
Abstract
In this study, we aimed to characterize drug-resistant strains by whole-genome sequencing (WGS), to describe the spreading lineages and the history of transmission. Drug susceptibility testing was performed by 96-well broth microdilution plates. The genomic DNA was extracted and purified; libraries were prepared and run on the Illumina NextSeq500 System. Among 82 isolates, 21 tuberculosis (TB) isolates (25.6%) were drug resistant, including 10 MDR and 4 pre-extensively drug-resistant (XDR)-TB. The mutation Ser315Thr in the katG gene was confirmed in 15 isolates. In rpoB, Ser450Leu and His445Asp mutations were the most common. Asp94Asn and Ala90Val mutations were reported in gyrA. The LAM family, the most TB drug resistant, was widely predominant in the north and the T sublineage in the south of the country. This study provides the first insight on TB drug resistance using WGS in Algeria and clearly describes the first pre-XDR-TB cases and lineage distribution across the country.
Introduction
Tuberculosis (TB), a highly transmissible and hardly treatable infectious disease, is a major health concern at the global scale. Despite efforts by the international community to reduce its incidence, the World Health Organization (WHO) annual reports and estimates remain of concern. The COVID-19 pandemic has reversed years of progress in providing essential TB services and reducing TB disease burden. Global TB targets are mostly off-track, the most obvious impact is a large global drop in the number of newly diagnosed TB patients and the increase in deaths, reaching 1.3 million among HIV-negative people, during 2020. 1
Geographically, in 2020, most TB cases were in the WHO regions of Southeast Asia (43%), Africa (25%) and the Western Pacific (18%). Furthermore, the African region recorded the highest case fatality rate of
The WHO African region is also facing a serious public health problem, with the emergence of drug-resistant TB, and lack of means for drug susceptibility testing (DST) and survey. In 2020, only 50% of confirmed TB isolates were tested for rifampicin resistance. 1 Moreover, Angola, Congo, and Liberia have never conducted a drug resistance survey, and most high-burden countries do not have the capacity to establish continuous surveillance systems. 2 The current Covid-19 pandemic can worsen the situation and the consequences of treatment interruption will be dramatic in the subsequent years.
To estimate drug-resistant TB, conventional DST methods do not allow a detailed study of a wide range of molecules and resistance levels. For this purpose, novel broth microdilution methods have been proposed recently, for example, the UKMYC-5 and UKMYC-6 96-well microtiter plates, variants of the MYCOTB plate from Thermo Fisher, designed by the Comprehensive Resistance Prediction for
The recent few works in Algeria revealed a low TB drug resistance rate 1 and high diversity of MTB lineages. However, to our knowledge, only classical methods were used, based on proportion methods, spoligotyping, and PCR, with lower accuracy with respect to WGS. For example, in the study of Bouziane et al., 5 only 10 MDR and 1 isoniazid-resistant isolates were characterized by PCR-Sanger sequencing. The WGS and UKMYC5 methods used here reach the highest resolution to characterize MTB strains, as in previous results.3,4 This study exploits the WGS approach to characterize TB drug resistance patterns, to highlight the main MTB spreading lineages in Algeria, and to reveal the history of transmission between populations from different regions.
Materials and Methods
Study design
This study was conducted between June 2017 and December 2019, at the Tuberculosis and Respiratory Disease Control Unit (TRDCU) of Bejaia city, the laboratory of Microbial Ecology of Bejaia University, in collaboration with the TB Supranational Reference Laboratory, IRCCS San Raffaele Scientific Institute, Milan, Italy. For these purposes, we asked the 48 TRDCUs representing the 48 provinces to send their 2 to 3 recent MTB strains. An initial collection of 143 strains was obtained from 40 TRDCUs. After culture, purification, exclusion of repetitive cases and extra pulmonary cases, 100 nonrepetitive samples (1 sample/patient) were randomly selected for the study, from pulmonary TB cases. Nevertheless, only 82 isolates achieved final results. All demographic and socioeconomic data of patients, including age, sex, geographic location, previous treatment status, and isolation date, were collected in total respect of deontology rules, medical secret, and patients' privacy.
