
Abstract
Elizabethkingia meningoseptica is an uncommonly encountered multidrug-resistant gram-negative bacterium that causes infections primarily among vulnerable hosts. A true opportunistic pathogen, its ability to cause severe sepsis and complicated infection in selected patients has been noted. Very limited preclinical and clinical data exist with regard to suitable therapeutic options. In this study, we present the case of prolonged bloodstream and central nervous system infection due to E. meningoseptica treated with dose-optimized combination antibiotic therapy, with evidence of microbiological (including development of adaptive resistance mechanisms) and clinical failure.
Introduction
Elizabethkingia species are nonfermenting gram-negative bacteria assigned to the family Weeksellaceae, order Flavobacteriales. 1 As opportunistic pathogens, Elizabethkingia spp. have caused a broad range of clinical diseases, with the most common being bloodstream infection; pneumonia, meningitis, peritonitis, and urinary tract infection have also been documented.2,3 Risk factors for infection primarily relate to immunosuppression and underlying comorbidities. 4 Elizabethkingia spp. intrinsically harbor many antimicrobial resistance genes and display in vitro resistance to a broad range of antimicrobials, including penicillins, β-lactams and β-lactamase inhibitors, monobactams, cephalosporins, carbapenems, aminoglycosides, and polymyxins. 5 Little is known about which treatment strategy is best in the management of infections due to this formidable pathogen.
Case
A 72-year-old male presented to a regional hospital following 2 weeks of left ear pain. He had been applying topical steroid therapy and an ear wax dissolving solution without any clinical improvement. He also described developing an acute headache, fever, vomiting, and malaise. He had a background of lymphoplasmacytic lymphoma treated with rituximab and bendamustine 1 year prior and was currently in remission. His medical history also included type 2 diabetes mellitus, hypertension, and gastroesophageal reflux disease. In the emergency department, he was noted to be confused and agitated. On examination, his vital signs were blood pressure 135/90 mmHg, heart rate 95 bpm, respiratory rate 20, and temperature 37.8°C. He was disoriented with a Glasgow Coma Scale (GCS) of 14; there was no focal neurology present. He was noted to have neck stiffness and marked tenderness to palpation of his left ear and mastoid process.
A full blood count demonstrated a raised white blood cell count of 15 × 109/L (neutrophils 13.8 × 109/L). Cerebrospinal fluid (CSF) analysis was performed, which demonstrated a white blood cell count of 3,500 × 106/L, protein 4,000 mg/L, and glucose 4.6 mmol/L; gram-negative bacilli were seen on the Gram stain. Computed tomography brain imaging demonstrated evidence of a subacute to chronic left-sided mastoiditis, with marked bony destruction of the petrous apex. Two sets of blood cultures were taken from separate venepuncture sites, and he was commenced in intravenous (IV) ceftriaxone 2 g twice daily. He had persistent evidence of sepsis, as evidenced by tachycardia and fever, and experienced worsening of his GCS, prompting intubation and admission to the intensive care unit.
At this point, his antimicrobial therapy was changed to IV meropenem 2 g every 8 hours. At 22.3 hours, the aerobic blood culture bottle flagged positive (BACT/ALERT® Virtuo®) and nonmotile gram-negative bacilli were seen on microscopy. Mucoid colonies were observed on 5% horse blood agar, chocolate agar and MacConkey agar, which were catalase, oxidase, and indole positive. MALDI-TOF MS (VITEK® MS v3.2; bioMe´rieux) identified the organism as Elizabethkingia meningoseptica; CSF culture yielded growth of the same organism. After 48 hours of being admitted to the regional hospital, he was then transferred to a tertiary referral hospital due to his clinical condition.
Immediately before hospital transfer, an infectious diseases specialist was contacted and the patient's antibiotic regimen was changed to IV ciprofloxacin 400 mg every 8 hours and IV vancomycin 1.25 g every 12 hours. He weighed ∼75 kg. Minimum inhibitory concentration (MIC) values on the index isolate were determined by the gradient diffusion strip method (Etest®; bioMe´rieux) and were 0.5, 0.25, 0.5, 2, and 4 mg/L (Fig. 1) for ciprofloxacin, trimethoprim–sulfamethoxazole, rifampicin, doxycycline and vancomycin, respectively. Disc diffusion was performed for piperacillin–tazobactam and cefiderocol, which yielded zone diameters of 19 and 6 mm, respectively. Magnetic resonance imaging of the brain revealed left-sided mastoid osteomyelitis with skull base destruction and intracranial extension of infection, with evidence of diffuse leptomeningitis, ventriculitis, and early hydrocephalus.
