
Abstract
The prevalence of methicillin-resistant Staphylococcus aureus (MRSA) in hospitals in Portugal is worrisome and among the highest in Europe. Surprisingly, MRSA prevalence in the community was described as very low (<2%) based on studies that used classical culture-based methods (CCBM). We investigated whether the apparent limited spread of MRSA in the community in Portugal might result from low sensitivity of CCBM. Nasopharyngeal- and oropharyngeal-paired samples obtained from senior adults living in nursing (n = 299) or family homes (n = 300) previously characterized by CCBM were reanalyzed. Samples were inoculated in a semi-selective enrichment medium, and those showing visible growth were evaluated by qPCR targeting nuc, mecA, and mecC genes (SSE+qPCR). By SSE+qPCR, 34 of the 1,198 (2.8%) samples were MRSA positive compared with 21 (1.8%) by CCBM. SSE+qPCR improved non-significantly detection of MRSA carriers from 5.4% to 8.0% (p = 0.12) in the nursing home collection, and from 0.3% to 1.7% (p = 0.13) in the family home collection. MRSA isolates belonged to three HA-MRSA clones widely disseminated in Portuguese hospitals. In conclusion, use of semi-selective medium combined with qPCR did not change the overall scenario previously described. In Portugal, MRSA circulation in the community among senior adults is low.
Introduction
Staphylococcus aureus is an opportunistic Gram-positive bacterium that colonizes asymptomatically the human anterior nares. It has been estimated that 20–40% of the adult population is colonized with S. aureus. 1 It is also a main cause of a wide range of infections, including skin and soft tissue infections, pneumonia, endocarditis, and bacteremia affecting primarily debilitated individuals such as those with diabetes, undergoing hemodialysis or with HIV. 2
Methicillin-resistant S. aureus (MRSA), in particular, is a leading cause of morbidity and mortality worldwide, and has been associated for >40 years with nosocomial settings only (hospital-associated MRSA [HA-MRSA]). In the late 1990s, however, MRSA emerged from the community affecting healthy individuals without typical risk factors for MRSA carriage (community-associated MRSA [CA-MRSA]).3–6 During the past decade, the prevalence of CA-MRSA increased very rapidly worldwide, varying from country to country.6,7
In parallel, an increasing blur between CA-MRSA and HA-MRSA clones has been described in several countries. For example, the EMRSA-15 clone traditionally associated with hospital infections has been found circulating in the community in England, Italy, and Portugal.8–10 Furthermore, some CA-MRSA clones such as USA300 and USA400 have been associated with nosocomial infections.11,12 In Greece, a country with high rates of both HA-MRSA and CA-MRSA, the presence of the CA-MRSA European clone ST80-IV was identified not only in the community (c.a. 90%) but also in hospitals (c.a. 11%). 13
In Portugal, the burden of MRSA infections is among the highest in Europe. Still, in recent years the rates of HA-MRSA (isolated from blood or cerebrospinal fluid) have been declining: from c.a. 50% in 2015 to c.a. 35% in 2019. 6 This declining trend parallels what has been observed in most European countries although the reasons underlying it are poorly understood, as these declines have not always been directly correlated with improved infection control practices and/or antibiotic stewardship.
