
Abstract
Antibiotic combinations remain the frontline therapy for severe infections to reduce mortality. However, conventional antibiotic combinations have some limitations such as the low bioavailability and the rise of resistant strains. Nanoparticles are increasingly used as antibiotic delivery systems to promote bioavailability and hence improve efficacy of antibiotics. In this work, we hypothesize that the simultaneous delivery of two antibiotic-loaded nanoparticles will improve the intracellular bioavailability and thus inhibit emergence of resistance. Accordingly, Chitosan–pluronic nanoparticles were used to construct nanosized ciprofloxacin and meropenem and the antibacterial activity of nanosized combined antibiotics were compared versus unloaded single, unloaded combined, and nanosized single antibiotics. Thirty-six stepwise mutants were selected by exposing two E. coli strains to increasing concentrations of free-unloaded and nanosized antibiotics, and mutants were tested for antimicrobial susceptibilities using broth microdilution and disc diffusion methods. The change in expression levels of acrB efflux pump and porins (ompC and ompF) was assessed by real-time reverse transcription–PCR. The in vitro evaluation of combined ciprofloxacin and meropenem-loaded nanoparticles demonstrated that this nanosystem exhibited enhanced antibacterial effect. Step mutants selected with nanosized combined antibiotics showed higher sensitivity to both drugs, exhibited lower mutation frequencies, and less cross-resistance to other antimicrobial classes. Moreover, for all steps of selection, nanosized combined antibiotic mutants expressed significantly lower levels of acrB as well as higher levels of ompC and ompF (p-value <0.01). In view of these results, the use of nanosized combined antibiotics may be considered among the new promising strategies to combat infections through their potential efficacy in reducing microorganisms' ability to form resistant mutants.
Introduction
The rapid emergence of multidrug-resistant (MDR) bacteria is an urgent global public health threat, indicating that monotherapy is increasingly no longer adequate to treat these infections. Antibiotic combinations are widely studied as an alternative approach to combat MDR bacteria arising from monotherapy. 1 Potential achievements with combinations as compared with monotherapy include expansion of the spectrum of antimicrobial coverage, synergistic effects with improved efficacy, and decreased risk for emergence of resistance. 2

Meropenem and ciprofloxacin together form an appealing combination; as each antibiotic has an excellent safety profile, and the combination produces a significantly higher killing rate than either drug used solely. This combination produced clinically relevant synergy against challenging microorganisms as Pseudomonas, Acinetobacter, and Klebsiella.3–5 One drawback of such combination is that both drugs induce overexpression of acrAB efflux pump as well as reduction in expression of outer membrane proteins, ompF and ompC, hence promote cross-resistance to other antimicrobials.6,7 Moreover, the low bioavailability of conventional antibiotics poses additional risk for development of resistant bacteria during therapy. 8 Consequently, in some cases, combined meropenem and ciprofloxacin therapy might be associated with increased risk of selection of resistant strains. 9
A novel appealing strategy to resolve antimicrobial resistance is the encapsulation of antibacterial drugs within nanosized material. Nanosystems used for antibiotic delivery render some benefits over conventional formulations possibly through increasing the intracellular bioavailability of antimicrobial agents thus suppressing the development of resistant mutants.8,10 Furthermore, nanosized antibiotics represent a potential candidate to block efflux pumps of bacterial cells as well.11,12 Our recent work demonstrated that nanosized levofloxacin is superior to unloaded levofloxacin in reducing emergence of antimicrobial resistance in E. coli. 13 The present study aimed to compare the antimicrobial activity of nanosized combined ciprofloxacin and meropenem versus that of nanosized single, unloaded single, and unloaded combined drugs. Moreover, to explore the change in expression of acrAB efflux pump and porins in stepwise mutants that emerge upon exposure of susceptible E. coli to all formulations.
