
Abstract
Purpose:
Infections caused by carbapenem-resistant Klebsiella pneumoniae (CR-KP) are an important public health problem. This study aimed to evaluate the clinical characteristics of patients with CR-KP.
Methods:
A retrospective cohort study was conducted of all patients with CR-KP infection. A total of 615 patients with CR-KP infection were identified and 135 patients who did not meet the eligibility criteria were excluded. Clinical characteristics, antimicrobial regimens, and patient outcomes were analyzed.
Results:
The overall mortality rate of CR-KP infections was 37.3% and the mortality rate in patients with bloodstream infections was 66.2%. Survival analysis revealed that there were statistically significant differences between patients with bloodstream infections and those with pulmonary and drainage fluid infections. Logistics regression analysis showed that hemopathy, age >60 years, solid tumors, diabetes, septic shock, acute kidney injury, and stroke were independent predictors of 30-day mortality rate. The chi-square test showed that treatment with a combination of carbapenems, tigecycline, and polymyxin B was superior to treatment with carbapenems with polymyxin B, without tigecycline.
Conclusions:
CR-KP infections, especially bloodstream infections, have a high mortality rate. The outcome is strongly dependent on patients' clinical conditions. Antimicrobial regimens combining carbapenems, tigecycline, and polymyxin B might be a better choice.
Introduction
Carbapenem-resistant Klebsiella pneumoniae (CR-KP) infection is a health threat worldwide.1–3 Infections caused by CR-KP are associated with a high mortality rate, ranging from 18% to 48% overall, and from 51% to72% in bloodstream infections, depending on the type of antimicrobial therapy administered and patient characteristics.4–7
The first CR-KP strain was identified in 1993, and since then, CR-KP strains have become endemic in many countries. 8 The 2016 Annual Report of the European Antibiotic Surveillance Network reported a mean prevalence of carbapenems resistance of 6.1%. In 2018, the prevalence of K. pneumoniae resistance in China was 15.4% to imipenem and 17.9% to meropenem. 9
Although several studies have shown the effectiveness of combination regimens for reducing mortality, choosing an effective treatment regimen remains a challenge for clinicians.10–13
This study evaluated the clinical characteristics of CR-KP infections in a tertiary hospital in China.
Methods
Patients
All patients with CR-KP infections at the First Affiliated Hospital of Zhengzhou University between January 2018 and December 2019 were identified from the hospital database. The study was approved by the human ethics committee of the First Affiliated Hospital of Zhengzhou University. The patients included in the database were followed by reviewing their medical records and contacting them directly. The requirement for informed consent was waived owing to the retrospective study design. Ethics approval number: 2020-KY-1468.
All patients included in this study were required to meet the following inclusion criteria: (1) age between 18 and 80 years and (2) diagnosis of CR-KP infection base on at least one positive culture. All sputum specimens were bronchoalveolar lavage fluid. Patients who died or were discharged within 48 hours after the initiation of adjusted therapy regimens and those with incomplete or missing data were excluded.
Sample collection
Patient variables include age, gender, presence of acute or chronic comorbidities, Acute Physiology and Chronic Health Evaluation (APACHE II) and Sequential Organ Failure Assessment (SOFA) scores, absolute lymphocyte count (LYM, within 2 days of culture collection), previous surgery (≤30 days before the positive culture), any invasive procedures (≤72 hours before the positive culture), steroid or immunosuppressive therapy (≤30 days before the positive culture), previous antimicrobial therapy regimens (≤30 days before the positive culture), survival days, and adjusted therapy regimens after the positive culture. Rectal swabs were collected from some patients and screened for the presence of carbapenem-resistant enteric bacteria.
The primary outcome was death within 30 days of the first positive culture. Survivor and nonsurvivor subgroups were compared to identify the predictors of mortality.
Antimicrobial therapies
Once the culture and susceptibility results were known, the attending physician determined the appropriateness of the initial antimicrobial therapy. Antimicrobial therapy administered within 5 days after the onset of infection was defined as empirical therapy. Appropriate definitive antibiotic therapy was defined as that matching the in vitro susceptibility results according to the Clinical and Laboratory Standards Institute criteria.
