
Abstract
We investigated the in vitro susceptibility of ceftazidime-avibactam (CZA) resistant Stenotrophomonas maltophilia to the associations aztreonam/amoxicillin-clavulanate (ATM-AMC) and ATM-CZA. Forty clinical isolates of S. maltophilia recovered from sputum samples of 40 cystic fibrosis people were selected from the collection of the Nantes University Hospital, based on their resistance to CZA. Minimum inhibitory concentrations (MICs) of ATM-CZA and ATM-AMC were determined for each isolate by an Etest strip superposition method, and by Etest for each individual antibiotic. MICs of CZA, ATM, and AMC ranged from 12 to ≥256, ≥256, and 16 to ≥256 mg/L, respectively. Synergistic effects were observed with the ATM-CZA combination for all isolates (fractional inhibitory concentration index range of 0.01 to 0.27), with combination MICs ranging from 0.75 to 16 mg/L (MIC50/90 = 3/12 mg/L), corresponding to a decrease of at least 16-folds in the MIC of ATM. In 23 (57.5%) S. maltophilia isolates, the association of AMC to ATM was also synergistic and combination MICs were ≤16 mg/L (EUCAST breakpoint for ATM resistance in Pseudomonas aeruginosa). Our results show that ATM-CZA or ATM-AMC could be alternative therapeutic options against some highly resistant S. maltophilia. This encourages further experimental studies, in particular time-kill analyses, and clinical trials to delineate conditions required for use of these combinations in practice.
Introduction
The environmental and opportunistic bacterium Stenotrophomonas maltophilia has been increasingly recognized as a true respiratory pathogen, especially in cystic fibrosis (CF) people with advanced lung disease.1–4 In these individuals, the use of long-course and repeated antipseudomonal therapies may promote S. maltophilia proliferation in lung, as this Gram-negative bacillus exhibits intrinsic resistance to different classes of antibiotics used in clinical practice, such as aminoglycosides and carbapenems.1–4 The resistance to β-lactams in S. maltophilia primarily involves two inducible chromosomally encoded β-lactamases, L1 and L2. L1 is a zinc-dependant carbapenemase (Ambler subclass B3), which is not inhibited by serine-β-lactamase inhibitors such as clavulanic acid and avibactam, and which hydrolyzes carbapenems and other β-lactams, with the exception of the monobactam aztreonam (ATM). L2 is a clavulanic acid- and avibactam-sensitive β-lactamase (Ambler class A) that confers resistance to penicillins, first- to third-generation cephalosporins, and ATM.1,2,5,6 Few therapeutic options are currently available for treating S. maltophilia infections, the most commonly used being the non-β-lactam antibiotics trimethoprim-sulfamethoxazole and fluoroquinolones like levofloxacin or moxifloxacin, which expose to the risk of more adverse effects than β-lactams.7,8 Historically, ticarcillin-clavulanate and ceftazidime were also effective agents against clinical strains of S. maltophilia. However, ticarcillin-clavulanate is no longer produced worldwide. In addition, an increasing trend in resistance toward ceftazidime has been observed in recent years through the emergence of various adaptive mutational events leading to β-lactamase overexpression, conformational changes in L1 and L2 residues associated with ligand binding, or overproduction of efflux transporters.5,9
Combinations of ATM plus serine-β-lactamase inhibitors (clavulanic acid or avibactam) were found to exhibit synergistic activity against S. maltophilia, although there are currently limited data on the ATM/amoxicillin-clavulanate (AMC) combination against ceftazidime-avibactam (CZA) resistant strains.10,11 Compared to CZA, AMC offers the advantage to be a markedly cheaper with a narrower spectrum antibiotic that can be administered orally. Hence, the aim of this study was to compare the in vitro activity of associations ATM-AMC and ATM-CZA against 40 clinical isolates of CZA-resistant S. maltophilia from 40 CF individuals.
Materials and Methods
The present work was approved by the Nantes University Hospital Institutional Review Board. This study was retrospective and no patient identification was performed during data collection.