Materials and Methods
Materials
Chitosan (CS), sodium tripolyphosphate (TPP), and Pluronic F127 (Fisher Scientific Co., Pittsburgh, PA) were used to construct the nanoparticles. Meropenem was purchased from AK Scientific, Inc., (Union City, CA), and ciprofloxacin was purchased from Sigma-Aldrich Co. (St. Louis, MO). Ciprofloxacin and meropenem-loaded CS/TPP/Pluronic F127 nanoparticles were constructed as by the ionic gelation method and micellar formation as described previously. 14
Bacterial strains
Two E. coli strains were used in this study: E. coli reference strain ATCC 25922 (EC 1 ; American Tissue Cell Culture, Manassas, VA), and a clinical E. coli isolate (EC 2 ) obtained from the Medical Microbiology Laboratory, Faculty of Medicine, Assiut University. The two isolates were fully susceptible to all antimicrobial classes. The minimal inhibitory concentrations (MICs) of ciprofloxacin, meropenem, nanosized ciprofloxacin and nanosized meropenem were determined by broth microdilution method according to the Clinical and Laboratory Standards Institute (CLSI) guidelines. 15 The study is exempt from IRB approval according to the IRB regulations.
In vitro selection of the resistant mutants
E. coli mutants were obtained by culturing the two parental E. coli strains on progressively increasing concentrations of each of the tested free or nanosized formulations, as previously described. 16 First-step mutants were defined as the mutants grown on the highest concentration of each formulation. Second- and third-step mutants were selected in the same way by choosing the mutants exhibiting the highest MIC during the first and second steps of mutation selection, respectively. After each selection step, two representative mutants were collected and stored at −80°C until further analysis.13,16
Mutation frequency
Mutation frequencies were calculated from the ratio of the number of mutant colonies grown on drug-containing plates (the MIC value of ciprofloxacin and/or meropenem free and nanosized—for each E. coli strain that was used to obtain the successive first-, second-, or third-step mutants) to the total viable count grown on drug-free plates. Each test was done in duplicate and the mutation frequency was calculated as the mean of the frequencies in the two experiments. 17
Antimicrobial susceptibilities of E. coli mutants
The MICs of ciprofloxacin and meropenem (free or nanosized) for E. coli step mutants were determined by broth microdilution method according to CLSI guidlines. 15 Antimicrobial resistance patterns of all step mutants were determined using the Kirby-Bauer method according to CLSI guidlines. 15 The antibiotic resistance phenotype was classified as no drug resistance (NDR), single-drug resistance (SDR; resistant to only one drug class), or multidrug resistance (MDR; resistant to two or more unrelated drug classes). E. coli ATCC 25922 was used for quality control purposes. 13
Relative quantification of efflux pump and porin genes' expression
The relative quantification of acrB, ompF, and ompC genes' expression was determined in parental EC 2 strain and its step mutants using quantitative real-time reverse transcription–PCR (qRT-PCR). The primers used (Table 1) were chosen from genetic codes published in GenBank. RNA extraction, purification, and reverse transcription of RNA into cDNA were done as previously described. 6 The amplification of cDNA templates by RT-qPCR was performed in a CFX96 Touch Real-Time PCR Detection System (Bio-Rad, CA) using a SYBR Green RT-PCR Kit (Promega). The expression of each gene was normalized to that of a ribosomal housekeeping gene (gapA). The relative expression of each target gene was calibrated against the corresponding expression by E. coli ATCC 25922 (expression = 1), which served as the control. All qPCR reactions were done in triplicates and values were calculated as the mean of the three expression levels.
Primers and Annealing Temperature
Statistical analysis
GraphPad Prism software was used for statistical analysis (Version 6.01; GraphPad, San Diego, CA). For all tests, a p-value of <0.1 was deemed week significant, a p-value of <0.01 strong significant, and p-value <0.001 very strong significant.
