
Abstract
Staphylococcus epidermidis, a major skin bacterium, can cause opportunistic infections. Use of antimicrobial agents against Cutibacterium acnes for acne treatment becomes a risk factor for emergence of antimicrobial-resistant skin bacteria. In this study, the impact of antimicrobial treatment of acne vulgaris on S. epidermidis antimicrobial resistance was assessed. A total of 344 S. epidermidis strains isolated from patients with acne vulgaris who visited hospital (165 strains) and dermatological clinics (179 strains), respectively, were analyzed. Except for doxycycline, the resistance rates were higher in strains isolated from patients who had used antimicrobials for acne treatment than in those isolated from patients who had not used antimicrobials. The prevalence rates of strains with erm(C) from patients who used macrolides and clindamycin (hospital, 78.0%; clinics, 61.3%) and those of strains with tet(M) from patients who used tetracyclines (hospital, 27.5%; clinics, 42.4%) were significantly higher than those of strains from patients who did not use antimicrobials (p < 0.05). All strains with erm(A) (8/8) and 91.7% strains with erm(C) (156/170) showed high-level resistance to macrolides and clindamycin (MIC ≥256 μg/mL). Furthermore, almost all strains with tet(M) showed resistance to minocycline. Our results showed that the use of antimicrobials for acne treatment may lead to an increased prevalence of antimicrobial-resistant S. epidermidis. In particular, the emergence of minocycline-resistant strains with tet(M) owing to the use of tetracyclines (doxycycline and minocycline) is a critical issue. Appropriate antimicrobial use for acne treatment may be an important strategy to prevent the emergence of antimicrobial-resistant skin bacteria.
Introduction
Staphylococcus epidermidis and Cutibacterium acnes are common colonizers of human skin. 1 Although skin bacteria generally maintain skin humidity and defence against pathogens, they can cause opportunistic infectious diseases in immunodeficient individuals. They are exposed to antimicrobials used orally and topically for the treatment of various infectious diseases, which may result in the rapid emergence of potentially resistant strains. Moreover, C. acnes exacerbates acne vulgaris and is targeted by antimicrobial treatment.2–4 In Japanese acne treatment guidelines, clindamycin, nadifloxacin, and ozenoxacin are recommended as topical agents, and doxycycline, minocycline, and roxithromycin are recommended as oral agents. Recently, the prevalence of antimicrobial-resistant C. acnes has rapidly increased in Japan, and the reduction in the clinical efficacy of antimicrobial treatment has become a major concern.5–9
In acne patients, antimicrobial use is strongly related to the prevalence of antimicrobial-resistant C. acnes. 6 In addition, S. epidermidis was isolated from acne specimens, and a strong correlation between the antimicrobial resistance (AMR) of S. epidermidis and C. acnes was observed.10,11 S. epidermidis is frequently isolated as a pathogen causing opportunistic infectious diseases and has high clinical significance because it shows a multidrug resistance pattern similar to that in Staphylococcus aureus.12,13 Although clarithromycin and levofloxacin-resistant S. epidermidis and S. aureus strains have been frequently isolated from healthy individuals and from the patients with skin and soft tissue infections, very few isolates have been found resistant to minocycline. 14 AMR can be transferred from S. epidermidis to S. aureus, which is a highly pathogenic bacterium.15,16
Therefore, appropriate antimicrobial use for the treatment of acne vulgaris may be considered an important strategy for the prevention of the emergence of antimicrobial-resistant skin bacteria. In this study, the impact of antimicrobial use for acne treatment on AMR in S. epidermidis was assessed.