Strain identification
M. tuberculosis (82) isolates were selected by direct examination, according to Ziehl-Neelsen (Z-N) staining and bacterial culture on Lowenstein–Jensen (L-J) medium. The identification of the isolates was confirmed by Bactec MGIT 960 (Becton, Dickinson, MD), Z-N staining, and WGS-based species identification.
Drug susceptibility testing
M. tuberculosis isolates (82) were tested for DST first, by the proportion method on L-J medium containing the following drugs: isoniazid (INH, 0.2 μg/mL), rifampicin (RIF, 40 μg/mL), ethambutol (EMB, 2 μg/mL), streptomycin (STR, 4 μg/mL), ofloxacin (OFL, 2 μg/mL), and kanamycin (KAN, 20 μg/mL). All tubes were incubated for up to 72 days, at 37°C. The critical proportion necessary to define an isolate as resistant is 1% for all drugs tested. Second, these isolates were tested on BBL mycobacteria growth indicator tube (MGIT) liquid medium (7 mL), using the Bactec MGIT 960. All samples were processed by decontamination and the following drugs were tested: isoniazid (0.1 μg/mL), rifampicin (1 μg/mL), streptomycin (1 μg/mL), and ethambutol (5 μg/mL). Results were obtained between 7 and 9 days. Finally, the MICs to 14 drugs were determined, using the UKMYC-5 and UKMYC-6 plates (Sensititre MYCOTB plate; Thermo Fisher Scientific, Inc.).
M. Tuberculosis isolates were subcultured in Middle brook 7H9/OADC broth supplemented with Tween 80, in the presence of glass beads. One hundred microliters of standard inoculum (105 c.f.u/mL) was inoculated on 96-well plates, using a standard microdilution method, and incubated for 21 days in the presence of 5% of CO2 at 37°C. MICs were tested for isoniazid, rifampicin, ethionamide (ETH), kanamycin, amikacin (AMK), ethambutol, levofloxacin (LEV), moxifloxacin (MXF), delamanid (DLM), linezolid (LZD), clofazimine (CFZ), rifabutin (RFB), bedaquiline (BDQ), and para-aminosalicylic acid (PAS). MICs were read by the sensitive Verizon digital system (Thermo Fisher Sensititre Vizion™ Digital MIC viewing system) after 7, 10, 14, and 21 days of incubation. The plate was considered valid for reading when both the positive control wells showed a visible growth, with no evidence of macroscopic contamination. MTB H37RV was used as a reference strain.
Whole-genome sequencing
Genomic DNA was extracted from the 82 isolates using 1 mL of MGIT culture, a lysis buffer (NaCl, Triton, EDTA, TRIS), and protease K. The heat inactivation step was performed at 95°C/30 minutes. Total DNA was purified using the Promega Maxwell 16 cell DNA purification kit (AS 1020), and the final concentration was quantified by a Qubit high sensitivity DNA assay (Life Technologies) spectrophotometer with a fluorescent detection system (Qubit 3.0 Fluorometer).
A library preparation was performed by the Nextera XT DNA Library prep kit (Illumina, San Diego). All isolates were sequenced on the Illumina NextSeq500 System (Illumina) according to the manufacturer's instruction. MTBseq pipeline was used to interpret the generated fastq files to analyze the mutations involved in drug resistance and to determine the lineages and intertransmission chains. 6 WGS files from this study have been submitted to the European Nucleotide Archive as fastq files under study accession no. PRJEB41267.
Statistical analysis
Statistical analysis was performed to estimate the significance of differences between regions and lineages. Chi-square test or Fisher's exact test, respectively, were used (XLSTAT-Pro). Associations between examined variables were assessed using contingency tables. Any value of p < 0.05 was considered significant.