The molecular epidemiology of nosocomial MRSA has been extensively studied in Portugal since the early 1990s. At that time the Iberian clone (ST247-IA) was dominant in several Portuguese hospitals, having been replaced by the Brazilian clone (ST239-IIIA) in the mid 1990s.14,15 In 2001, the EMRSA-15 (ST22-IVh) clone emerged in Portugal and soon became the dominant clone in nearly all hospitals, a situation that has persisted for several years. Since 2010, in parallel with EMRSA-15, the New York/Japan related clone (ST105-II) and the Pediatric and its related clones (ST5-IVc and ST125-IVc, respectively) were also found to be frequent in Portuguese hospitals, representing together c.a. 20% of the MRSA isolates.14–17
In Portugal, the available studies suggest that the prevalence of CA-MRSA is low,18–20 a somewhat surprising observation given its high prevalence in hospitals. 6 Previous studies conducted in the community among children attending day-care centers, young healthy adults (draftees and university students), and adults aged >60 years reported a prevalence of MRSA asymptomatic colonization <2%.18–20
Two other studies showed MRSA rates >20% in the community.10,16 However, differently from the studies mentioned above, where only colonization samples were obtained, the latter studies included not only colonization samples but also infection samples. One study included individuals attending health care centers due to skin and soft tissue infections.10,16 The other included individuals attending health care centers and hospital inpatients from which MRSA was isolated within the first 48 hr upon admission.10,16
The gold standard for routine detection of MRSA from clinical specimens are culture-based approaches. These methodologies are laborious and time-consuming as they are often preceded by a selective enrichment step, require isolation of a pure culture and its characterization. 21 In recent years, in-house and commercial PCR-based methods have been developed.22,23 These strategies enable the reliable identification of MRSA within hours and have a high sensitivity, which is important in low-density samples. 24
In carriage studies, culture-based approaches are also the most frequent ones for the identification of MRSA. 24 The few studies available that have used quantitative real-time PCR (qPCR)-based methods to investigate MRSA carriage, in patients admitted to an intensive care unit and individuals attending health care organizations, have shown that these methods yield comparable results with those obtained by using culture-based approaches.23,25
We hypothesized that the low prevalence of MRSA observed among individuals in the community in Portugal might be due to an underestimation of carriage with low-sensitivity classical culture-based approaches.
The aim of this study was to investigate the prevalence of MRSA carriage in the community, among healthy adults >60 years of age, using a highly sensitive approach, which involved a semi-selective enrichment step followed by qPCR.
We revisited two collections of carriage samples previously characterized by classical culture-based approaches obtained from adults >60 years of age living in either nursing homes or family homes in Portugal. We combined the use of a semi-selective enrichment step followed by qPCR to re-evaluate the prevalence of MRSA carriers in this age group.
Materials and Methods
Study population and samples
This study was nested on a larger one conducted previously. 18 In brief, the prevalence of S. aureus and MRSA carriage, associated risk factors, and the properties of circulating MRSA lineages were studied in a Portuguese population of 3,361 adults of >60 years of age, between April 2010 and December 2012. Nasopharyngeal and oropharyngeal samples (3,361 samples each) were obtained for each participant, as previously described. 26
S. aureus and MRSA isolates were identified by classical culture-based methods (CCBM): nasopharyngeal and oropharyngeal swabs were plated onto mannitol salt agar (Difco, Detroit, MI, USA) and incubated in aerobic conditions, overnight at 37°C; the yellow colonies were streaked on tryptic soy agar (TSA) (Difco) and, on the following day, presumptive S. aureus colonies were tested for the production of coagulase using Staphaurex test (Remel, Lenexa, KS, USA). Oxacillin and cefoxitin susceptibility was tested for all S. aureus isolates, by agar disk diffusion, according to the Clinical and Laboratory Standards Institute (CLSI) guidelines. 27
Screening for the mecA gene was performed by PCR to identify MRSA. 28 Genotyping of MRSA was carried out by SCCmec typing, spa typing, and multilocus sequence typing (MLST) following previously described protocols.19,28 Nasopharyngeal and oropharyngeal swabs were frozen in skim milk, tryptone, glucose, and glycerin (STGG) and stored at −80°C.
In this study, two collections of samples from the earlier initial study were re-examined. One collection corresponded to 600 paired samples (300 nasopharyngeal and 300 oropharyngeal) obtained from 300 individuals randomly selected from a pool of 3,062 individuals living in their own family home. The second collection corresponded to 598 paired samples (299 nasopharyngeal and 299 oropharyngeal) obtained from all individuals (n = 299) living in nursing homes at the time of the initial study. 18
Identification of MRSA by molecular methods
To screen for MRSA, an enrichment step was used: 200 μL of the frozen stock of each (nasopharyngeal and oropharyngeal) sample were inoculated into 2 mL of a semi-selective enrichment broth—tryptic soy broth (Difco), containing 2.5% of NaCl (Merck), 3.5 mg/L cefoxitin, and 20 mg/L aztreonam (Sigma-Aldrich) 29 —and were incubated overnight at 37°C in ambient air with agitation. Total DNA was extracted from turbid cultures (indicative of bacterial growth) using the MagNA Pure Compact system (Roche Diagnostics GmbH) according to a modified protocol: 200 μL of the enriched culture were centrifuged for 1 min at 13,000 rpm.