Materials and Methods
Patients and bacterial strains
The study was approved by the Research Ethics Committee of the Tokyo University of Pharmacy and Life Sciences (Approval No. 16–21). Patient information was obtained using a questionnaire-based survey, and the use of antimicrobials for acne treatment in the previous 6 months was assessed. S. epidermidis strains were isolated from acne pustule specimens as previously described. 7 S. epidermidis was identified by multiplex polymerase chain reaction (PCR) to detect the thermonuclease gene and 16S rDNA sequencing.5,17 In this study, 165 and 179 S. epidermidis strains were isolated from patients with acne who visited Toranomon Hospital between 2013 and 2018 and 13 Japanese dermatological clinics during 2016–2017, respectively.5,6,18
Antimicrobial susceptibility test and resistance gene detection
Antimicrobial susceptibility of S. epidermidis was evaluated by determining the minimum inhibitory concentration (MIC) using the agar dilution method of the Clinical and Laboratory Standards Institute (CLSI).5,19 In total, five antimicrobial agents were analyzed, including doxycycline hydrate (Sigma-Aldrich, Tokyo, Japan), levofloxacin hydrochloride, clindamycin hydrochloride, and minocycline hydrochloride (Tokyo Chemical Industries, Tokyo, Japan), and erythromycin (from Wako Pure Chemical Industries, Osaka, Japan). Breakpoints of levofloxacin, erythromycin, clindamycin, doxycycline, and minocycline were used by CLSI (MIC ≥4, ≥8, ≥ 4, ≥16, and ≥16 μg/mL, respectively) and EUCAST (MIC >1, >2, >0.25, >2, and >0.5 μg/mL, respectively).20,21 Inducible clindamycin resistance in S. epidermidis strains with erm(C) was detected by a double-disk diffusion assay (D-test) according to CLSI using erythromycin discs (15 μg), clindamycin (2 μg), and Mueller Hinton II agar (Becton, Dickinson and Co.). 20
The methicillin resistance gene mecA was detected using PCR, and strains with mecA were defined as methicillin-resistant S. epidermidis (MRSE).5,6 The macrolide resistance genes erm(A), erm(C), erm(X), mph(C), and msr(A/B) and tetracycline resistance genes tet(M) and tet(K) were also detected using PCR.6,7
Statistical analysis
Comparison between the patients with previous antimicrobial use and the patients with no previous treatment was performed using Fisher's exact test in js-STAR XR. ver. 1.0.4j.
Results
AMR in S. epidermidis
Antimicrobial susceptibility tests of S. epidermidis strains isolated from Toranomon Hospital between 2013 and 2018 and dermatological clinics from 2016 to 2017 showed that strains isolated from patients who had used antimicrobials exhibited higher resistance rates for all tested agents than those of strains isolated from patients who had not used antimicrobials (Table 1). In addition, the data of S. epidermidis strains isolated from hospital during 2009–2010 in Japan were used to compare the rates of AMR and resistance genes. 7 When the correlation between antimicrobial use and resistance to the antimicrobials was analyzed, strains isolated from patients who had used macrolides and clindamycin, in which the same mechanisms confer AMR, showed significantly higher resistance rates to erythromycin (hospital, 96.6%; clinics, 85.0%) and clindamycin (hospital, 94.9%; clinics, 76.3%), respectively, than those of strains isolated from patients who had not used antimicrobials (p < 0.05).
Profiles of Staphylococcus epidermidis Isolated from Patient With/Without Antimicrobial Agents for Acne Treatment
Bold values showed the resistance rates which increased than that in 2009–2010.
Resistant strains were selected by breakpoints of CLSI. “Used” showed the strains isolated from the patients with histories of using antimicrobial agents for acne treatment. In Macrolides/Clindamycin, it showed the strains isolated from the patients who had either used oral macrolides or topical clindamycin. Similarity, in Tetracyclines, it showed the strains isolated from the patients who had either used oral tetracyclines. In Quinolones, it showed the strains isolated from the patients who had either used oral levofloxacin or topical quinolones, such as nadifloxacin and ozenoxacin. Hospital 2009–2010 and Hospital 2013–2018 were studies performed in Tokyo Women's Hospital and Toranomon Hospital in Japan, respectively.
The assessments were performed using Fisher's exact test versus Not used (p < 0.05).
Similarly, strains isolated from patients who had used tetracyclines and quinolones showed significantly higher resistance rates to minocycline (hospital, 23.5%; clinics, 39.4%) and levofloxacin (hospital, 81.3%; clinics, 51.4%), respectively, than those of strains isolated from patients who had not used antimicrobials (p < 0.05). In contrast, no difference in doxycycline resistance rate was observed between strains isolated from patients who had and had not used tetracyclines. Compared to hospital in 2009–2010, the resistance rates of erythromycin and clindamycin in hospital 2013–2018 and clinics 2016–2017 were higher; nevertheless, the rates of strains having erm(C) only showed a slight increase or decrease, respectively.