Results
Epidemiological characteristics and phenotypic resistance
With the first 100 selected isolates, only 82 completed the DST and WGS analysis, the other 18 isolates did not give conclusive results, either for nongrowth or for contamination during DNA extraction. Samples were mainly obtained from sputum (57), gastric tubing (11), bronchial aspiration (9), and pleural fluid (5). Twenty-eight patients were under treatment or already treated, but 54 did not receive any treatment. The other epidemiological data are presented in Table 1. On the 82 isolates, 61 strains (74.4%) were phenotypically susceptible to all the drugs tested and 21 (25.6%) were resistant (Table 1).
Epidemiological Data, Lineage Distribution, and Phenotypic Drug Susceptibility Testing of Mycobacterium tuberculosis Isolates, Recovered in Algeria (2017–2019)
Bold to highlight the drug resistance.
In accordance with the WHO new definition.
Delhi-cas, Central Asian Clade; EAI, Euro-African-Indian; EMB, Ethambutol; Euro-Am, Euro-American; INH, isoniazid; KAN, kanamycin; LAM, Latin American-Mediterranean; MDR, multidrug resistant; Mono-R, monoresistant; OFL, ofloxacin; pre-XDR, pre-extensively drug resistant; RIF, rifampicin; S, susceptible to all drugs; S, susceptible; S-type, Sardinia-Sicily type; STR, streptomycin; XDR, extensively drug resistant.
Whole-genome sequencing and drug resistance
With the WGS, we interrogated 25 genes frequently described in TB drug resistance (Table 2). Interpretation of results was carried out according to the WHO Catalogue of mutations in Mycobacterium tuberculosis complex and their association with drug resistance. 7
Phenotypic Drug Susceptibility Testing, Minimal Inhibitory Concentrations (UKMYC Plates), and Whole- Genome Sequencing of Mycobacterium tuberculosis Isolates, Recovered from Algeria (2017–2019)
Results compared with Ref. 7
AMK, amikacin; BDQ, bedaquiline; CFZ, clofazimine; DLM, delamanid; DST, drug susceptibility testing; ETH, ethionamide; LEV, levofloxacin; LZD, linezolid; MXF, moxifloxacin; NR, not realized; PAS, para-aminosalicylic acid; R, resistant; RFB, rifabutin.
A total of seventeen (17) isolates were isoniazid resistant, fifteen (15) carried the same mutation in the katG gene, namely, Ser315Thr, and 1 isolate carried mutations prom_ahpC_g-88a and Gly121Ser in the katG gene. The last isolate was phenotypic resistant, with an Arg463Leu substitution katG and ahpC promoter region (c-52t). Within ethionamide, nine isolates expressed MICs of 8 μg/mL or more. Mainly, mutations were observed in the gene ethA (Leu397Pro), four isolates showed insertions and deletions in ethA gene (4327282_C_INS, and 4327373–4327382_DEL). Another isolate with high MIC expressed the mutation prom_fabG1-inhA (c-15t).
Fifteen (15) strains reported rifampicin resistance, expressed MICs between 4 and >8 μg/mL. Ser450Leu and His445Asp mutations in rpoB gene were reported in 9 and 4 isolates, respectively.
Eleven EMB-resistant isolates carried mutation (Met306Leu) in the embB gene. However, two susceptible isolates expressed MICs of 4 μg/mL, with no modification in the embB gene.
Within streptomycin-resistant strains, diverse polymorphisms were reported in the four target genes. Isolates carrying mutations (rrs_a514c), (rrs_a514c and rrs_c1402t), (rrs_c492t and rrs_g660t), and (rrs_c517t) were streptomycin resistant. In gid gene, mutations associated with phenotypic resistance were Val124Gly, Gly73Arg, and Gly17Gly. In rpsL gene, the mutation (Lys88Met) was reported in four STR-resistant isolates.
In pncA gene, 6 polymorphisms were identified in 13 isolates, Ala146Pr, Thr142Met, Ser104Arg, Lys96Thr, Thr87Met, and Thr100Pro.
