic measures or in antibiotic use.
In accordance with other studies carried out in Spain and other European countries,16–19,28,33 most ESBLPE in our series, both in the PDR and in the NHR cohorts, were E. coli, whereas CTX-M that accounted for 82% of ESBLs identified in the two cohorts, were the most common enzymes.
CTX-M-15 was the predominant ESBL, not only among isolates from NHR (72.7%) as it had been previously described,28–33 but also among isolates from PDR (53.6%), followed by CTX-M-14 and SHV enzymes. Diaz-Agero Perez et al. found that 52.9% of ESBLs detected in carriers identified at admission in a university hospital in Madrid from 2014 to 2016 were CTX-M-15, 19 whereas the frequency was only 5.9% in a previous study conducted in 2007 in the same hospital among outpatients. 16 Likewise, CTX-M-15 was not found in a prevalence survey conducted in 2007 in healthy adults from two Spanish regions 34 and accounted for just a 6% among healthy children from Gipuzkoa (Spain) in 2012. 17
Interestingly, up to 86.7% of CTX-M-15-producing E. coli isolates from NHR and 25% from PDR belonged to O25b-ST131 clonal group, which was also represented in 16.7% of CTX-M-14-producing isolates. A frequency of 24.1% was reported among CTX-M-15-producing isolates from intestinal carriers in Birmingham 35 and of 51% among French children in the community, 26 whereas the percentage among isolates from NHR in a federal state of Germany was 60%. 36
These findings point out that CTX-M-15 is displacing other ESBLs that were formerly preponderant in community gut carriers, as was the case of CTX-M-14 and SHV-12 in Spain, which is to a large extent due to the successful transmission of the O25b-ST131 lineage. This is particularly true for NHR, which have become significant reservoirs of this high-risk clone, whereas horizontal transference of mobile genetic elements may be more relevant in PDR, as was noticed elsewhere. 37
The rates of antimicrobial resistance in the ESBLPE isolates of the current study were worryingly elevated, and much higher than those reported by other European researchers,16,17,29,34,37 with 89.7% of them being resistant to ciprofloxacin, 56.8% to cotrimoxazole, 48.7% to tobramycin, 31.2% to amoxicillin/clavulanate, and as much as 72.7% being resistant to at least two groups of non-β-lactam antibiotics. On the other hand, it is noteworthy mentioning the high percentage of isolates carrying transferable quinolone resistance determinants (46%), mainly aac-(6′)-Ib-cr, in our cohort compared with the 14% identified by Paniagua et al. in isolates from 2007. 16 The association of ESBL production with multidrug resistance and with transferable quinolone resistance determinants, related outstandingly to the spread of ST131 isolates producing CTX-15, amplifies the magnitude of the problem.
Concerning the risk factors for intestinal ESBLPE carriage, overall data analysis demonstrated that residence in a nursing home, but not age, was significantly associated with colonization. Hence, this circumstance should be taken into account when selecting empirical antimicrobial therapy.
As we have stated before, due to the lack of information on noncolonized PDR, we could not assess which features act as risk factors in this cohort. Notwithstanding, data obtained from 200 healthy subjects who have already been recruited for another epidemiological survey, which is underway in our Health Region, indicate that in the general population the frequency of exposure to antibiotics in the prior 12 months (29%) and of travels to countries with high prevalence of ESBLPE or close relationship with subjects having traveled there (30%) is rather lower than in colonized patients of the PDR cohort under study (63% and 45%, respectively), whereas history of usual contact with animals was similar in both groups (56% and 50%). Moreover, a recent meta-analysis on this issue found that international travel and antibiotic consumption, but not contact with animals, were associated with a higher colonization rate. 15
As regards to the NHR cohort, antimicrobial exposure and skin ulcers (which could be a surrogate of impaired mobility), but not classical risk factors, such as urinary catheters, diabetes mellitus, recurrent urinary tract infections, or prior hospitalization,31,32 showed a significant relationship with ESBLPE colonization. On the other hand, there is some controversy about risk factors for O25b-ST131 ESBL-producing E. coli carriage.6,26,38 In our series, institutionalization in a nursing home increased the risk of colonization by 14-fold, whereas amoxicillin/clavulanate use showed a protective effect in NHR and age over 25 years and masculine gender enhanced the likelihood of intestinal carriage in PDR. The latter could be due to a higher exposure in these subsets of individuals to other potential risk factors, such as proton pump inhibitors' consumption that were not contemplated in the present survey.
Finally, in concordance with other surveys conducted in Spain,18–20 community fecal carriers of PCPE were anecdotal. We could only detect two OXA-48-producing isolates (E. coli and K. oxytoca), which did not produce ESBL and with low MICs for carbapenems. Both were recovered from PDR with recognized risk factors (a child having traveled to Morocco, whose mother was also colonized and a patient, recently discharged from a tertiary hospital after undergoing a kidney transplant, who was in treatment with immunosuppressants).
Nonetheless, since this work was finished, we have recovered several OXA-48-producing Enterobacterales from urine specimens obtained from patients with no history of foreign travels nor hospital admission or underlying diseases, but in whom and in some of their household contacts we could document intestinal colonization (data not published). These findings suggest that migratory movements and household transmission, among others, contribute to the introduction of OXA-48-producing Enterobacterales in our setting.
Surprisingly, and similarly to the situation described in Belgian nursing homes, 33 no PCPE were identified among NHR, what contrasts with a relative high prevalence of PCPE (4.1%) recorded in long-term hospitals in Madrid. 39
In summary, in spite of the limitations of the current work (the PDR study sample did not comprise healthy asymptomatic individuals but patients suffering from gastrointestinal disorders; epidemiological information could have been affected by recall bias or incomplete data in medical records and it was not available in noncolonized PDR; the number of patients included in the NHR cohort was low), we can conclude that in our geographical area (1) community fecal carriers of virtually all age groups, and particularly NHR, are important reservoirs of multidrug-resistant ESBLPE; (2) CTX-M-15, linked to E. coli O25b-ST131 notably in NHR, has become the dominant enzyme; and (3) PCPE gut carriers are already present in the community. To cope with this challenging scenario, it is mandatory to deepen our knowledge of the risk factors and routes of transmission involved in ESBLPE and PCPE carriage.
Footnotes
Acknowledgments
The authors are grateful to María Pérez Vázquez and Belén Aracil from the Laboratorio de Referencia e Investigación en Resistencia a Antibióticos e Infecciones Relacionadas con la Asistencia Sanitaria (Centro Nacional de Microbiología, Majadahonda, Madrid, Spain) for performing GES, VEB, BEL, PER, and SFO ESBLs PCR. They thank Andrea Gras for editorial assistance.
Disclosure Statement
The authors declare that there are no conflicts of interest regarding the publication of this article.
Funding Information
This work was partially supported by Fundació Dr Ferran (2016 Ferran i Clua Research on Health Sciences Grant, FFPI16/AE01).