By contrast, an increase in the proportions of minocycline-resistant strains and strains acquiring tet(M) were observed. Comparing between MRSE and methicillin-susceptible S. epidermidis (MSSE), MRSE showed higher resistance rates in all tested antimicrobials (Supplementary Table S1). Therefore, our data showed that the use of antimicrobials for acne treatment is associated with an increase in the prevalence of antimicrobial-resistant S. epidermidis and changes in their resistance genes.
AMR genes
AMR genes were analyzed based on the history of antimicrobial use (Table 1). Strains isolated from patients who had used macrolides and clindamycin acquired erm(C) (hospital, 78.0%; clinics, 61.3%) more frequently than those isolated from patients who did not use any antimicrobials (p < 0.05). All strains with erm(A) and 91.7% strains with erm(C) (156/170) showed high-level resistance to macrolides and clindamycin (MIC ≥256 μg/mL). In contrast, the other 14 strains with erm(C) showed high-level resistance to macrolides and were susceptible to clindamycin. The erm(X), which confers high-level resistance to macrolides and clindamycin in C. acnes, was not detected. 8 The erm gene expresses two phenotypes, constitutive resistance showing resistance to macrolides and clindamycin, and inducible resistance showing resistance to macrolides and susceptibility to clindamycin.
To elucidate the phenotype of strains with erm(C), the D-test, which detects inducible clindamycin resistance, was conducted. Strains with erm(A) or erm(C), which possessed high-level resistance to macrolides and clindamycin, showed constitutive clindamycin resistance phenotype. In contrast, 14 strains with erm(C), which showed high-level resistance to macrolides and susceptibility to clindamycin, showed inducible clindamycin resistance phenotype.
The prevalence rate of strains with tet(M) detected in patients who had used tetracyclines was significantly higher (hospital, 27.5%; clinics, 42.4%) than in patients who did not use antimicrobials (p < 0.05). In contrast, no difference in the prevalence rate of strains with tet(K) was observed. Although MIC comparisons among very few S. aureus strains having tet(M) and tet(K) have been reported, 22 that of S. epidermidis was not well understood. Thus, the MIC distributions of doxycycline and minocycline in strains with tet(M) and tet(K) were compared (Fig. 1). According to CLSI breakpoints, almost all strains with tet(M) (95.7%, 44/46) showed resistance to minocycline but were susceptible to doxycycline.
