
Abstract

Colistin resistance inflicts untreatable multi-drug-resistant (MDR) infections. It was discontinued in the 1970s owing to nephrological toxicity but was reintroduced in the 1990s to treat MDR infections. The global dissemination of mobile colistin-resistance genes (mcr) is worrisome. 1 The gut microbiome modulates a plethora of physiologies in humans. In Europe and several countries such as the United States, Brazil, and China, the use of colistin as a growth promoter in animals has been banned to curb colistin resistance. 2 Microbial colonization of the infant’s gut occurs rapidly during the perinatal period and the immediate postnatal phase despite the initial near-sterile conditions. The primary colonizers of the gut microbiome in early life influence the maturation of infants’ metabolic pathways, especially the development of the immune system. 3 In this study, we have explored the acquisition and persistence of mobile colistin-resistance genes (mcr) in 17 mother-neonate dyads’ gut microbiome, collected from birth to one year at different intervals in a hospital in the USA from 2016 to 2019. We retrieved this data from publicly available metagenome (NCBI BioProject PRJNA698986) submitted and published by Lou et al. 4
The FASTQ files were retrieved through the SRA Toolkit (https://github.com/ncbi/sra-tools/wiki/01.-Downloading-SRA-Toolkit). After the quality check using FastQC v0.11.9 (https://github.com/s-andrews/FastQC) and MultiQC v0.9.1a0 (https://github.com/MultiQC/MultiQC), MEGAHIT v. 1.2.9 (https://github.com/voutcn/megahit) was used to assemble the reads with k-min -35 and k-max -141 and k-step of 28. Bowtie v.2 2.4.1 (https://github.com/BenLangmead/bowtie2) was used to check the assembly quality. The RGI v.6.0.1 (Resistance Gene Identifier) (https://github.com/arpcard/rgi) was used to detect the mcr genes against Comprehensive Antibiotic Resistance Database v.3.2.5 (CARD). The metagenome was annotated using Prokka v.1.14.5 (https://github.com/tseemann/prokka).
Out of the 205 fecal metagenomes, seven were found to be mcr positive, and infants carried all of them. mcr-9.1 was recurrently detected in infant #8 at the 1st, 2nd, 3rd, and 4th months (SRR13622661, SRR13622650, SRR13622637, SRR13622626), and infant #40 at the 2nd and 3rd months (SRR13622610, SRR13622607). Infant #21 (SRR13622702) carried mcr-10.1 gene at the 1st month. PlasClass (https://github.com/Shamir-Lab/PlasClass) predicted the detected mcr-10.1 to be plasmid-mediated, and Kraken2 (https://github.com/DerrickWood/kraken2) predicted its carrier as Enterococcus faecalis. In infant #40, mcr-9.1 was predicted as chromosomally mediated by Klebsiella pneumoniae at the 2nd month, but later on, at the 3rd month, it was detected as plasmid-mediated in Pseudomonadota (could not be identified at species level). In infant #8, mcr-9.1 was initially carried chromosomally by Phocaeicola vulgatus at the 1st month and later on, chromosomally by Haemophilus parainfluenzae at the 2nd month and Veillonella atypica at the 4th month. Notably, it was plasmid-mediated at the 3rd month and carried by Klebsiella.