Results
Mutation frequency
The frequencies of mutations emerged upon stressing E. coli with each of the six formulations are demonstrated in Table 2. Mutations' frequencies were lower upon treatment with nanosized drugs versus free drugs whether single or in combination. Mutation frequencies ranged from 1.1 × 10−4 to 6.2 × 10−3 and from 1.6 × 10−4 to 2.4 × 10−3 for free ciprofloxacin mutants (Cm) and free meropenem mutants (Mm), respectively, whereas ranged from 5.2 × 10−8 to 1.6 × 10−6 and from 7 × 10−9 to 5.4 × 10−8 for nanosized ciprofloxacin mutants (NCm) and nanosized meropenem mutants (NMm), respectively. Meanwhile, the frequency of mutations selected with free combined drugs (CMm) ranged from 1.3 × 10−5 to 7.5 × 10−3, whereas from 1.6 × 10−9 to 1 × 10−8 for nanosized combined drug mutants (NCMm). For the three steps of selections, resistant mutants emerged at a lower frequency when E. coli was treated with nanosized combined drugs.
Mutation Frequencies in Stepwise Escherichia coli Mutants Using All Formulations
Cm, ciprofloxacin-selected mutants; CMm, combined ciprofloxacin and meropenem-selected mutants; EC 1 , E. coli reference strain ATCC 25922; EC 2 , clinical E. coli isolates; Mm, meropenem-selected mutants; NCm, nanosized ciprofloxacin-selected mutants; NCMm, nanosized combined ciprofloxacin and meropenem-selected mutants; NMm, nanosized meropenem-selected mutants.
Antimicrobial susceptibility of E. coli mutants to unloaded ciprofloxacin and meropenem
The basal MICs of the two parental strains were 0.008 mg/L for ciprofloxacin and 0.008 mg/L for meropenem (Table 3). Ciprofloxacin MICs for Cm ranged from 0.5 to 64 mg/L, whereas ranged from 0.5 to 32 mg/L for Mm, and meropenem MICs for Cm ranged from 1 to 16 mg/L, whereas in Mm ranged from 0.25 to 4 mg/L. However, MICs for CMm ranged from 0.016 to 4 mg/L for ciprofloxacin (8–16-fold decrease) and 0.016 to 2 mg/L for meropenem (2–8-fold decrease).
Minimal Inhibitory Concentrations of Unloaded Ciprofloxacin and Meropenem for All Selected Mutants
MIC, minimal inhibitory concentration.
Resistance to ciprofloxacin (MIC ≥1 mg/L) started to appear in all second-step mutants selected with either ciprofloxacin or meropenem, but only in EC 2 second-step mutant selected with free combined antibiotics. Moreover, the levels of ciprofloxacin resistance in monotherapy-selected mutants were moderate–high (8–64 mg/L), while mutants selected with combined drugs expressed only low-level resistance (1–4 mg/L). On the other hand, resistance to meropenem (MIC ≥4 mg/L) began in second-step Cm (EC 2 ), and in third-step Mm, whereas all CMm retained susceptibility to meropenem.
Antimicrobial susceptibility of E. coli mutants to nanosized ciprofloxacin and meropenem
The basal MICs of the two parental strains ranged from 0.001 to 0.002 mg/L for nanosized ciprofloxacin and were 0.001 mg/L for nanosized meropenem (Table 4). Nanosized ciprofloxacin MICs for NCm ranged from 0.016 to 8 mg/L, whereas ranged from 0.063 to 4 mg/L for NMm. Furthermore, nanosized meropenem MICs for both NCm and NMm ranged from 0.016 to 1 mg/L. On the contrary, MICs of NCMm ranged from 0.004 to 2 mg/L for nanosized ciprofloxacin (two to fourfold decrease) and 0.002 to 0.5 m/L for nanosized meropenem (twofold decrease). Resistance to nanosized ciprofloxacin emerged in EC 2 seconnd-step NCm and NMm, but only in third-step NCMm. On the contrary, all mutants selected with nanosized drugs were susceptible to nanosized meropenem.