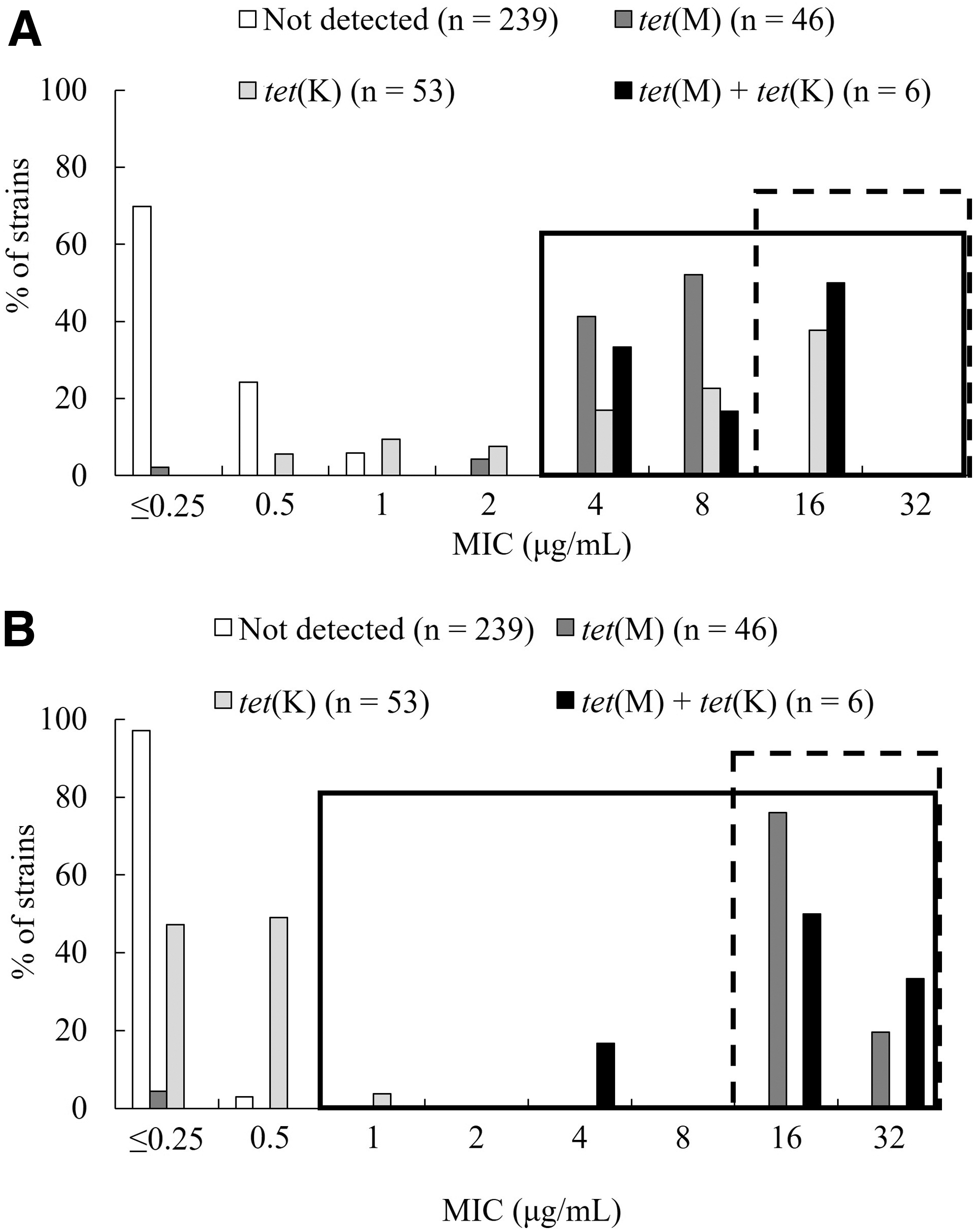
The MIC distributions of tetracyclines in Staphylococcus epidermidis strains with tet(M) and tet(K).
In contrast, several strains with tet(K) showed resistance to doxycycline (37.7%, 20/53), and all strains were susceptible to minocycline. According to EUCAST breakpoints, most of the strains with tet(M) (93.5%, 43/46) showed resistance to doxycycline and minocycline. Although strains with tet(K) showed doxycycline resistance in 77.4% (41/53), they showed few resistances to minocycline (3.8%, 2/53). Notably, no strain without tet(M) or tet(K) showed resistance to doxycycline or minocycline. MRSE acquired erm(C), tet(M), and tet(K) at higher rates than MSSE (Supplementary Table S2). Therefore, our data showed that the prevalence of minocycline-resistant S. epidermidis with tet(M) increased remarkably owing to the use of tetracyclines for acne treatment, and first described that the resistance levels to tetracyclines in S. epidermidis differed for acquisition of tet(M) and tet(K).
Discussion
S. epidermidis strains isolated from patients with acne vulgaris were analyzed to evaluate the impact of antimicrobial treatment for acne vulgaris on AMR in skin bacteria. Strains isolated from patients who had used antimicrobials showed higher resistance rates for all tested agents than those of strains isolated from patients who had not used antimicrobials. In patients with acne vulgaris, C. acnes strains isolated from the patients who had used antimicrobials showed higher resistance rates than those isolated from the patients who had not used antimicrobials.5,6 The resistance rates of erythromycin and clindamycin in C. acnes isolated from the patients who had used antimicrobials was significantly higher. An increased prevalence of quinolone-resistant S. epidermidis isolated from the patients with acne vulgaris has been reported. 11 We revealed that S. epidermidis strains as well as skin microbiota exhibit AMR due to antimicrobial use for acne treatment.