A two-component system of qseC (histidine kinase sensor) and qseB (cognate protein) was found flanking downstream to mcr-9.1 (Fig. 1). These proteins are involved in a signaling network inducing colistin resistance. In the absence of qseBC, despite carrying the mcr-9.1 gene, an isolate remains susceptible to colistin, highlighting its role in the activity of mcr. 5
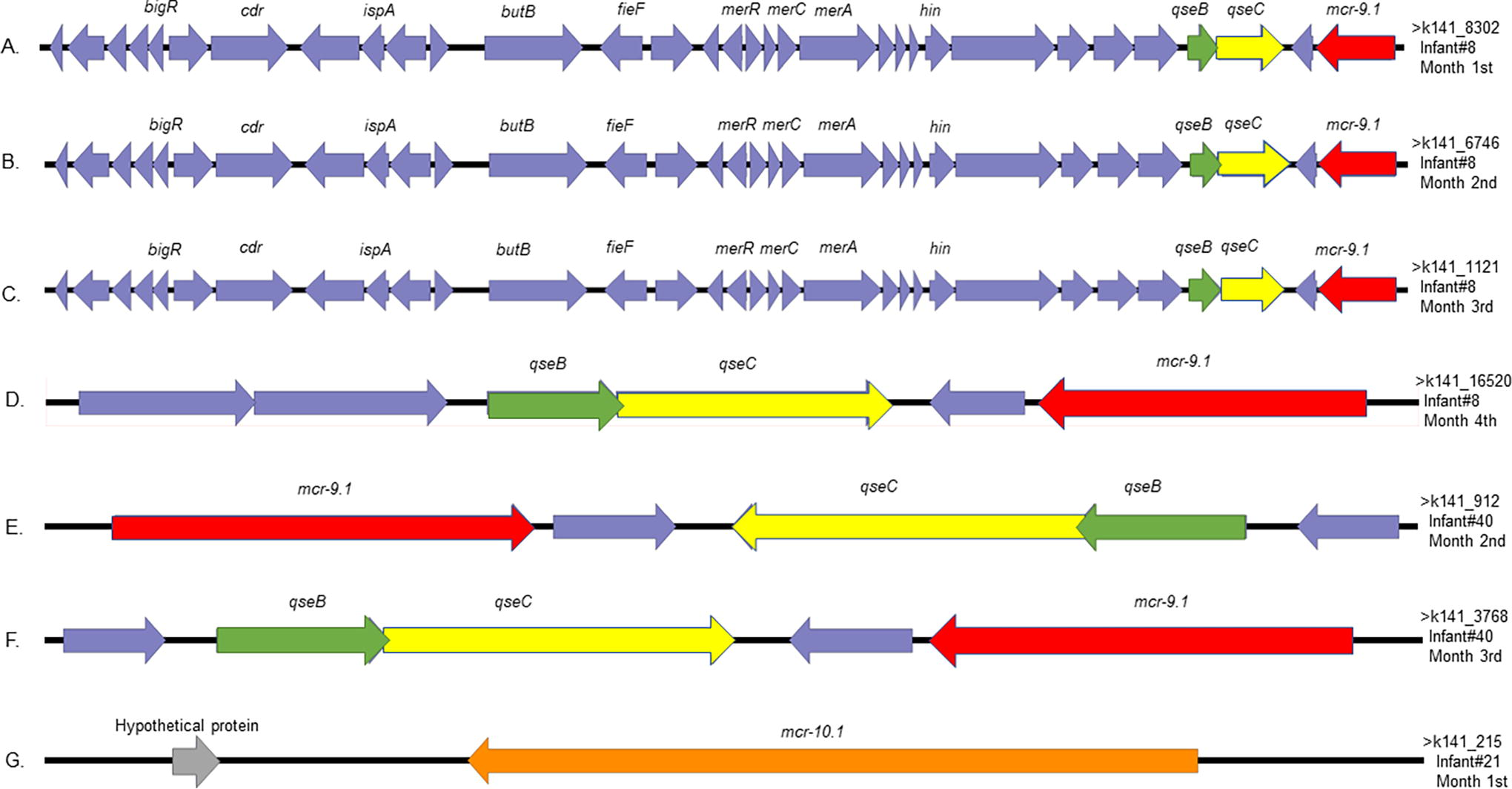
The genomic context of mcr-9.1 and mcr-10.1 represented by EasyFig (http://mjsull.github.io/EasyFig./files.html). Arrows represent the position and transcriptional direction of the open reading frame regions; mcr-9.1 gene is indicated by red color and mcr-10.1 by orange.
To the best of our knowledge, this is the first worldwide report of the mcr-10.1 gene detected in the fecal sample of an aseptic neonate. None of the infants except infant #40 were administered any antibiotics. Infant #40 was preterm and was administered vancomycin, cefepime, and amoxicillin to treat necrotizing enterocolitis. Because neither of these neonates were on colistin nor their mother was reported to have colistin resistance genes, the probable route of mcr genes acquired in neonates is nosocomial or environmental. The presence of compatible regulatory genes qseBC enhances the severity. The acquisition and persistence of these mcr genes for a prolonged duration at different ages of neonates are worrisome, exposing them to a high risk of multi-drug resistant infections.
Footnotes
Acknowledgments
We thank the DBT for support as well as internal funds of department, AMU Aligarh.
Declarations
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
The data has been retrieved from the National Center for Biotechnology Information (NCBI) database with BioProject accession number PRJNA698986.
Authors’ Contributions
A.U.K. conceived the idea. S.F. and A.T. retrieved the available data, performed computational analyses and interpreted the results. S.F. and A.T. drafted the article with critical revisions from A.U.K. All authors reviewed and approved the final manuscript.
Authors Disclosure Statement
The authors declare no conflict of interest.
Funding Information
We acknowledge funding from the DBT, Government of India, grant no. BT/PR40148/BTIS/137/20/2021, Tata Innovation Fellowship, BT/HRD/TIF/09/04/2021-22 and NNP DBT GRANT: BT/PR40180/BTIS/137/59/2023.