The supernatant was discarded, the pellet was resuspended in 250 μL of phosphate-buffered saline (PBS) 1 × (PBS: NaCl 137 mM, KCl 2.7 mM, Na2HPO4 10 mM, and KH2PO4 1.8 mM, pH 7.4), and 200 μL were transferred into a tube containing 200 μL of a lysis buffer (Roche) and 10 μL of lysostaphin 10 mg/mL (AMBI products LLC). Tubes were incubated for 20 min at 37°C, and the subsequent isolation steps were performed in the MagNA instrument. DNA concentration and nucleic acid purity ratios, A260/A280 and A260/A230, were assessed using NanoDrop (Thermofisher).
DNA samples were tested by qPCR targeting mecA (confers resistance to methicillin), mecC (homolog of mecA, confers resistance to methicillin), and nuc (encodes for a S. aureus thermonuclease) genes. The sequences of primers and probe for mecA (Applied Biosystems, Germany) were described before 30 ; for mecC (Applied Biosystems) and nuc (TIB MOLBIOL, Germany), sequences were kindly provided by Prof. Henrik Westh from the University of Copenhagen, as part of an in-house multiplex qPCR (H. Westh, pers. comm.). 31 For all samples two qPCRs were performed. The first qPCR targeted the nuc gene and was performed in a final volume of 25 μL, containing 1 × FastStart TaqMan Probe Master (Roche), 250 nM of each primer, 125 nM of probe, and 2.5 μL of total DNA.
The second qPCR, a duplex, targeted mecA and mecC genes, and was also performed in a final volume of 25 μL, containing the same concentration of primers and probes as described for the nuc gene. DNA was amplified using the CFX96 QSystem Amplification (Bio-Rad) using the following cycling conditions: 95°C for 10 min followed by 45 cycles of 95°C for 10 sec; 55°C (for nuc) or 60°C (for mecA and mecC) for 25 sec; and a final step of 40°C for 30 sec. Samples were considered positive for the gene tested if the cycle threshold (Ct) value was <40. Samples positive for both nuc and mecA (or mecC) genes with concordant Ct values (|Ctnuc – Ctmec|≤2) were considered to contain MRSA only.
Samples positive for mecA or mecC and negative for nuc were considered to contain methicillin-resistant coagulase-negative staphylococci (MRCNS) and no MRSA. Samples positive for nuc and mecA, but with discordant Ct values, were considered to potentially contain MRSA among other staphylococci depending on the Ct values obtained. Strains COL (MRSA, with MLST-SCCmec type-spa type ST250-I-t008, positive control for mecA gene), LGA251 (MRSA, ST425-XI-t6300, positive control for mecC gene), ATCC25923 (S. aureus, ST243-t948), and ATCC14990 (Staphylococcus epidermidis, negative control for S. aureus/MRSA) were used as controls.
Characterization of MRSA isolates
Samples positive for MRSA by qPCR were re-examined to try to isolate a pure culture of MRSA. Two hundred microliters of each MRSA-positive previously enriched culture were plated on a chromogenic selective medium CHROMagar MRSA (ChromAgar, Paris, France) and incubated overnight at 37°C with ambient atmosphere. Strains COL (MRSA) and ATCC14990 (S. epidermidis) were used as positive and negative controls, respectively. For each sample, up to 50 presumptive MRSA colonies were picked and isolated in TSA plates.
The presence of mecA was confirmed by qPCR, using the same primers mentioned above. From each sample, one positive MRSA colony was further cultivated and characterized by SCCmec typing, spa typing, and MLST, as previously described.19,28 DNA sequencing reactions were performed at STAB VIDA (Caparica, Portugal).
Statistical analysis
The Ct values of nuc and mecA genes from nasopharyngeal and oropharyngeal samples were summarized by their geometric mean and corresponding standard deviation. Statistical associations between the Ct values from nursing homes versus family home and nasopharynx (NP) versus oropharynx (OP) were obtained by using a generalized linear model with a Gaussian distribution and a log link function.