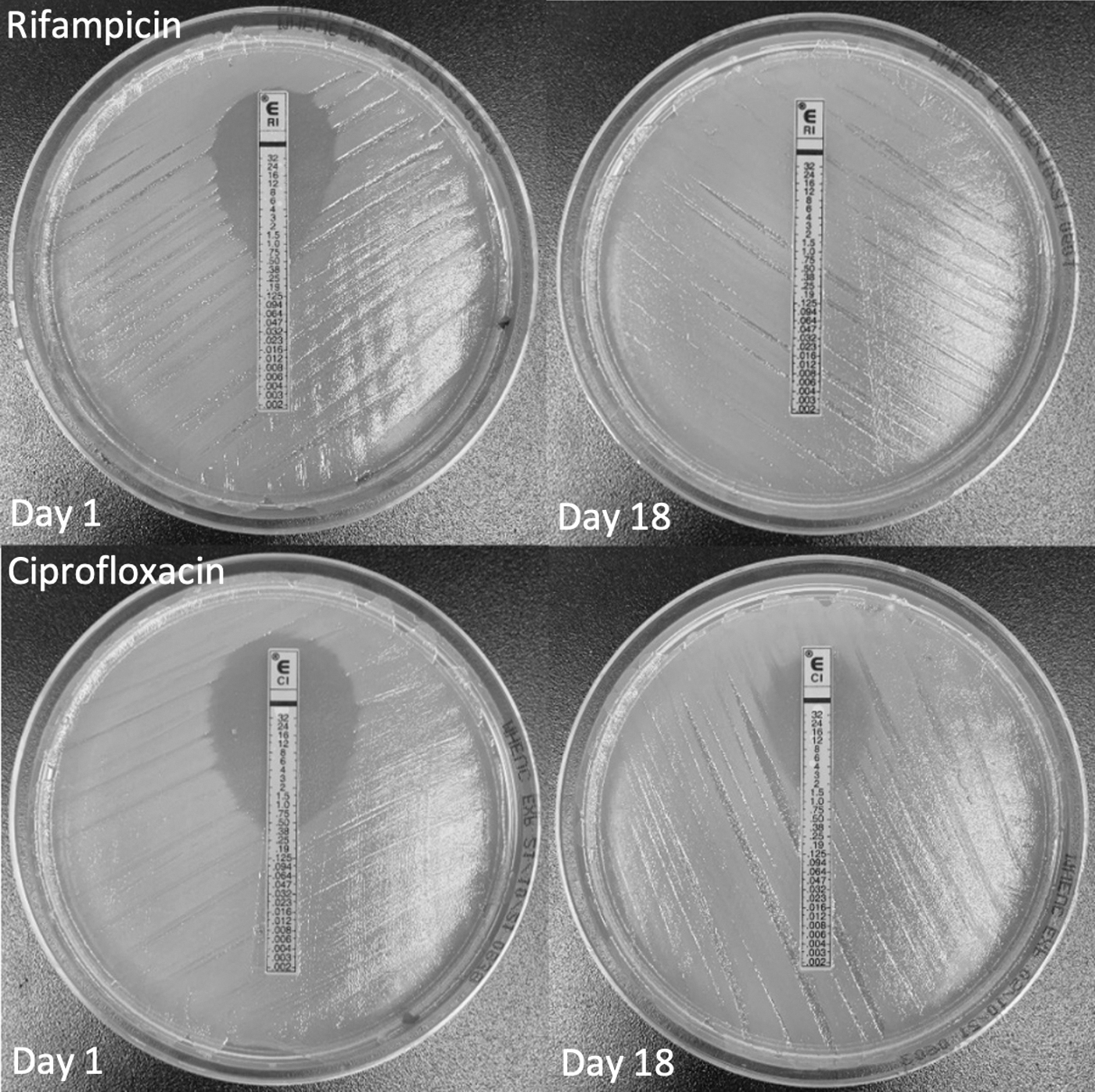
Rifampicin and ciprofloxacin MIC values determined by the gradient diffusion method (Etest®; bioMe´rieux) on day 1 and day 18 Elizabethkingia meningoseptica bloodstream isolates. MIC, minimum inhibitory concentration.