Minimal Inhibitory Concentrations of Nanosized Ciprofloxacin and Meropenem for All Selected Mutants
Mutants emerged after stressing with combination therapy, whether free or nanosized, were more sensitive to both meropenem and ciprofloxacin than monotherapy step mutants. Furthermore, NCMm showed higher susceptibility to ciprofloxacin and meropenem than CMm. For all step mutants, ciprofloxacin MICs and meropenem MICs were lower for NCMm (nanosized ciprofloxacin MIC = 0.004–2 mg/L and nanosized meropenem MIC = 0.002–0.5 mg/L) than MICs for CMm; ciprofloxacin MIC = 0.016–4 mg/L (twofold more) and meropenem MIC = 0.016–2 mg/L (fourfold more).
Antimicrobial resistance profile of E. coli mutants
Parental isolates, as well as first-step mutants selected with either mono or combined nanosized drugs, were fully susceptible to all the tested drugs (NDR). The first evidence of resistance was SDR (SDR, 1 resistance only to β-lactams) that appeared in first-step Cm, Mm, and CMm. With further selection steps, there was an increase in the number of antibiotic drugs to which resistance developed (Table 5).
The Change of Resistance Phenotype in Stepwise Escherichia coli Mutants
MDR, multidrug-resistant; NDR, no drug resistance; SDR, single-drug resistance.
Interestingly, after three steps of selection, all mutants selected with free drugs both single and combined expressed cross-resistance to all drug classes (XDR; extreme drug resistance). Conversely, mutants selected with nanosized drugs, both single and combined, expressed less MDR phenotype and retained susceptibility to carbapenems and aminoglycosides.
Expression levels of efflux pump and porin genes
Testing of acrB expression in parental EC 2 strain and its stepwise mutants showed that all mutants exhibited higher level of gene expression than the parental strain. Moreover, regardless of the type of treatment, the acrB expression levels increased gradually from first-step mutants through second-step mutants until it reached the highest level in third-step mutants. Generally, the acrB expression levels were lower in nanosized drug-selected mutants (ranging from 0.106 to 0.300 in first mutants, 0.186–0.810 in second mutants, and 0.590–0.913 in third mutants) than free drug-selected mutants (0.213–0.753 in first mutants, 0.859–2.266 in second mutants, and 1.421–2.438 in third mutants). Also, acrB expression levels were lower in mutants selected with free combined drug (0.213–1.421 for CMm and 0.106–0.590 for NCMm) than in monotherapy-selected mutants (0.325–2.438 for free drugs and 0.229–0.913 for nanosized drugs).
Additionally, acrB expression levels were low in all step-NCMm (0.106 in first mutants, 0.186 in second mutants, 0.590 in third mutants) in comparison to levels in CMm (0.213 in first mutants, 0.859 in second mutants, 1.421 in third mutants). For all steps of selection, NCMm expressed significantly lower levels of acrB (p-value <0.01) (Fig. 1).