Culture and qPCR approaches were compared by the McNemar's test based on paired individuals. To compare the prevalence of MRSA between nasopharyngeal and oropharyngeal samples and between nursing home and family home by qPCR or CCBM, the chi-square test was used. A p-value of <0.05 was considered statistically significant for all tests used. All analyses were performed using R version 3.2.3. 32
Ethics statement
The initial study was performed in line with the European Statements for Good Clinical Practice and the principles of the Declaration of Helsinki of the World Health Medical Association. The study was registered and approved at health care centers of Oeiras and Montemor-o-Novo that report to Administração Regional de Saúde (ARS, “Regional Health Administration”) of Lisboa e Vale do Tejo, and Alentejo, respectively, from the Ministry of Health. Informed written consent was obtained from all participants. A numeric code was attributed to all samples and questionnaires, all of which were processed anonymously. This study—a retrospective reanalysis of samples—did not require ethical approval.
Results
Detection of MRSA carriage by semi-selective enrichment followed by qPCR
We used semi-selective enrichment followed by qPCR to re-evaluate MRSA carriage in samples obtained from 599 adults aged >60 years, divided into two collections: participants living in nursing homes (n = 299) and participants living in family homes (n = 300). These samples are a subset of 6,722 samples (3,361 nasopharyngeal samples and 3,361 oropharyngeal samples) obtained in a study previously described. 18 Overall, in this study we analyzed 1,198 paired samples (599 nasopharyngeal samples and 599 oropharyngeal samples) and compared the results with those previously obtained by classical culture-based approaches for the same samples. 18 The sociodemographic characteristics of the population were described before 18 and are summarized in Supplementary Table S1.
By semi-selective enrichment, 241 of the 1,198 samples showed visible growth after overnight incubation. By qPCR, 34 of the 241 (14.1%) samples with visible bacterial growth were positive for both nuc and mecA genes, suggesting that they contained MRSA.
We next looked for concordance between the Ct values obtained for nuc (specific for S. aureus) and mecA (indicating methicillin resistance) within each individual sample to infer on the potential presence of methicillin-susceptible S. aureus (MSSA) or MRCNS. In 23 samples, both Ct values were concordant (differing in ≤2 Ct) suggesting the exclusive presence of MRSA in those samples (Fig. 1).