Vancomycin was ceased on day 3 of presentation and a left cortical mastoidectomy and tympanostomy tube insertion were performed. He continued to have fever and E. meningoseptica was growing on repeated blood and surveillance endotracheal aspirate cultures. On day 6, IV trimethoprim–sulfamethoxazole 320 mg (total dose) every 8 hours was added to ciprofloxacin. He then developed deranged liver function tests attributed to the addition of the new antimicrobial and this was ceased on day 10; IV rifampicin 300 mg every 12 hours was commenced. Peak and trough plasma free ciprofloxacin levels were 3.44 and 1.98 mg/L (expected range: peak 0.7–6.6 mg/L, trough 0.05–2.16 mg/L). 6 This regimen failed to sterilize his blood cultures, with the blood culture isolate on day 14 demonstrating high-level rifampicin resistance (MIC >32 mg/L).
Rifampicin was ceased, the IV ciprofloxacin dose was increased to 600 mg every 8 hours, and IV piperacillin–tazobactam 27 g over 24 hours as a continuous infusion was commenced. Peak and trough plasmafree ciprofloxacin levels were now 5.63 and 2.59 mg/L. With this piperacillin–tazobactam dosing strategy, the free plasma levels of piperacillin in plasma and CSF were 103.6 and 0.2 mg/L, and of tazobactam were 14.3 and 5 mg/L. His clinical condition failed to improve, and he had ongoing bacteremia. An extraventricular drain was inserted on day 17 with intraventricular vancomycin 10 mg delivered into the central nervous system (CNS) over 24 hours.
Despite this, E. meningoseptica was still able to be cultured from the blood, CSF, and endotracheal aspirate specimens up to day 19. MIC testing on the day 18 blood culture isolate demonstrated MIC values for ciprofloxacin, rifampicin, trimethoprim–sulfamethoxazole, and vancomycin of 4, >32, 4, and 4 mg/L, respectively. Active medical care with curative intent was discontinued and he subsequently died on day 22 (Fig. 2).
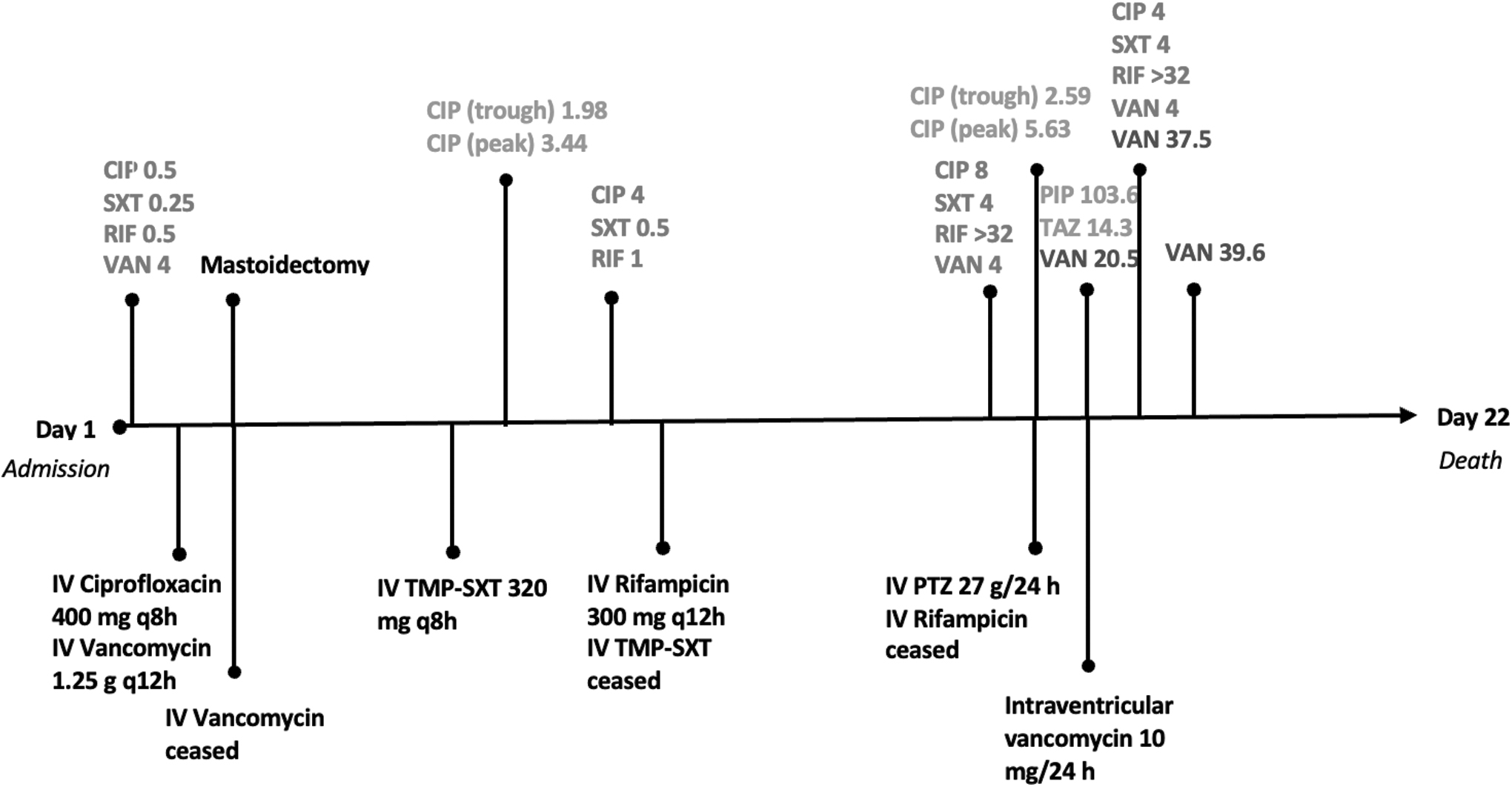
Time line of events. MIC (mg/L) in blood (red); antibiotic drug level (mg/L) in blood (green); antibiotic drug level (CSF, mg/L) in CSF (purple). CSF, cerebrospinal fluid.