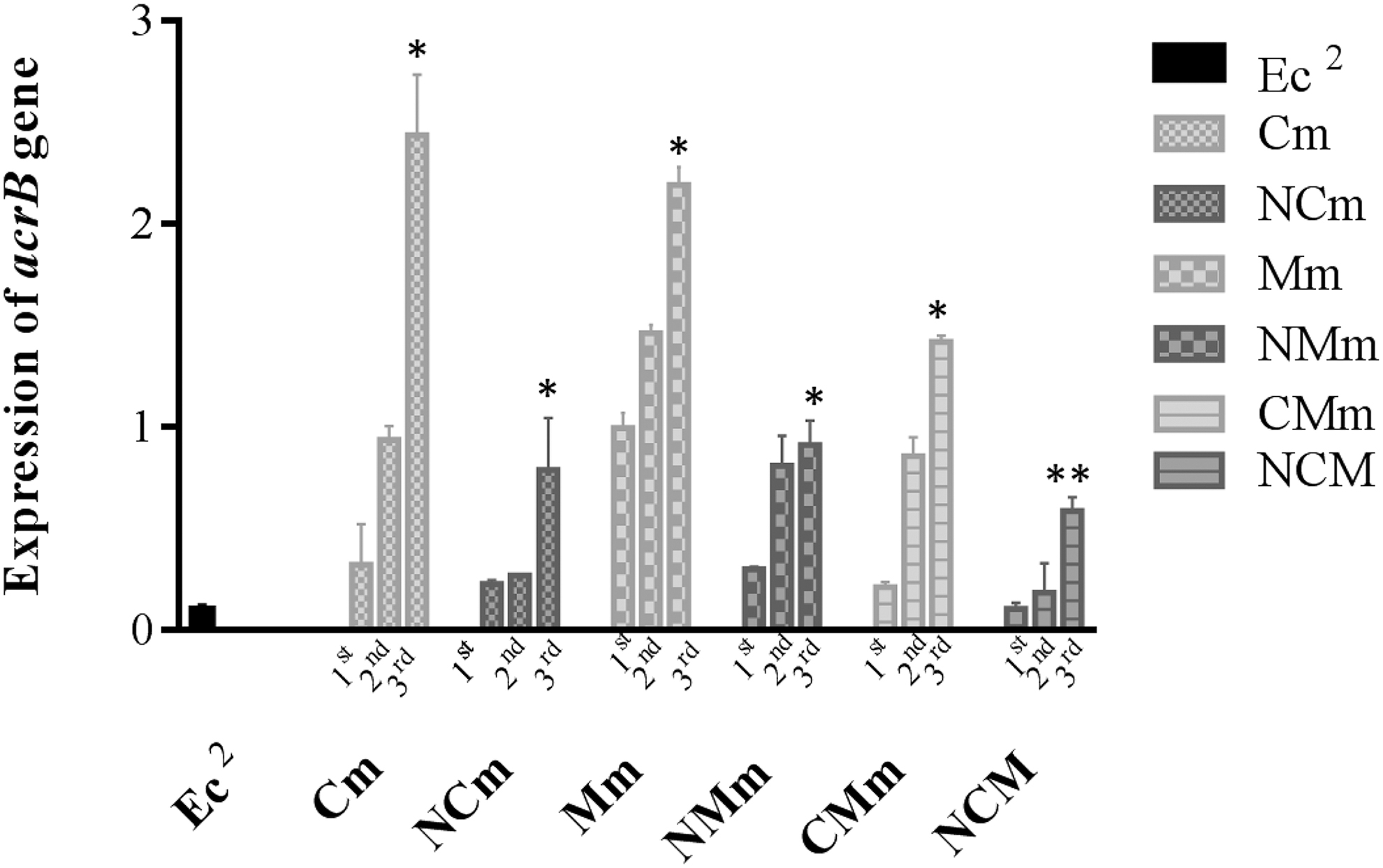
Expression of acrB in parental EC 2 strain and its step mutants. ***p-value <0.001, **p-value <0.01, *p < 0.1. The values are presented as mean ± SD (n = 3). Cm, free ciprofloxacin mutants; CMm, free combined ciprofloxacin and meropenem mutants; EC 2 , clinical E. coli isolates; Mm, free meropenem mutants; NCm, nanosized ciprofloxacin mutants; NMm, nanosized meropenem mutants; NCMm, nanosized combined ciprofloxacin and meropenem mutants; SD, standard deviation.
On the other side, ompC and ompF expression levels decreased gradually from first-step mutants through second-step mutants until they reach the lowest level in third-step mutants. Overall, ompC expression levels were higher in mutants selected with nanosized drugs (ranging from 0.653 to 0.977 in first mutants, 0.109–0.804 in second mutants, and 0.018–0.668 in third mutants) than in mutants selected with free drugs (0.292–0.864 in first mutants, 0.007–0.240 in second mutants, and 0.004–0.022 in third mutants). Also, ompC expression levels were higher in mutants selected with free combined drugs (0.022–0.864 for free combined drugs and 0.668–0.977 for nanosized combined drugs) versus those selected with monotherapy (0.004–0.339 for free drugs and 0.018–0.791 for nanosized drugs). Regarding the combined drug formulations, ompC expression levels were higher in NCMm (0.668–0.977) than in CMm (0.022–0.864). Again, for all steps of selection, NCMm expressed significantly higher level of ompC (p-value <0.01) (Fig. 2).