Definitions
Septic shock was defined as sepsis with persistent hypotension, requiring vasopressors to maintain a mean arterial pressure ≥65 mmHg and serum lactate levels >2 mmol/L, despite adequate fluid resuscitation. 14
Acute kidney injury was defined as follows: (1) increase in serum creatinine by ≥0.3 mg/dL within 48 hours, (2) increase in serum creatinine by ≥1.5 times baseline, and (3) urine volume <0.5 mL/kg per hour for ≥6 hours. 15
Samples were routinely collected for microbial culture patients had fever and there was evidence or clinical suspicion of infection. Bloodstream infection was defined as hospital acquired if the index blood culture was collected >48 hours after hospital admission.
Statistical analysis
Statistical analysis was performed using SPSS version 22.0 (IBM Corp., Armonk, NY). Categorical variables reported as frequencies were compared using the χ 2 test or Fisher's exact test. Multivariable logistic regression analysis was used to identify independent risk factors for mortality. Kaplan–Meier curves were plotted to compare the 30-day survival rate in patients with blood stream infection, bronchoalveolar lavage fluid infection, and drainage infection. Continuous variables were evaluated using multiple linear regression analysis. Receiver-operating characteristic (ROC) curves were constructed for the LYM, and the APACHE II and SOFA scores. p-Value <0.05 was considered statistically significant.
Results
Baseline characteristics
We collected clinical data from 615 patients diagnosed with CR-KP infections between January 2018 and December 2019. A total of 135 patients who did not meet the eligibility criteria were excluded, and the remaining 480 patients were enrolled in the study. The baseline characteristics of the study cohort are given in Table 1.
Demographic and Clinical Characteristics of the Study Cohort According to the 30-Day Outcome
BALF, bronchoalveolar lavage fluid; CNS, central nervous system; COPD, chronic obstructive pulmonary disease; CRRT, continuous renal replacement therapy; ICU, intensive care unit.
The 30-day mortality rate in patients with CR-KP was 37.3%. The majority of patients (289, 60.2%) were male, and 191 (39.8%) were female. Of the 480 patients, 379 patients (78.9%) had pulmonary infection and 68 patients (14.2%) had bloodstream infection. Hypertension, coronary heart disease, and neurological diseases were the most common underlying diseases (47.7%, 35.2%, and 21.9%, respectively). Stroke (188, 39.2%) was the most common acute complication, followed by acute kidney injury (117, 24.4%) and septic shock (108, 22.5%). Septic shock was significantly more frequent among nonsurvivors than among survivors (46.3% vs. 8.3%, p < 0.001).
Most patients (430, 89.6%) underwent intubation or tracheotomy, and 387 patients (80.6%) underwent central venous catheter insertion. A proportion of patients received steroid therapy (93, 19.4%) or continuous renal replacement therapy (58, 12.1%). Rectal swabs were collected from 116 patients and screened for the presence of carbapenem-resistant enteric bacteria, of whom 35 (30.2%) were positive.
Antibiotic therapy
The empirical and definitive antibiotic therapies administered to patients with CR-KP in the survivor and nonsurvivor groups are summarized in Table 2. The most frequently used antibiotic regimens for both empirical and definitive therapies were carbapenems in both groups. The survival according to the antibiotic regimen is given in Table 3.
Antibiotic Therapy According to the 30-Day Outcome
Combination Antibiotic Regimens According to the 30-Day Outcome
The chi-square test showed that both regimen A (ceftazidime avibactam and tigecycline, χ 2 = 4.52, p = 0.033) and regimen B (carbapenems, tigecycline, and polymyxin B, χ 2 = 3.96, p = 0.04) were associated with significantly better survival than regimen C (carbapenems and polymyxin B alone) (Fig. 1). However, there was no statistically significant difference in survival among patients treated with antibiotic regimens D (carbapenems and tigecycline), C (carbapenems and polymyxin B), and E (carbapenems, tigecycline, and fosfomycin). Polymyxin B and tigecycline appeared to have a synergistic effect and were more effective than a regimen of carbapenems plus polymyxin B alone. Ceftazidime avibactam-based antimicrobial regimens had no advantage over other antibiotic regimens.