Ofloxacin phenotypic resistance was described in four isolates, two carried mutations gyrA (Asp94Asn) and gyrA (Ala90Val). In gyrB, no mutation was reported in phenotypic-resistant isolates.
Six isolates were reported kanamycin resistant, carried different mutations, in prom_eis(c-12a) and rrs gene (rrs_a514c, rrs_c1402t, rrs_c492t; and rrs_g660t) (Table 2).
Geographic distribution, molecular epidemiology, and transmission
Whole-genome analysis reported seven (7) different lineages: Haarlem (25), Latin American-Mediterranean (LAM 19), mainly T (14), Euro-American (11), Sardinia–Sicily (S-type, 10), Central Asian Clade (Delhi-cas, 2), and East African-Indian (EAI, 1), distributed in 40 provinces of Algeria (Table 1 and Fig. 1). Of the 82 patients, recent transmissions were revealed in 20 of them (Fig. 2). The Haarlem group was the most frequent M. tuberculosis lineage, widely drug susceptible. However, only two monoresistant strains, to rifampicin and streptomycin, respectively, were reported. This family is more frequent in north of Algeria compared with the south (p < 0.0001). Two patients, from distant regions (north and south), were infected by the same strain sharing the same genetic background (Fig. 2).

Geographic and provincial distribution of MTB lineages in Algeria (2017–2019). Delhi-cas, Central Asian Clade; EAI, Euro-African-Indian; Euro-Am, Euro-American; LAM, Latin American-Mediterranean; MTB, Mycobacterium tuberculosis; S-type, Sardinia-Sicily type.
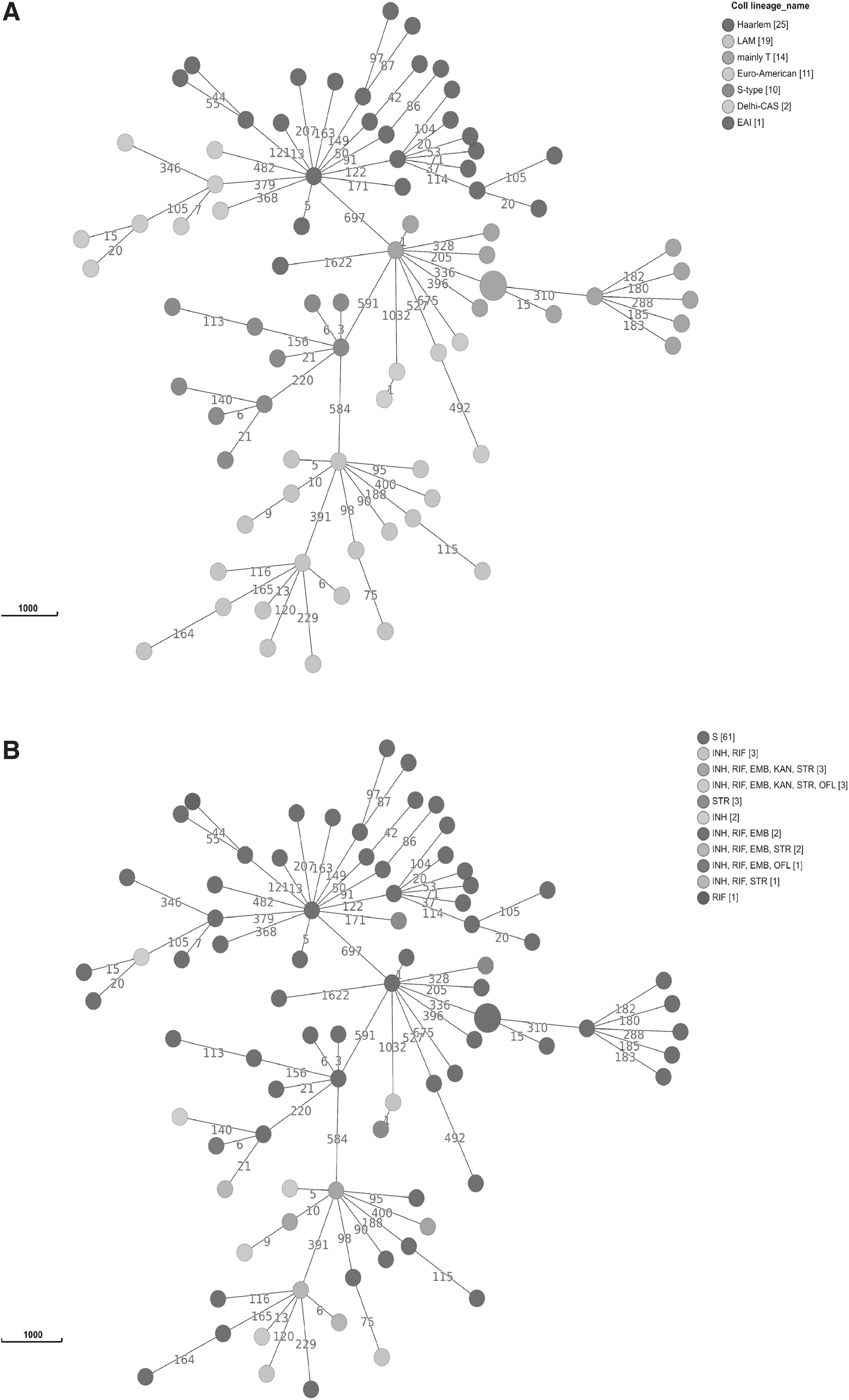
Minimum spanning tree of 82 MTB isolates, recovered from Algeria (2017–2019). The numbers on the branches indicate the genetic distance (in SNPs) to the nearest isolate and clustering made on the basis of WGS.
Nineteen isolates belonged to the LAM family, largely the most drug-resistant group, with six MDR (Table 1). This group is widely predominant in the north of the country (p = 0.013) and less frequent in the south (p < 0.0001). Two patients, one from the north and one from the west, were infected by the same pre-extensively drug-resistant (XDR)-TB isolate and neither family relationship nor recent contacts were recorded between them. Otherwise, two young patients were infected by MDR-TB isolates that differ with only two alleles; one of them has already stayed in jail. Surprisingly, a third patient was infected with a pre-XDR-TB isolate that shared the same genetic background, with five different alleles. These three patients have no family relationships, but lived in the neighboring towns of the north (Fig. 2).