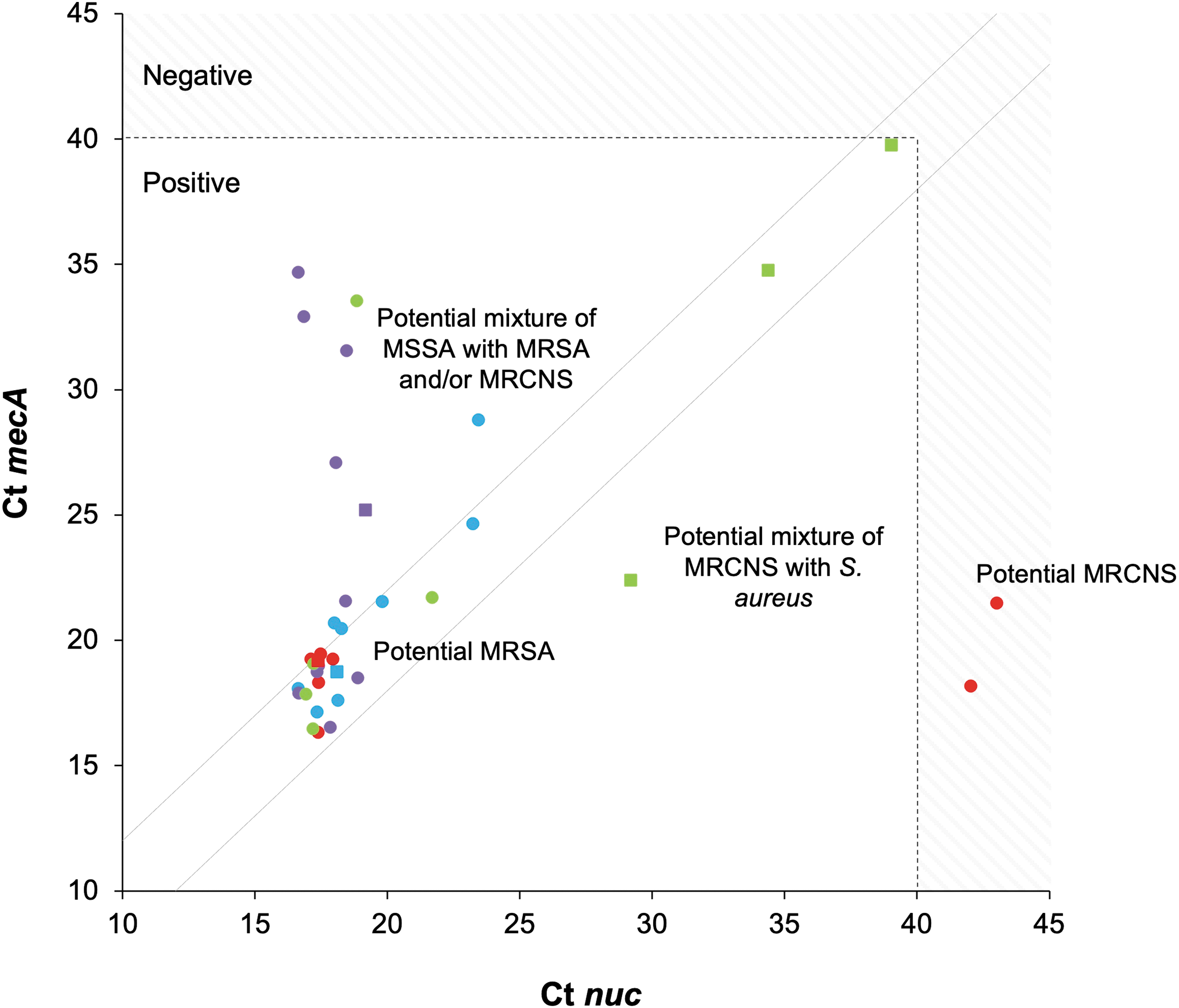
Detection of MRSA by qPCR in adults >60 years of age living in nursing homes (circles) and family homes (squares). Each dot represents a sample and its position corresponds to the Ct values for nuc and mecA genes. Blue, nasopharyngeal samples that were positive by culture; purple, nasopharyngeal samples that were negative by culture; red, oropharyngeal samples that were positive by culture; green, oropharyngeal samples that were negative by culture. Diagonal dashed lines indicate the threshold of 2 Ct values difference between nuc and mecA genes. Samples with Ct values >40 were considered to be negative. Ct values for mecC gene are not shown since all samples were negative for this gene, with Ct values ≥40. Potential presence of staphylococci—Staphylococcus aureus or CNS—and MR is indicated based on Ct values for nuc and mecA. CNS, coagulase-negative staphylococci; Ct, cycle threshold; MR, methicillin resistance; MRCNS, methicillin-resistant coagulase-negative staphylococci; MRSA, methicillin-resistant S. aureus; MSSA, methicillin-susceptible S. aureus; qPCR, quantitative real-time PCR. Color images are available online.
Of note, 10 samples had Ct values for nuc that were lower in >2 U than those obtained for mecA, suggesting that those samples contained a potential mixture of MSSA with MRSA and/or MRCNS strains (Fig. 1). Similarly, there were three samples in which the opposite occurred, suggesting that these contained a potential mixture of S. aureus and MRCNS (Fig. 1). In addition, there were two samples that were only positive for mecA suggesting the presence of MRCNS (Fig. 1). All samples were negative for mecC (Ct values ≥40).
Of note, there were six MRSA samples that were previously identified by culture-based methods that were not identified in this study using semi-selective enrichment followed by qPCR. Several unsuccessful attempts were made to recover these samples. We hypothesized that the original swab frozen stock might have lost viability. To investigate the plausibility of this hypothesis we selected randomly 40 original swab frozen stocks previously identified as containing MSSA. In 14 cases (35%), we were unable to isolate the MSSA. Importantly, this only happened in these low-density multispecies frozen stocks (containing the swabs in STGG medium), and was not observed for the pure cultures isolated and frozen at the time of the original study.