In addition, we investigated the effectiveness of tigecycline in combination with other antibiotic regimens for the treatment of CR-KP. The different antibiotic regimens used are listed in Table 4.
Outcomes in Patients Who Received Tigecycline in Combination with Other Antibiotic Regimens
Chi-square test showed that there were no statistically significant differences among the different antibiotic regimens (χ 2 = 5.432, p = 0.246). Considering the price of antibiotic regimens, we recommend the use of biapenem combined with tigecycline as a therapeutic regimen.
Prognostic factors
In the multivariate logistic regression analysis, hemopathy, age (>60 years), solid tumors, diabetes, septic shock, acute kidney injury, and stroke were independent predictors associated with the 30-day mortality rate (Table 5).
Multivariable Logistic Regression Analysis of Risk Factors for Mortality
CI, confidence interval; OR, odds ratio.
Correlation analysis and ROC curves
Multivariate linear regression was performed to assess the correlation between APACHE II and SOFA scores, lymphocyte absolute value, and survival time. Survival time was negatively correlated with APACHE II and SOFA scores, and positively correlated with lymphocyte absolute value (Fig. 2). The areas under the ROC curves for the APACHE II score, SOFA score, and lymphocyte absolute value were 0.825, 0.876, and 0.797, respectively, with cutoff values of 17, 6, and 0.775, respectively.
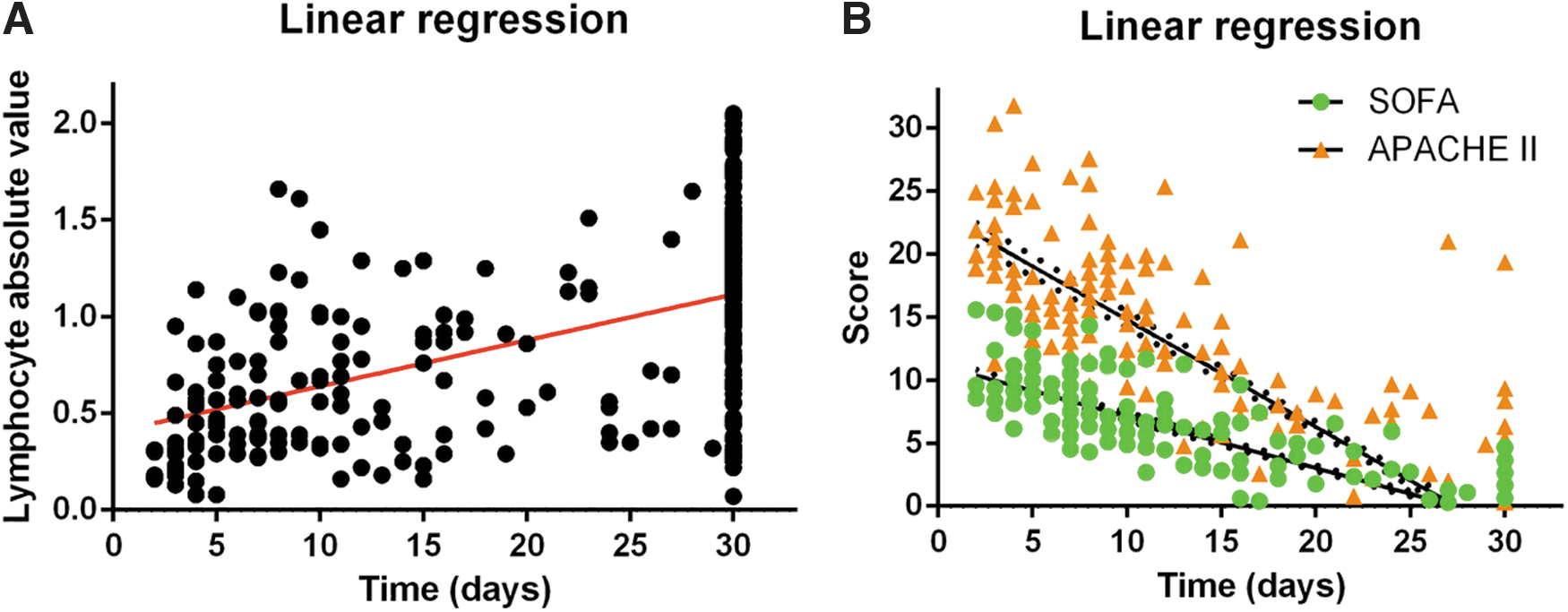
Linear regression analyses of the survival time in relation to the absolute lymphocyte count, SOFA and APACHE II scores.