The presence of erm(C) was significantly higher in the strains isolated from patients who had used macrolides and clindamycin. Most of the S. epidermidis strains with erm(C) (91.7%) showed resistance to macrolides and clindamycin; thus, these strains expressed constitutive resistance. In contrast, the other 14 strains showed high-level resistance to macrolides and were susceptible to clindamycin. In S. aureus, more than half of the strains with erm(C) express inducible resistance and are susceptible to clindamycin in many articles.23,24 In contrast, many coagulase-negative staphylococci (CoNS), such as S. epidermidis, express constitutive resistance to macrolides and clindamycin. 25 It is reported that the strains expressing inducible resistance show constitutive clindamycin resistance by acquiring gene mutation. 26
Although clindamycin is frequently used for acne treatment, it is rarely used for the treatment of infectious diseases caused by S. aureus. Clindamycin is not a mutation inducer; however, it may select resistant mutants. Therefore, S. epidermidis strains with erm(A) and erm(C) isolated from the patients with acne vulgaris tended to show constitutive resistance that presume to develop due to exposure to antimicrobials for acne treatment.
The minocycline resistance rate in strains isolated from patients who used tetracyclines was significantly higher than that in strains isolated from patients who did not use tetracyclines. In contrast, no difference in doxycycline resistance rate was observed. The prevalence rate of tet(M) in strains isolated from patients who used tetracyclines was significantly higher than that in strains isolated from patients who did not use tetracyclines. Moreover, all strains with tet(M), except one strain that was susceptible, showed minocycline resistance. In this susceptible strain, tet(M) may act as a pseudogene because the MICs of tetracyclines were the same as those observed in susceptible strains.
The current susceptibility of S. epidermidis strains to tetracyclines with tet(M) and tet(K) is unknown. For S. aureus, strains with tet(M) are usually susceptible to minocycline (MIC = 4 μg/mL) and resistant to doxycycline (MIC = 16 μg/mL), whereas strains with tet(K) are susceptible to both these agents. 22 Therefore, the resistance levels of tetracyclines in strains with tet(M) and tet(K) were suggested to be different between S. epidermidis and S. aureus.
There is limited information available of S. epidermidis with tet(M) and tet(K) compared with S. aureus. The prevalence rates of tet(M) and tet(K) in S. epidermidis vary according to regions and isolation sites. In the study carried out in Iran, tet(M) (∼40%) and tet(K) (50%) were obtained from the strains isolated from infectious regions of patients. 27 In contrast, in China, tet(M) and tet(K) were found from the strains isolated from dental plaque with 0% and ∼20%, respectively. 28 However, no detailed susceptibility of tetracyclines was described in previous studies. Our results showed that the use of tetracyclines for acne treatment confers minocycline resistance in S. epidermidis, which is associated with an increased prevalence of strains with tet(M).
Although there were fewer patients who had used tetracyclines in clinics than in hospitals, the prevalence of strains with tet(M) isolated from patients who had used tetracyclines in clinics was higher than that in hospitals. In acne treatment, doxycycline and minocycline are highly recommended. 4 Furthermore, the number of acne patients who have been prescribed tetracyclines may be increased by the dissemination of acne treatment guidelines. Therefore, strains with tet(M) have the potential to spread further. Almost all methicillin-resistant S. aureus (MRSA) reportedly shows susceptibility to minocycline. 29 However, tet(M) located on a plasmid may transfer from S. epidermidis to S. aureus, 30 leading to multidrug resistance in MRSA by the acquisition of tet(M), which should be further investigated. Minocycline topical agents have been approved by the United States Food and Drug Administration (FDA) for acne treatment. 31
During in vitro study, no resistant- and low-susceptible mutants of C. acnes (minocycline MIC ≥0.5 μg/mL) were detected.32 However, the resistance frequency of staphylococci was not evaluated. Minocycline-resistant staphylococci acquiring tet(M) may increase in patients with acne vulgaris who use minocycline as a topical agent. To control and prevent AMR, antimicrobial use related to the development of AMR in skin inhabitants needs to be continuously surveyed.
In conclusion, our study demonstrated that the use of antimicrobials for acne treatment may lead to an increased prevalence of antimicrobial-resistant S. epidermidis. The emergence of minocycline-resistant strains with tet(M) owing to the use of tetracyclines is a critical issue. Appropriate antimicrobial use for acne treatment may become an important strategy for the prevention of the emergence of antimicrobial-resistant skin bacteria.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.