Fourteen MTB isolates belonged to the mainly-T lineage; only one was phenotypic streptomycin resistant. This group is more frequent in the south (p < 0.0001) and the east (p = 0.003) of the country. Recent transmissions were observed between four patients, with the same isolate without any difference for two of them, and two strains differing only by a single allele. These two recent transmissions were recorded between patients from the south and east of the country, working in the same factory.
The Euro-American group represented 13.41% of isolates, equally distributed in different regions. Although predominantly isolates were drug susceptible, one MDR-TB and one isoniazid resistant have been reported. A recent transmission was recorded between two patients in the west of the country, with two isolates differing by five alleles.
Ten isolates (13%) belonged to the S-type lineage, four isolates were drug resistant, including three MDR-TB. This group is most common in the north (p < 0.0001) and west (p = 0.012) of the country, but never reported in the south. Two patients were infected with closely related isolates. In the first patient who was not under treatment, an MDR isolate was reported. However, for the second patient, who was under treatment, the isolate developed resistance also to ofloxacin. Both had neither family relationships nor recent contact. Moreover, three patients were infected with susceptible isolates that shared a close genetic background, even if isolated from geographically distant regions.
Only two Delhi-Cas isolates were reported in this study, from the north of the country (Bejaia). The first was an MDR-TB, isolated from a previously treated patient; the second was streptomycin resistant, from a patient never treated. Surprisingly, these two strains share the same genetic background, with no allelic differences. Finally, only one drug susceptible isolate was reported for the African-Indian (EAI) lineage, from the north of Algeria.