Expression of ompC in parental EC 2 strain and its step mutants. ***p-value <0.001, **p-value <0.01, *p < 0.1. The values are presented as mean ± SD (n = 3).
Similarly, ompF expression levels were higher in mutants selected with nanosized drugs (ranging from 1.011 to 1.339 in first mutants, 0.764–1.178 in second mutants, and 0.586–0.895 in third mutants) than in mutants selected with free drugs (0.449–0.627 in first mutants, 0.216–0.508 in second mutants, and 0.162–0.436 in third mutants). Interestingly, ompF expression levels were higher in mutants selected with free single drug (0.390–0.627) versus free combined drugs (0.162–0.449) but lower in NCMm (0.895–1.339) versus those selected with nanosized single drugs (0.586–1.035). However, as with ompC, NCMm expressed significantly higher level of ompF (p-value <0.001) (Fig. 3).
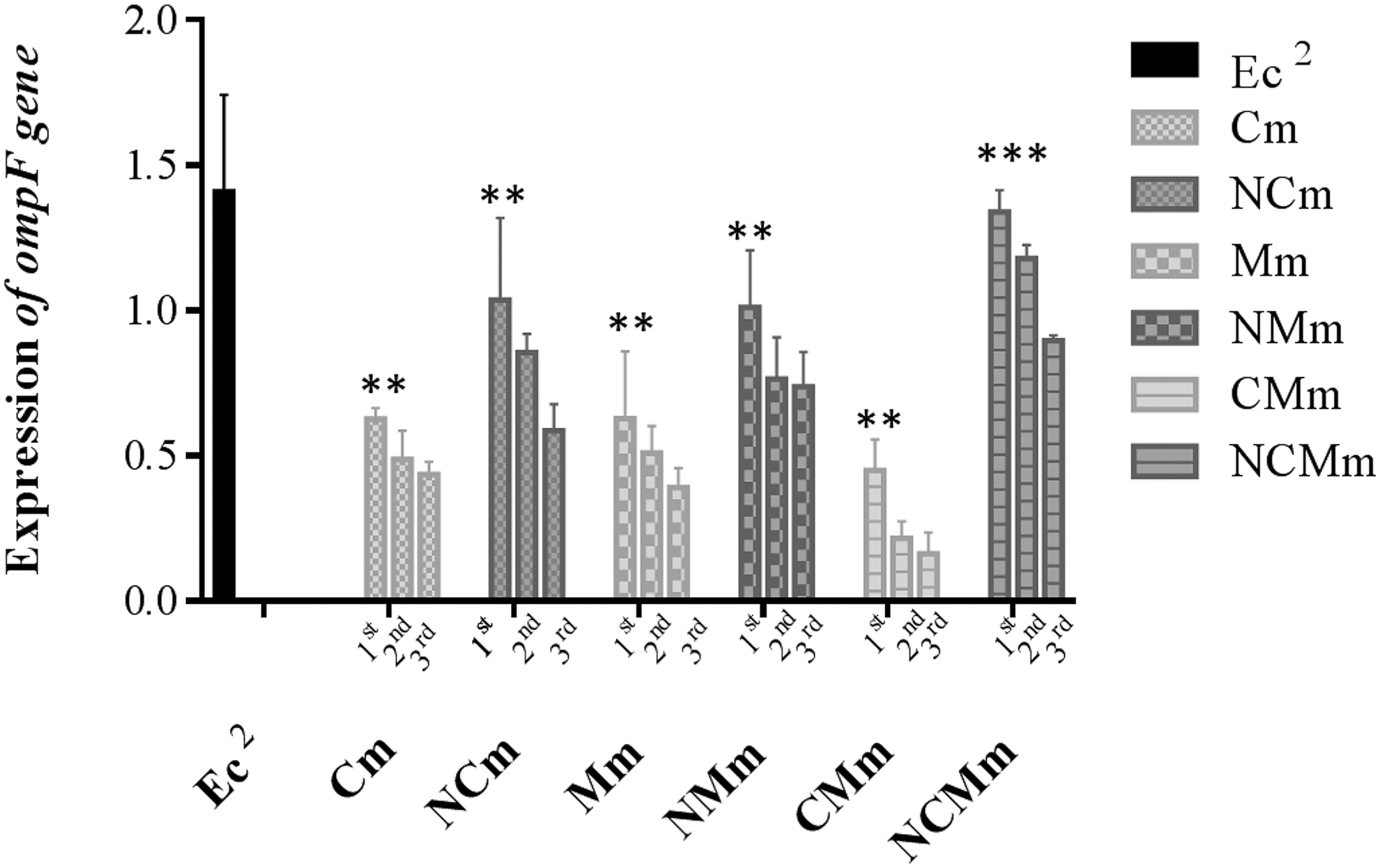
Expression of ompF in parental EC 2 strain and its step mutants. ***p-value <0.001, **p-value <0.01,*p < 0.1. The values are presented as mean ± SD (n = 3).
Discussion
Our previous research demonstrated that nanosized levofloxacin exhibited enhanced antibacterial potency but was not entirely efficient in prevention of resistance development. 13 In the present work, a CS-based nanosystem consisting of nanosized ciprofloxacin in combination with nanosized meropenem was constructed and tested for its potential ability to hinder the development of antibiotic-resistant mutants. Moreover, on the molecular level, the change in acrB efflux pump and porins' expression levels in stepwise selected mutants were tested. To the best of our knowledge, this is the first study to highlight the efficacy of combined nanosized antimicrobials to minimize emergence of treatment-related bacterial resistance through modulation of underlying genetic mechanisms.
