
Abstract
Biofilms are microbial communities and occur on different medical devices such as catheters. The formation of bacterial biofilms on medical devices leads to indwelling medical device-related infections. Since biofilm bacteria are more resistant to antibiotics than planktonic bacteria, using these antibiotics in indwelling medical device-related infections causes recurrence of infections, treatment failure, and death. Minimum inhibitory concentration (MIC) is an important reference in treating acute infections caused by planktonic bacteria. However, MIC is ineffective in indwelling medical device-related infections caused by biofilm bacteria. The study aims to demonstrate the necessity and development of effective and standard methods such as minimum biofilm prevention concentration, minimum biofilm inhibitory concentration, and minimum biofilm eradication concentration in the case of indwelling medical device-related infection. The study was conducted with 10 isolates of Staphylococcus species from patients who developed infections in the Pediatric Hematology–Oncology Department at Medical Park Bahcelievler Hospital. According to the study results, even if planktonic bacteria are sensitive to antibiotics, they can become resistant to this antibiotic when they are in a biofilm (p < 0.05, Crosstab). Also, inhibiting the growth of planktonic bacteria does not prevent biofilm formation. The study additionally revealed that inhibiting and eradicating biofilm is more difficult than preventing biofilm formation (p < 0.05).
Introduction
Biofilms are microbial communities embedded in a self-produced extracellular polymeric substance called an extracellular matrix.1,2 Biofilm matrix protects bacteria against extreme conditions such as antibiotics, chemicals, nutrient deficiency, and host defense.3,4 Biofilms form on medical devices such as urinary catheters, central venous catheters, intravenous catheters, endotracheal tubes, prosthetic heart valves, dental implants, prosthetic joints, and contact lenses, leading infections.2,4 Biofilm infections are divided into two groups based on infected area: infections resulting from microorganisms adhering to biotic or abiotic surfaces, and infections resulting from microorganisms adhering to tissue or secretion.5,6 Biofilm bacteria are 10–1,000 times more resistant to antibiotics than planktonic bacteria.7–10 While planktonic bacteria cause acute infections, biofilm bacteria cause chronic infections because they exhibit greater antibiotic resistance and can avoid host immune systems. Acute infections caused by planktonic bacteria are mostly treated with antibiotics, but chronic infections caused by biofilm bacteria are generally not treated with antibiotics. Due to the resistance of biofilm bacteria to antibiotics and host defenses, eradication of biofilms is quite difficult, and biofilms facilitate the dissemination of bacteria throughout the human body.2,5,6 It is estimated that over 80% of infections, including 60–65% of hospital-acquired infections, are biofilm-related.4,10,11
Catheters are the most widely used medical devices in clinical practices and the second major cause of infection. 12 The most common type of device-related infection is intravascular catheter infection caused by the attachment of microorganisms to the catheter. Colonization of the catheter by microorganisms causes bloodstream infection by spreading microorganisms through the blood and eventually increases mortality rates and healthcare costs.5,13 Biofilms are formed by various bacteria such as Staphylococcus aureus, Staphylococcus epidermidis, Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Proteus mirabilis. 8 The protection of bacteria provided by biofilm is crucial for the pathogenicity of many bacteria including S. aureus and S. epidermidis. S. aureus, S. epidermidis, and related coagulase-negative Staphylococcus species (CoNS) are the most common pathogens associated with indwelling medical device infections.9,14,15 Studies have drawn attention to catheter-related infections in pediatric hematology–oncology patients. The most common Gram-positive bacteria are S. epidermidis, CoNS, and S. aureus in these infections. 16 In recent years, an increase in nosocomial infections caused by Gram-positive bacteria has been observed. CoNS are among the most important causes of sepsis in neutropenic patients, as well as catheter-associated bacteremia. 17 Despite the in vitro efficacy of antibiotics, biofilm eradication still difficult. 18 The mortality rate for catheter-related bloodstream infections in children has been reported to range from 1.9% to 11%. 19
The main constraint in the treatment of indwelling medical device-related infections is that the standards for antimicrobial treatment rely on the antimicrobial susceptibilities of planktonic bacteria. Nevertheless, antibiotics that are effective on planktonic bacteria are not effective on biofilm bacteria. Consequently, using these antibiotics in indwelling medical device-related infections causes treatment failure or recurrence of infections. Indwelling medical device-related infections are associated with prolonged antibiotic therapy, reoperation, and significant morbidity.2,20,21 The minimum inhibitory concentration (MIC) is a standard for antibiotic susceptibility testing. The MIC is a reliable standard for guiding the treatment of acute infections caused by planktonic bacteria but it does not apply to chronic indwelling medical device-related infections caused by biofilm bacteria.21,22 For this reason, numerous researchers have proposed different values such as minimum biofilm prevention concentration (MBPC), minimum biofilm inhibitory concentration (MBIC), and minimum biofilm eradication concentration (MBEC) to provide an effective prediction in the treatment of many indwelling medical device-related infections.14,23–26
The study aims to highlight the necessity of methods such as MBPC, MBIC, and MBEC, rather than relying solely on MIC, for determining the antibiotic susceptibilities of biofilm bacteria in case of indwelling medical device-related infection. Additionally, the study seeks to demonstrate the application of effective and standardized methods for evaluating the antibiotic susceptibility of biofilm bacteria in a laboratory setting. In this study, the most commonly used antibiotics for the treatment of Staphylococcus species in the Pediatric Hematology–Oncology Department were investigated. Thus, it was aimed to determine whether these commonly used antibiotics are appropriate for treating indwelling medical device-related infections based on MBPC, MBIC, and MBEC values.