Discussion
Algeria is considered a medium incidence country for
Twenty-one (25.6%) isolates were resistant, to at least 1 drug, including 10 MDR and 4 pre-XDR. According to the old definition, three MDR isolates could be classified as XDR (resistant to KAN and OFL). However, under the new definition, these three isolates are nowadays considered pre-XDR isolates: TB strains that fulfill the definition of multidrug-resistant and rifampicin-resistant TB (MDR/RR-TB) and that are also resistant to any fluoroquinolone. 8 Another work on the subject has described the first isolates of MDR-TB in Algeria in recent years.9,10 Isoniazid, rifampicin, and streptomycin resistance was the most important. This is mainly due to the common prescription of these three molecules in TB treatment regimens in Algeria. Among these resistant isolates, 13 were recovered from previously treated patients, including 8 MDR and 3 pre-XDR-TB.
The 17 isoniazid-resistant isolates present the Ser315Thr mutation conferring resistance. This mutation is described in several works as the most important one conferring resistance to INH. One phenotypic INH-resistant isolate expressed, simultaneously, two mutations: prom_ahpC_(g-88a) and katG(Gly121Ser), the second one is of uncertain significance. 11 Mutations in the ahpC promoter are known for their probable role in the overexpression of the AhpC enzyme, which could compensate for the loss of KatG activity. 12
We also describe here the prom_fabG1-inhA_c-15t mutation, well known as associated with ETH resistance, in two isolates (MICs ≥8 μg/mL). Two other mutations in the ethA gene were also reported, ethA(Leu397Pro), with uncertain significance, according to Walker et al. 11 but associated with ETH resistance, according to Boonaiam et al. 13 This mutation is not reported in the WHO catalogue of mutations and variation in reported MICs, ranging from 2 to 8 μg/mL make the interpretation even more challenging. 1 The second mutation is an insertion ethA(4327282_C_INS), not reported elsewhere, to our knowledge, and it is associated with high MICs (˃8 μg/mL).
Most mutations conferring RIF resistance are located in the rpoB gene. In our study, the Ser450Leu and His445Asp mutations were the most frequent 11 and already reported in Algeria by Bouziane et al. 5 and in the neighboring countries, such as Tunisia 14 and Morocco. 15 In this study, we also report the RIF resistance conferring mutation Ser441Leu, but never described in Algeria to our knowledge, and is associated with high MICs to RIF (>4 μg/mL) and rifabutin (>2 μg/mL).
Within EMB-resistant isolates, three mutations were reported, Met306Val, Met306Leu, and Met306Ile. These mutations are well documented and confirmed to be associated with EMB resistance. 11 However, two isolates expressed MICs of 4 μg/mL, without any mutation in the embB gene. This may be due to drug susceptibility testing misinterpretation, and could also be due to other mechanisms, including compensatory mutations in embC and embA genes or cellular permeability changes. 16
In this study, 11 isolates carried mutations in the gid B gene, 2 phenotypic-resistant isolates carried only one of the mutations Val124Gly; Gly73Arg in gidB. The first one was already reported in Algeria, but not associated with STR resistance, 5 the second mutation is of uncertain significance. In rspL protein, four phenotypic STR-resistant isolates carried the mutation Lys88Met. 11 However, other phenotypic STR-resistant isolates carried mutations 1472359-C and 1472362-T in the rrs gene; to our knowledge, these mutations have not been reported before and deserve further investigation to understand whether or not they are associated with STR resistance.
For pyrazinamide resistance, here we described various mutations already reported in several studies mainly: Thr87Met, Lys96Thr, Ser104Arg, Thr100Pro, Thr142Met, and Ala146Pro.5,11 Fluoroquinolone resistance is conferred by mutations in the quinolone resistance-determining region. We report here confirmed mutations in gyrA, Ala90Val, and Asp94Asn. 11 It is interesting to note that the isolate carrying the Asp94Asn mutation expressed very high MICs (≥4 μg/mL) for LEV and MXF.