Fluoroquinolones and carbapenems are mutagenic in bacteria, and their usage increases the frequency of mutations fueling the development of resistant mutants during antibiotic therapy. This effect is mainly due to stimulation of the SOS response and the upsurge of reactive oxygen species levels, promoting bacterial mutagenesis.18–20 The elevated mutation rate is suggested to play a significant role in the development of antimicrobial resistance by increasing the rate of accumulation of new mutations. 21 In this study, we aimed to explore the effect of nanoparticle encapsulation as well as drug combination on the mutagenicity of both ciprofloxacin and carbapenem.
Mutation frequencies were lower upon treatment with nanosized drugs versus free drugs whether single or in combination in all steps of selection. The small size and positive charge of the nanoparticles increased intracellular bioavailability of the antibiotic and thus inhibited development of mutant subpopulation.8,10 Interestingly, mutation frequencies emerged upon treatment with nanosized combined drugs were low, which could be explained by the counterselection of mutants by the drug combination coupled with the effect of nanoparticle loading. 22
De novo antimicrobial resistance develops gradually through stepwise accumulation of spontaneous mutations that each decreases the susceptibility by small amounts. 23 Therefore, antibiotic protocols enriching mutant subpopulations promote the emergence of resistant mutants. Likewise, agent regimens that inhibit the growth of mutant subpopulations block the development of de novo resistance. 24 To evaluate the antibacterial potency of the nanosized versus free antibiotic formulations, we compared the MICs of ciprofloxacin and meropenem for all step mutants. Ciprofloxacin resistance developed after a single step of selection by either free ciprofloxacin or free meropenem but required two steps of selection by either nanosized ciprofloxacin or nanosized meropenem. Yet, ciprofloxacin resistance appeared in second-step CMm but only in third-step NCMm it expressed only low-level resistance to ciprofloxacin. On the other hand, meropenem resistance emerged in second-step Cm or Mm, and third-step CMm, but, all NCm, NMm, and NCMm expressed susceptibility to meropenem.