Survival analysis
Survival analysis showed that patients with bloodstream infections had significantly worse survival than patients with pulmonary or drainage fluid infections (Fig. 3).
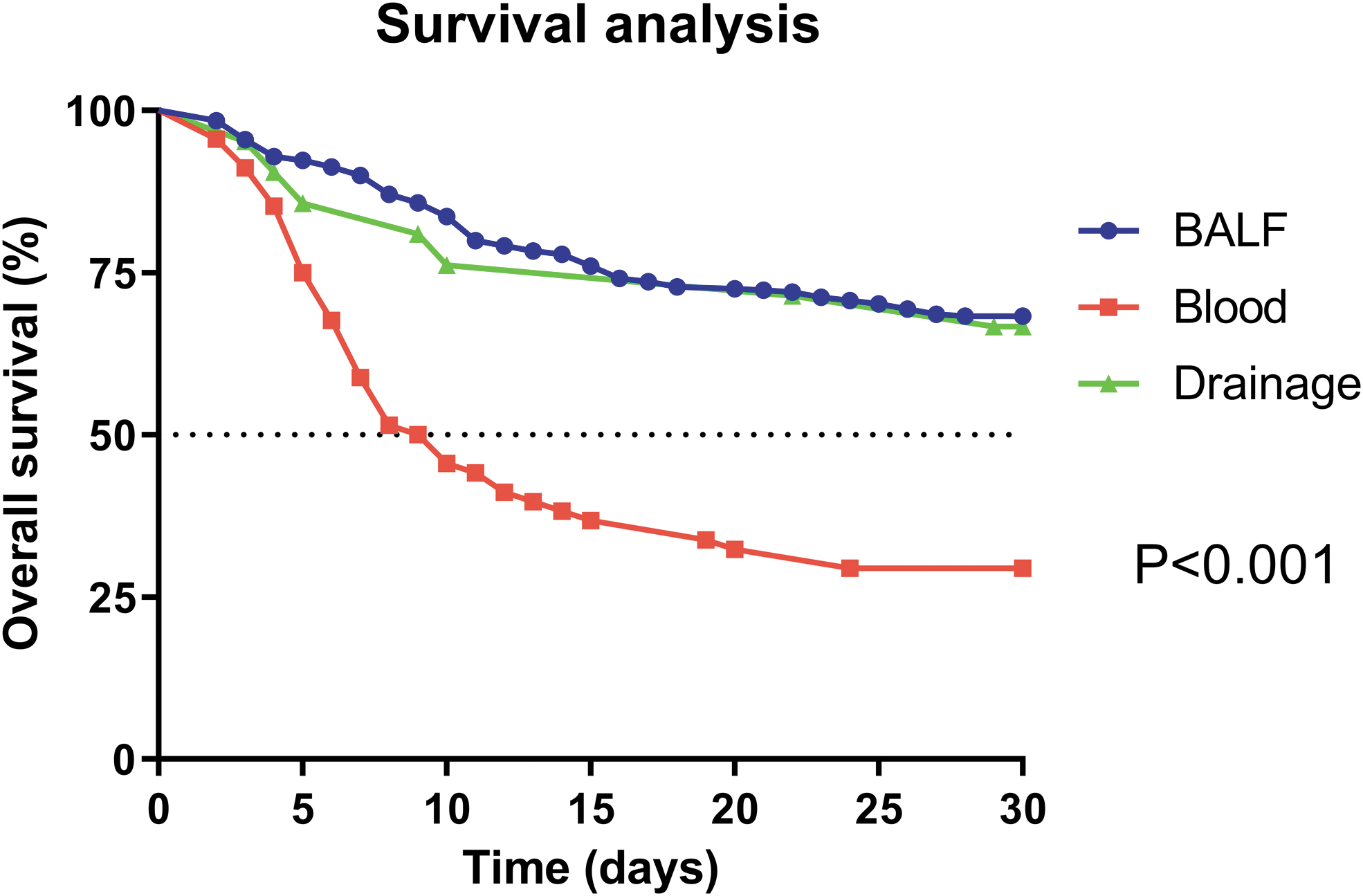
Kaplan–Meier survival curves of survival in relation to the site of infection. BALF, bronchoalveolar lavage fluid.