Clinical characteristics of the isolates
The isolates of S. maltophilia tested in this study (n = 40) were recovered from sputum samples of 40 CF individuals 2 to 55 years of age (median of 21 years), followed from June 2017 to January 2022 at Nantes University Hospital (France). Isolates were selected from the collection of the microbiology laboratory, if they were resistant to CZA (interpretation was made according to the EUCAST breakpoints established for Pseudomonas aeruginosa (version 2019 V.9.0), with a cutoff value of >8 mg/L (resistant)). 12 Only one isolate per patient was incorporated into the study.
Susceptibility testing
Isolates were stored frozen and subcultured onto chocolate agar plates for purity check before subsequent testing. Minimum inhibitory concentrations (MICs) of ATM, AMC, and CZA were determined by Etest MIC strips (BioMérieux SA, Marcy l'Etoile, France), according to the EUCAST guidelines. 12 To evaluate the antimicrobial activity of ATM-AMC and ATM-CZA combinations, the Etest strip superposition method was used, as previously described. 10 Briefly, Mueller-Hinton agar plates were inoculated with 0.5 McFarland suspensions of S. maltophilia and the strips of AMC or CZA were applied for 30 minutes, and then removed. The ATM strip was subsequently deposited at the exact same place.
The concentration ranges for the Etest were 0.016–256 mg/L for ATM, AMC (with a fixed clavulanate concentration of 2 mg/L), and CZA (with a fixed avibactam concentration of 4 mg/L). For MIC interpretation, the EUCAST breakpoints established for P. aeruginosa (version 2019 V.9.0) were used, with a cutoff value of ≤16 mg/L (susceptible) for ATM alone and in combination. 12 Combination MICs were also analyzed using the CLSI breakpoints for P. aeruginosa, with a cutoff value of ≤8 mg/L (susceptible) for ATM alone and in combination. 13
A fractional inhibitory concentration index (FICI) was calculated for each combination by using the following formula: FICA + FICB = FICI, where FICA equals the MIC of drug A in combination divided by the MIC of drug A alone and FICB equals the MIC of drug B in combination divided by the MIC of drug B alone. The Etest results with one-half increment were rounded up to the next highest twofold dilution before FICI calculations. The FICIs were interpreted as follows: synergy if FICI ≤0.5, additivity if 0.5 < FICI ≤1.0, indifference if 1.0 < FICI ≤4.0, and antagonism if FICI >4.0.
Results
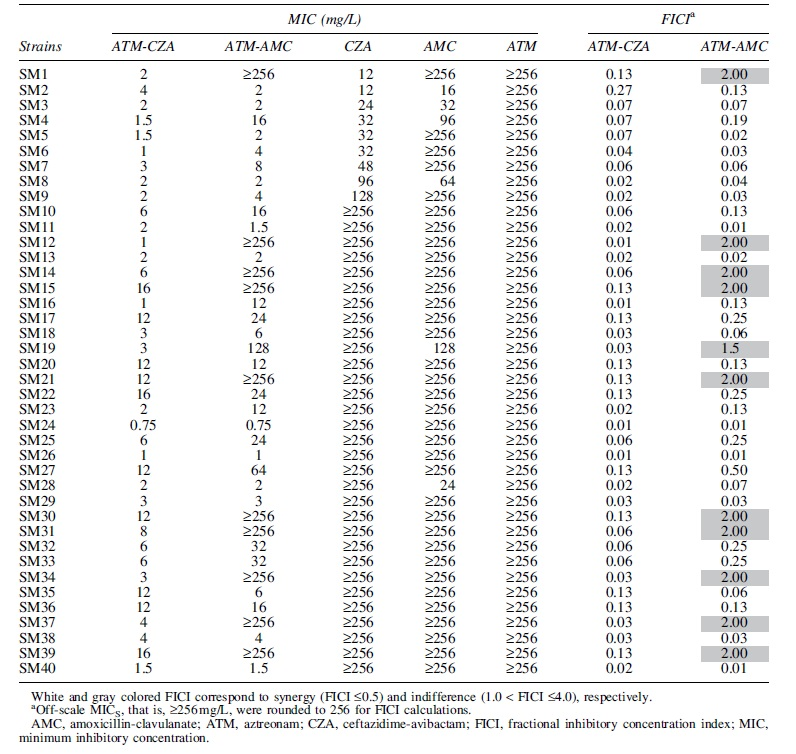