Concordance between oropharyngeal and nasopharyngeal swabs for detection of MRSA by qPCR
Among the 34 MRSA-positive samples detected by SSE+qPCR, 20 were nasopharyngeal samples and 14 were oropharyngeal samples. Of these, only 12 were concordant (paired) samples obtained from 6 individuals. Compared with sampling the OP only, the addition of nasopharyngeal sampling improved significantly the overall detection of MRSA carriage (18/599, 3.0% vs. 34/599, 5.7%; p = 0.03). In contrast, compared with sampling the NP only, the addition of oropharyngeal sampling did not significantly improve the detection of MRSA carriage (22/599, 3.7% vs. 34/599, 5.7%; p = 0.13).
Comparison of semi-selective enrichment followed by qPCR with classical culture-based approaches for detection of MRSA nasopharyngeal and oropharyngeal carriage
The use of semi-selective enrichment followed by qPCR, when compared with CCBM, improved detection of MRSA carriage in oropharyngeal and nasopharyngeal samples in both the nursing home and family home collections (Table 1 and Fig. 2). This increase was, however, only statistically significant for the nasopharyngeal samples from the nursing home collection: by culture, MRSA was detected in 10 (3.3%) samples, while by qPCR MRSA was detected in 18 (6.0%) samples (p = 0.04) (Table 1 and Fig. 2).

Proportion of MRSA carriers (adults >60 years old) detected by classical culture-based methods and qPCR. Red bars, carriers living in nursing homes; blue bars, carriers living in family home. CCBM, classical culture-based methods. Color images are available online.
Detection of Methicillin-Resistant Staphylococcus aureus Carriers According to Sampling Site and Methodology Used
p in bold represents statistically significant values.
p-Values determined using McNemar's chi-square test for paired individuals.
NP, nasopharynx; OP, oropharynx; qPCR, quantitative real-time PCR.
MRSA carriage in nursing homes and family homes
In both groups of individuals, we observed that the geometric Ct mean was not significantly different between positive nasopharyngeal samples and positive oropharyngeal samples (p = 0.092 for nuc; p = 0.965 for mecA), suggesting that both anatomical sites were colonized at comparable MRSA densities.
Nevertheless, Ct values for nuc gene were significantly lower in samples from adults living in nursing homes than in samples from adults living in the family homes (p < 0.001) indicating higher density of S. aureus colonization in the former case. On the contrary, Ct values for the mecA gene were not significantly different between samples from both collections (p = 0.069) (Fig. 1 and Supplementary Table S2), suggesting that colonization by MRSA occurred at a comparable density.
When results of the two sampling sites were combined, the use of a semi-selective enrichment medium followed by qPCR, compared with culture-based methods, improved detection of MRSA carriers from 5.4% to 8.0% in the nursing home collection and from 0.3% to 1.7% in the family home collection (Table 1). However, probably due to the low number of positive results, these increases were not statistically significant. In fact, when results from the two collections were analyzed together, the use of a semi-selective enrichment medium followed by qPCR improved significantly the detection of MRSA carriers compared with CCBM [from 17 (2.8%) to 29 (4.8%), p = 0.03].
Characteristics of MRSA isolates
Overall, 40 samples were positive for MRSA by culture and/or by qPCR (18 from oropharyngeal samples and 22 from nasopharyngeal samples; Table 1 and Supplementary Table S3). From these, pure MRSA cultures were obtained from 38 samples and were further characterized. For two MRSA samples detected by semi-selective enrichment medium followed by qPCR, we were not able to obtain a pure culture. All isolates were found to be related to three HA-MRSA epidemic clones: 19 (50.0%) isolates were related to the New York/Japan clone, 17 (44.7%) belonged to the Pediatric clone, and 2 (5.3%) belonged to the EMRSA-15 clone (Table 2). The six MRSA carriers yielding both a positive nasopharyngeal and oropharyngeal sample carried the same strain in both samples.
Characteristics of the 38 Methicillin-Resistant Staphylococcus aureus Isolates Carried by Adults Aged >60 Years
Fifteen isolates from the nursing home collection and four isolates from the family home collection.
CC, clonal complex; MLST, multilocus sequence typing.
Discussion
In Portuguese hospitals, MRSA prevalence is among the highest in Europe. 6 By contrast, previous studies suggested that its prevalence in the community is very low and is associated with well-defined risk groups.18–20 We used an enrichment step followed by qPCR, to investigate MRSA carriage in nasopharyngeal and oropharyngeal paired samples obtained from adults >60 years of age living in nursing homes or in family homes. We compared results with those obtained using CCBM.