Day 1 and day 18 blood culture isolates underwent comparative genomic analysis. Whole-genome sequencing (WGS) (Illumina MiniSeq; Illumina) was performed on both isolates. Using Kraken and RefSeq database, both samples were screened for contamination and taxonomic labels were assigned. Both bacterial isolates were identified as E. meningoseptica by WGS. In silico resistance gene profiles were determined by screening the genome assemblies for each isolate against the NCBI resistance gene database using ABRicate. Both isolates had blaB-3 and blaGOB-16 present; there were no van gene mutations present. The day 18 isolate demonstrated both an R493K mutation in the rpoB gene and a frameshift mutation in tetR family transcriptional regulator. This transcriptional regulator is located immediately upstream from the acrAB efflux pump, which has been associated with ciprofloxacin resistance in Klebsiella pneumoniae. 7
No mutations were detected in GyrA, GyrB, ParC, or ParE genes in the day 18 isolate. In addition, plasmid-mediated qnr genes were not detected.
Discussion
Elizabethkingia species have proven to be formidable multidrug-resistant pathogens. Indeed, genomic studies have demonstrated a host of commonly encountered resistance genes including blaCME (class A extended-spectrum beta-lactamase), blaB and blaGOB (class B carbapenemase), AmpG (class C beta-lactamase), tet(X) (tetracyclines), aadS (aminoglycosides), and van (glycopeptides). 5 In vitro susceptibility results reveal that most isolates are susceptible to fluoroquinolones, rifampicin, tetracyclines, and trimethoprim–sulfamethoxazole.5,8 In vitro results in these studies for fluoroquinolones, tetracyclines, and trimethoprim–sulfamethoxazole use Clinical & Laboratory Standards Institute breakpoints for non-Enterobacteriaceae as there are no agreed upon breakpoints for Elizabethkingia species. Vancomycin susceptibility appears more varied depending on the geography. 5 In our case, a significant rise in MIC occurred during therapy for ciprofloxacin, trimethoprim–sulfamethoxazole, and rifampicin (Table 1).