Results of MICs for ATM, AMC, CZA, and combinations of ATM-AMC or ATM-CZA are presented in Table 1. All tested isolates exhibited high levels of MICs for CZA (MIC range, 12 to ≥256 mg/L), ATM (MIC values ≥256 mg/L), and AMC (MIC range, 16 to ≥256 mg/L). MICs of ATM-AMC and ATM-CZA combinations ranged from 0.75 to ≥256 mg/L (MIC50/90 = 12/≥256 mg/L), and 0.75 to 16 mg/L (MIC50/90 = 3/12 mg/L), respectively. As shown in Fig. 1, MIC distribution was very wide for the ATM-AMC combination with a peak at ≥256 mg/L (10 isolates), while distribution was bimodal, but tighter for ATM and CZA. Synergistic effects were observed with the ATM-CZA combination for all isolates (FICIs ≤0.5), with MICs of ATM reduced at least 16-folds. The ATM-AMC combination showed less synergistic effects, as an indifference (1.0 < FICI ≤4.0) was found for 11 (27.5%) isolates (Table 1).
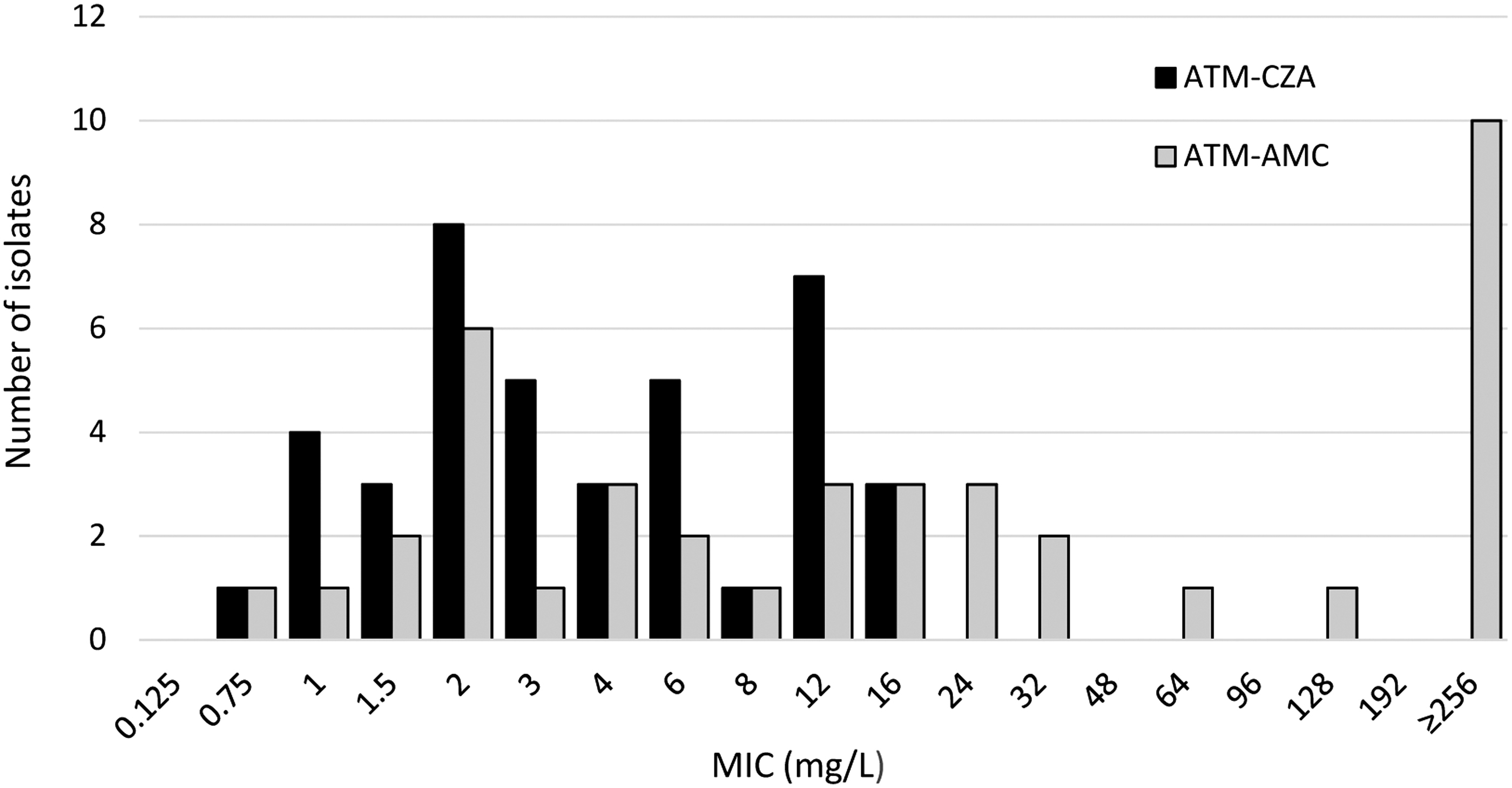
Distribution of ATM-AMC (gray) and ATM-CZA (black) MICs assessed by an Etest strip superposition method for the set of 40 CZA-resistant Stenotrophomonas maltophilia isolates from this study. AMC, amoxicillin-clavulanate; ATM, aztreonam; CZA, ceftazidime-avibactam; MICs, minimum inhibitory concentration.
Minimum Inhibitory Concentrations Measured by Etest for Aztreonam Combined with Ceftazidime-Avibactam or Amoxicillin-Clavulanate, and for Each Individual Agent, Against the 40 Stenotrophomonas maltophilia Clinical Isolates from This Study
Discussion
This study compared the in vitro activity of ATM-AMC and ATM-CZA combinations against 40 strains of S. maltophilia recovered from 40 CF individuals. There are currently no clinical guidelines for the management of S. maltophilia in CF, and the pathogenicity of this species in acute pulmonary exacerbations is still to be understood. 7 Hence, health care professionals need to use their clinical judgment when deciding whether or not to treat transient or chronic infections with S. maltophilia.
Since this organism has been associated with pulmonary exacerbations in some studies, and also because S. maltophilia is often multidrug resistant, it may encourage clinicians to prescribe broad-spectrum antibiotic therapies.7,8 A number of recent studies have underlined an alarming trend in S. maltophilia resistance toward trimethoprim-sulfamethoxazole and fluoroquinolones, which have traditionally been considered the first-line antimicrobial treatments.5,6,8 Few alternative strategies have shown good in vitro activity against resistant S. maltophilia, among which are tetracycline derivatives like minocycline, colistin, cefiderocol, and ATM in combination with CZA.8,10,11,14–16