In agreement with previous studies, we observed that the use of a semi-selective medium increased detection of MRSA in the NP and OP both among individuals living in family homes and in nursing homes. Compared with previous estimations based on CCBM, the current strategy increased detection by an average of 1.5-fold of MRSA carriers in the nursing home collection and by an average of 6-fold of MRSA carriers in the family home collection. Still, MRSA carriage prevalence was relatively low in both groups: 8.0% among individuals living in nursing homes and 1.7% among individuals living in family homes. These findings are similar to the ones described in studies from Brazil, Malta, and United States that estimated a prevalence of MRSA ∼2%, 5%, and 8%, respectively, among elderly adults living in the community.33–35
We also observed that the combined use of nasopharyngeal and oropharyngeal swabs increased detection of MRSA as concordance between sampling sites was not high. Nevertheless, the nasopharyngeal swab alone enabled significantly higher detection of MRSA carriers than the oropharyngeal swab in the nursing home collection (in the family home collection the numbers were too low to draw conclusions). As density of colonization was comparable in both sites, the results suggest that the NP may be a preferred colonization niche compared with the OP.
In our study, we detected MRSA by qPCR that were not detected by culture-based approaches. This is not unexpected, given the significantly higher sensitivity of qPCR.36,37 High Ct values correlate well with low bacterial density, which may be too low to be detected by culture. The biological relevance of MRSA carriers detected by qPCR only (with negative cultures) is unclear, as the DNA detected might be from dead bacteria or from bacteria at low density. Nevertheless, these individuals should be considered MRSA carriers since their sample contained DNA from MRSA, indicating that, at a given time point, they carried it.
Genotyping of MRSA isolates identified three HA-MRSA clones widely disseminated in Portuguese hospitals with no evidence for specific CA-MRSA clones in circulation.
Our study has some limitations. First, samples from the anterior nares were not obtained despite the fact that this is considered to be the preferential human niche. 1 This was due to the fact that the study was nested in another one aimed to detect Streptococcus pneumoniae. Still, it is known that S. aureus colonizes multiple human body sites (skin, perineum, pharynx, axillae, among others), and is a frequent colonizer of the NP and the OP.1,18,19 Second, this study was done 8 years after the original study. We observed that some of the originally frozen swabs—containing either MRSA or MSSA—had lost viability. As this apparently occurred indiscriminately, we consider the conclusions were not affected.
One strength of our study was the use of paired samples for all individuals, which improved detection of MRSA. The combination of an enrichment step with qPCR also increased the detection of MRSA compared with culture alone. In addition, we were able to isolate 38 MRSA strains from the 40 qPCR-positive samples allowing culture confirmation of results and genotyping of the strains.
Conclusions
In conclusion, the use of selective enrichment combined with qPCR does not change the overall scenario previously described in Portugal: MRSA circulation in the elderly is low and is associated with HA-MRSA clones.
Footnotes
Acknowledgments
We are grateful to all the participants who collaborated in the study. We thank Anabela Gonçalves, Pedro Fonseca, Idalina Valadares, Sara Martins, and Ana Morais for collecting the nasopharyngeal and oropharyngeal samples. We are grateful to Ana Paula Ribeiro from Câmara Municipal de Montemor-o-Novo.
Authors' Contributions
The study was conceived by R.S.-L. Experiments were performed by S.T.A. Statistical analyses were done by A.C.P. Data interpretation was done by S.T.A. and R.S.-L. R.S.-L. and H.d.L. contributed with reagents and materials. The article was written by S.T.A. and R.S.-L., and critically revised by all authors. All authors read and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was partially supported by Projects LISBOA-01-0145-FEDER-007660 (Microbiologia Molecular, Estrutural e Celular, funded by FEDER funds through COMPETE2020- Programa Operacional Competitividade e Internacionalização (POCI) and LISBOA-01-0145-FEDER-016417 (ONEIDA project, co-funded by FEEI—“Fundos Europeus Estruturais e de Investimento” from “Programa Operacional Regional Lisboa 2020”). S.T.A. and A.C.P. were supported by grants SFRH/BD/108380/2015 and SFRH/BPD/99638/2014 from Fundação para a Ciência e a Tecnologia, Portugal.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.