Aminoglycosides (KAN and AMK) and cyclic peptide capreomycin (CAP) are important in MDR-TB treatment. In this study, we confirmed the prom_eis(c-12a) and the rrs(c1402t) mutations in our isolates. However, one isolate carried the combined mutations rrs(c492t) and rrs(g660t), the first one is not associated with resistance, and the second is of uncertain significance. 11
Bedaquiline (BDQ), delamanid (DLM), linezolid (LZD), and clofazimine (CFZ) have shown good efficacy and low toxicity against MDR and XDR TB. 17 In this study, we reported neither interesting changes involved in resistance to BDQ, LZD, and CFZ, nor high MICs (≤0.008 to 0.5 μg/mL). These four drugs were never prescribed in Algeria, and thus, this genotypic study represents a baseline data set in the country to monitor the emergence of resistance to these drugs. However, we describe here the mutation Lys270Met in fgd1 protein and the deletion 490683–490720_DEL in fgd1 gene, all associated with low MICs (≤0.008 to 0.12 μg/mL). The first one is of uncertain significance for DLM resistance, 11 and the second mutation was reported before.
The few studies on
In Algeria, no study relationship between drug resistance and genotypes was reported. However, it is interesting to note that drug resistance was statistically associated with the LAM family, compared with the other families. Thus, of the 21 resistant isolates, 6 MDR and 3 pre-XDR-TB were described in this LAM family. This result is different from what was reported in Tunisia, where the Haarlem group was most frequently represented among MDR strains. 14 The T sublineage is present in high proportions in most African countries and distributed in the central region of Africa. 21 In this study, group T is more present in the south, a region closer to sub-Saharan countries than to the northern Mediterranean regions.
These border regions are open to population movements, particularly from the Tuareg tribe, toward Mali and Chad, where this sublineage is more frequent.23,24 In addition, southern Algeria is the gateway for sub-Saharan migrants. The S sublineage appears to be more resistant to TB drugs, with three MDR-TB and one pre-XDR-TB isolate, after LAM sublineage, and is found mainly in the north of the country. This group is rare in the African continent, 21 but it has been reported in Sicily. 20
WGS analysis confirmed cases of TB transmission in the population without confirmed family links. Although in some cases, the acquisition of resistance is acquired later, frequenting the same workplaces and neighborhoods may explain cases of recent transmission. 14
Conclusion
The reduced number of isolates is one of the main limitations of this study. Nevertheless, it is the first of its kind to explore the whole genome and to combine mutations with MICs. This work describes clearly the first pre-XDR-TB isolates in Algeria, reports the association of LAM family with drug resistance, and reveals the main lineages spreading in the country. The genetic diversity of studied isolates reflects the heterogeneity of the Algerian society, made up of populations of various origins distributed between the north, close to the Mediterranean countries, and the south, close to the sub-Saharan countries.
Thus, in the light of these results,
Footnotes
Acknowledgments
Minimum inhibitory concentration (MIC) data were generated using the UKMYC5 and UKMYC6 plates designed by the CRyPTIC Consortium. We thank all the members of the different Tuberculosis and Respiratory Disease Control Units (TRDCUs) who helped us in the collection of strains and the Ministry of Higher Education and Scientific Research (MESRS), General Direction of Scientific Research and Technological Development (DGRSDT) of Algeria.
Authors' Contributions
D.B: retrieved the strains, designed the protocols, performed the experiments, and wrote the draft; F.D.: designed the study, validated the protocols, analyzed the results, and corrected the draft; A.G.-S.: helped in carrying out the experiments and participated in the interpretation of the results; S.K.: collected epidemiological data and participated in writing and editing the article; A.S.: participated in WGS and interpretation of results; S.B.: designed the figures and tables and participated in the interpretation of the results; A.M.C.: validated the results and corrected the draft and the edition; D.M.C.: directed and designed the project, and validated revision and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.