In this study, by using an Etest strip superposition method, we confirmed the synergism of the association ATM and CZA against 40 CZA-resistant S. maltophilia with FICI scores from 0.01 to 0.27 and combination MICs lower than or equal to the EUCAST breakpoint usually considered for ATM alone against P. aeruginosa (16 mg/L) (version 2019 V.9.0). 12 However, it should be noted that 25% (10/40) of the strains showed ATM-CZA combination MICs of 12 or 16 mg/L, thus exceeding the CLSI breakpoint of ATM against P. aeruginosa (sensitive if MIC ≤8 mg/L). 13 This decreased susceptibility, already noticed in a few strains of previous studies, could be explained by the simultaneous overexpression of the intrinsic β-lactamases (L1 and/or L2) and efflux transporters.11,14
Beyond this, our Etest strip superposition method showed that the association of AMC to ATM was also synergistic against 29 (72.5%) S. maltophilia (FICI range of 0.01 to 0.25), but sole 23 (57.5%) and 17 (42.5%) isolates had combination MICs ≤16 or 8 mg/L, respectively. The synergistic activity of ATM plus clavulanate against S. maltophilia had already been reported in other in vitro susceptibility studies, especially for the ticarcillin-clavulanate and ATM combination.17–20 García-Rodríguez et al. were the first to describe a synergy between ATM and clavulanate, but only at certain ratios (mainly 2:1). In their study, MICs of ATM-clavulanate (2:1) and AMC-ATM (2:1:2) were similar, ranging from 0.5 to 8 mg/L (MIC50/90 = 1/2 mg/L) for the 42 strains tested by an agar dilution method. 17
Then, Muñoz Bellido et al. confirmed the high level of activity of ATM-clavulanate (2:1) against 32 strains of S. maltophilia in vitro, and showed that this activity was even increased twofold to fourfold by the addition of ticarcillin, although not by the addition of amoxicillin or piperacillin. 18 In the study of Krueger et al., the synergism of ATM-clavulanate was observed for a constant concentration of clavulanate (2 mg/L), with MIC50/90 = 4/16 mg/L for the 23 strains tested. 19 More recently, comparisons to novel β-lactamase inhibitors (avibactam, vaborbactam, and bicyclic boronate) have been conducted.6,10,11 Thus, by performing kinetic and structural studies with purified L1 and L2 β-lactamases, Calvopiña et al. showed that clavulanate, unlike avibactam and bicyclic boronate, induced L1 production, but all three inhibitors restored ATM susceptibility, even when L1/L2 was hyperproduced. 6