Moreover, NCMm displayed a fourfold decrease in MIC values of ciprofloxacin and meropenem compared with CMm. The low MICs and low mutation frequencies exhibited by nanosized drug-selected mutants are expected to impede clonal expansion of resistant mutants when patients are treated with nanosized combined drugs. 25 Besides, dual drug therapy using antibiotics with different targets has an additional advantage through narrowing each other's mutation selection window, thus counter selecting against resistant mutants.24,26 Moreover, polymeric nanocarriers act as cargoes producing a sustained drug release allowing antibiotic concentrations to be kept above the mutation prevention concentration (MPC) for a prolonged period of time. 27 Maintaining antibiotic concentrations above the MPC throughout treatment is essential for limiting emergence of drug resistance.23,28
Previous studies demonstrated that FQ-resistant mutants were associated with MDR phenotype.29,30 The cross-resistance to other antimicrobial classes could be attributed to the mutagenic SOS response that triggers mutation in other drugs' target genes as well as regulators of efflux pumps and porins.16,31 In this study, mutants selected with free drugs—whether single or combined expressed cross-resistance to more antibiotics than in nanosized drug-selected mutants. The less cross-resistance arising with nanosized drugs might be attributed to their small size and sustained release pattern, which significantly restrict evolution of resistance mutations.10,12,16 Interestingly, unlike mutants selected with single nanosized drugs or unloaded combined antibiotics, third-step NCMm retain susceptibility to levofloxacin, denoting stronger antibacterial potency of the nanosized combined formulation.
One of the main mechanisms of the MDR phenotype is the overexpression of efflux pumps and downregulations of membrane porins triggered by mutations in their regulators.31,32 In the current study, the expression levels of acrB efflux pump as well as outer membrane porins ompF and ompC in EC 2 step mutants were tested by qRT-PCR. The expression levels of acrB, ompF, and ompC correlated with the MDR phenotype of step mutants. Mutants selected with nanosized drugs demonstrated lower acrB and higher ompF and ompC expression levels. Furthermore, NCMm exhibited the lowest acrB expression level, and highest ompF and ompC expression levels. Recent studies reported that metallic nanoparticles have an inherent ability to block efflux pumps of bacteria. 9
Moreover, nanoparticles are assumed to bind directly to the pump on the cell membrane, thus preventing the drugs sweeping out of the cell. 33 In this study, we suggest that the increase in the intracellular bioavailability of nanosized drugs hindered the selection of mutant subpopulations, including those with mutations in regulators, thus expressing close to normal pump and porin levels. This suggestion is supported by the low mutation frequency arising with nanosized drugs, with additional counter selection of populations with regulators' mutation by the dual drug therapy.
Conclusion
In the current work, CS–pluronic nanoparticles were loaded with ciprofloxacin and meropenem and the combination of nanosized antibiotics was evaluated for its antibacterial potency. The nanosystem displayed high activity in restricting the evolution of resistant mutants owing to enhanced bioavailability by nanoparticle encapsulation coupled with the complementary bactericidal effect of ciprofloxacin and meropenem. Accordingly, research studies should be implemented to evaluate the in vitro antimicrobial activity of these combined antibiotic nanosystems. Furthermore, it is important to present a general policy against MDR infections based on the concomitant use of nanosized antibiotics with different but complementary activity.
Footnotes
Authors' Contributions
S.H.: performed investigation, data analysis, and writing original draft. S.A.A.: performed experimental protocol conceptualization, project administration, supervision, accomplished the resources, validation, and editing the article. M.E.: provided supervision of nanoparticle procedures, resources, and supervision. R.M.A.E.: performed validation and editing. R.A.I.: provided supervision and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported financially by the Science and Technology Development Fund (STDF), Egypt, grant no (25913).