Minimum Inhibitory Concentration Values and Antimicrobial Drug Levels (mg/L)
CSF, cerebrospinal fluid; MIC, minimum inhibitory concentration.
The most common mechanism of fluoroquinolone resistance in Elizabethkingia species appears to occur in the quinolone resistance determining region of the gyrA gene. 9 The AcrAB efflux pump expression also plays a role in mediating fluoroquinolone resistance. 9 Given the absence of GyrA gene mutations in our isolates, and the presence of a frameshift mutation in a transcriptional regulator of the AcrAB efflux pump, this provides a possible explanation for the in vivo development of ciprofloxacin resistance. No resistance mechanism for trimethoprim–sulfamethoxazole was identified. Mutations in dfrA12, sul I, sul II, and folP genes have been described as possible mechanisms. 10
WGS in real time provides an opportunity to rapidly identify antimicrobial resistance genes and may provide insight into emerging adaptive resistance mechanisms. This offers another testing modality in the arsenal used to inform treatment of complicated multidrug-resistant gram-negative infections.
Very little treatment and outcome data exist for this uncommon pathogen. Treatment strategies utilized in documented outbreaks, case reports, and series are varied.11–13 Although the most effective and reliable antimicrobial therapy is still unknown, various combinations of minocycline, tigecycline, ciprofloxacin, levofloxacin, rifampicin, trimethoprim–sulfamethoxazole, and piperacillin–tazobactam have been used.11–13 Some have advocated for the use of vancomycin as previous studies have shown activity in vitro and clinical resolution with its use. 14 However, vancomycin MIC may be unreliable, and many studies have revealed a high percentage of isolates demonstrating resistance. 5
An observational study, which included 210 hospitalized patients with bacteremia or pneumonia due to Elizabethkingia species, identified rifampicin MIC as a predictor of a 28-day mortality rate. 15 In the absence of established clinical breakpoints for the Elizabethkingia species, and the potential for this pathogen to rapidly develop resistance in vivo, we believe that high-dose combination therapy with antimicrobials demonstrating in vitro activity is warranted.
Therapeutic drug monitoring and antimicrobial dose optimization in critically unwell patients due to gram-negative infections may provide benefit.16,17 The different classes of antibiotics used have different pharmacodynamic indices of efficacy. Therefore, in the setting of combination therapy, it is important to take an individual approach to optimizing their dosing. This was pertinent in our case not only to overcome intrinsic and adaptive resistance mechanisms of E. meningoseptica, but also to attain adequate drug levels at privileged sites of infection such as the CNS. It is possible that subtherapeutic antibiotic concentrations at difficult-to-penetrate sites drove adaptive resistance mechanisms seen in our case. Source control is paramount in such infections, and this was unable to be achieved in our case due to the nature of the infection.
We optimized drug exposure in numerous ways: increased the dose of ciprofloxacin to maximize area under the curve/MIC, high-dose piperacillin–tazobactam administered as a continuous infusion to maximize
This case highlights several gaps in knowledge that we currently suffer when answering the question on the best therapeutic strategy for uncommon gram-negative nonfermenters. These include establishing clinical breakpoints, drivers of acquired resistance mechanisms, and optimal therapeutic strategies. It also recognizes emerging tools that are making their way into clinical practice that may prove to be invaluable in improving patient care.
Footnotes
Authors' Contributions
A.G.S.: Conceptualization, writing—original draft, formal analysis, review, and editing. J.A.R.: Writing—review and editing and formal analysis. B.M.F.: Formal analysis (lead). H.B.: Formal analysis. T.J.K.: Formal analysis, review, and editing. H.W.: Writing—review. P.N.A.H.: Writing—review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
J.A.R. would like to acknowledge funding from the Australian National Health and Medical Research Council for a Centre of Research Excellence (APP2007007) and an Investigator Grant (APP2009736) as well as an Advancing Queensland Clinical Fellowship. P.N.A.H. has received funding from Pfizer, Merck Sharpe & Dohme (MSD), and Shionogi.