By using the same method as here, Emeraud et al. found that ATM-AMC was as efficient as ATM-CZA not only against five S. maltophilia isolates but also against metallo-β-lactamase-producing Enterobacteriaceae or P. aeruginosa. 10 However, a recent study from Biagi et al. that compared the in vitro activity of ATM in combination with clavulanate (2 mg/L), avibactam (4 mg/L), relebactam (4 mg/L), or vaborbactam (8 mg/L) against 47 S. maltophilia, including 35/47 (74.5%) CZA-nonsusceptible isolates, found that avibactam reduced ATM MICs to the greatest degree and restored susceptibility in the highest number of isolates (97.8%), followed by relebactam (71.3%), clavulanate (60.8%), and then vaborbactam (15.2%). 11
To date, methodologies to be adopted when testing AMC in vitro are still a matter of debate. EUCAST indicates the use of a fixed 2 mg/L clavulanate concentration, while CLSI recommends a 2:1 ratio with the downside that some high clavulanate concentrations, far above those that can be achieved in vivo (>2 mg/L), are tested. 21 In this work, Etest strips with fixed concentrations of clavulanate (2 mg/L) or avibactam (4 mg/L) were used. Our findings fall in line with the results of Biagi et al. achieved by a broth microdilution method, showing a better synergistic effect of the ATM-CZA combination compared to the ATM-AMC combination. 11
In this study, we used a technique that is easy to implement routinely. However, more labor-intensive time-kill experiments able to detect bactericidal activities and bacterial re-growth over time would be required to provide more accurate data regarding the effect of both combinations and confirm these results. Further pharmacokinetic/pharmacodynamic approaches will be necessary to identify precisely the optimal conditions for the inhibition of ATM degradation by CZA or AMC, generate information on the appropriate dosing regimen and mode of administration of the drugs in human, and establish which methodology and interpretive criteria to use in vitro for predicting the activity of those combinations in CF people. 22
In conclusion, this study shows that ATM combined with CZA could be a potential therapeutic option against multidrug-resistant S. maltophilia and merits clinical evaluation. The combination based on ATM and AMC exerted less promising in vitro activity against S. maltophilia isolates tested in this study.
Footnotes
Authors' Contributions
All authors read and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.