Discussion
In this study we evaluated 30-day mortality rate in patients with CR-KP infection. The total mortality rate of patients with CR-KP infection was 37.3% and was higher in patients with bloodstream infection (66.2%) as in previous studies.2,3,16 Mortality was associated with patient characteristics, antibiotic therapeutic regimens, and the immune status of the patients.
The relatively high mortality rate compared with previous studies might be attributable to several factors. First, our hospital is a tertiary referral hospital, and many patients had severe disease on admission to our hospital. The state of the patients was directly related to mortality, as shown in previous studies.4,5 Second, administering appropriate empirical antibiotic therapy and definitive therapy are important predictors of patients' outcome.6,17 Therefore, it is very important to administer appropriate antibiotic regimen before patients are admitted to the intensive care unit.
Clinical departments, especially surgery departments, should pay more attention to the rational use of antibiotic regimens. Finally, it is important to detect pathogens and adjust the therapeutic regimen to treat CR-KP infection. 18 However, the positive rate of bacterial culture was low. The positive rate of rectal swabs for the carbapenem-resistant enteric bacteria was only 30.2% in our study. In recent years, next-generation sequencing has emerged as a tool to help diagnose infections with organisms that are difficult to culture. Its role in diagnosing CR-KP infections warrants further study. 19
Independent risk factors associated with mortality included hemopathy, age >60 years, solid tumors, diabetes, septic shock, acute kidney injury, and stroke. Correlation analysis showed that survival time was positively correlated with LYM. Lymphocytes are involved in innate and adaptive immunity, and a low is directly associated with poorer prognosis.20–22
We investigated the effectiveness of tigecycline in combination with different antibiotic regimens (meropenem, imipenem, biapenem, ceftazidime avibactam, and third- or fourth-generation ephalosporins) in the treatment of CR-KP, and the differences were not statistically significant. Considering the price of antibiotic regimens, we recommend the use of biapenem combined with tigecycline as a therapeutic regimen. The combination of tigecycline with meropenem or ceftazidime avibactam was associated with a higher survival rate. As there were many neurosurgical patients, meropenem was used frequently.
Antibiotic regimens A (ceftazidime avibactam and tigecycline) and B (carbapenems, tigecycline, and polymyxin B) were superior to antibiotic regimen C (carbapenems and polymyxin B). This may be because polymyxin B is a narrow-spectrum antibiotic and some patients have multiple drug-resistant bacterial infections. In addition, polymyxin B and tigecycline may have synergistic effect in treating CR-KP infection. Finally, ceftazidime avibactam-based antimicrobial regimens had no advantage over other therapeutic regimens; however, the sample size was small, and the effectiveness of ceftazidime avibactam-based antimicrobial regimens warrants further study.
Our study has some limitations. The sample size was too small to allow detection of subtle differences in the treatment outcome. As our data were obtained from a single center, a multicenter prospective cohort study with a more extensive collection of data on potential confounders is required.
Conclusion
Our study confirmed a high mortality rate in patients hospitalized with CR-KP infections, especially for bloodstream infections. The outcome was strongly associated with patients' clinical conditions. A combination of carbapenems, tigecycline, and polymyxin B might be a good choice for treating patients with CR-KP infections. Ceftazidime avibactam-based antimicrobial regimens had no advantage over other therapeutic regimens. Further research is required to confirm this finding, especially in light of the introduction of new antimicrobial agents.
Footnotes
Authors' Contributions
Z.C. contributed to methodology, software, collecting data, and writing the original draft. L.W. was involved in investigation, methodology, data curation, and validation. M.F. took care of review and editing.
Availability of Data and Materials
Data will be made available upon reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.