Materials and Methods
Bacterial strains
The study was carried out with Staphylococcus species isolated from patients who developed infections during a 10-month follow-up period in the Pediatric Hematology–Oncology Department at Medical Park Bahcelievler Hospital. After the identification of bacteria via the VITEK2 system in the hospital, they were stocked in tryptic soy broth (TSB, Oxoid) with 20% glycerol and stored at −86°C until the experiment time in the pharmaceutical microbiology laboratory of Altınbaş University. Sample types and bacterial names of the isolates used in the study are given in Table 1.
Information about Clinical Isolates
Preparation of antibiotic solutions
Antibiotic examined were teicoplanin (Sigma, T0578), meropenem (Sigma, M2574), cefepime (Sigma, A3737), linezolid (Sigma, PZ0014), amikacin (Sigma, 1019508), clarithromycin (Sigma, A3487), rifampicin, (Sigma, R3501), and trimethoprim (Sigma, T7883)/sulfamethoxazole (Sigma, S7507). The antibiotics selected for the study were chosen based on their frequent use in treating infections in the Pediatric Hematology–Oncology Department at Medical Park Bahcelievler Hospital. The antibiotics were dissolved in the appropriate solution according to the manufacturer’s instructions. Stock solutions of each antibiotic were kept at −20°C until experiment day when they were freshly adjusted to the right concentration.
MIC and minimum bactericidal concentration of antibiotics on planktonic bacteria
MIC and minimum bactericidal concentration (MBC) values were performed using the reference broth microdilution method established by The Clinical and Laboratory Standards Institute (CLSI). 27 MIC was determined as the lowest concentration of antibiotic in which there was no visible growth. For MBC analyses, 10 µL of the sample from wells with no visible growth were subcultured on Mueller Hinton agar (MHA, Becton Dickinson) and incubated at 35°C for 24 hours. MBC was determined as the lowest antibiotic concentration that kills bacteria at a rate of more than 99.9%. 15 S. aureus ATCC 25923 and S. epidermidis ATCC 35984 were used as experiment control. All experiments were performed in triplicate. Results were averaged and standard deviations were calculated.
MBPC of antibiotics on developing biofilms
MBPC analyses were performed as stated in prior studies with some modifications.14,23,24,28 After following CLSI guidelines for planktonic bacteria, nonadherent cells were removed, and wells were washed three times with 200 µL sterile physiological saline. The remaining cells were suspended with 200 µL of TSB with 1% glucose and were incubated at 35°C for 20 hours. After that, the supernatant was discarded and the wells were washed three times with 200 µL sterile physiological saline. Subsequently, wells were dried at 60°C for 45 minutes, then 150 µL of 0.5% crystal violet was added to the well and waited for 15 minutes at room temperature. At the end of the staining period, crystal violet was discharged and 200 µL 95% ethanol was added to wells and incubated for 15 minutes at room temperature. After that, wells were read at 450 nm with a microplate reader (Biotek synery microplate reader H1). In total, 200 µL of TSB with 1% glucose and biofilm-producing S. aureus ATCC 25923 and biofilm-producing S. epidermidis ATCC 35984 were used as positive controls. In total, 200 µL of 95% ethanol was used as negative control and MBPC was determined as the lowest concentration of antibiotic in the well that visually prevents biofilm formation. All experiments were performed in triplicate. Results were averaged and standard deviations were calculated.
MBIC and MBEC of antibiotics on 24-hour biofilms
MBIC analyses were performed as stated by prior studies with some modifications.14,21,23,25,28,29 A total of 20 µL of the bacterial suspension prepared McFarland 0.5 turbidity standard and 180 µL of TSB with 1% glucose were added into the wells of the flat-bottomed 96-well microtiter plates and incubated for 24 hours at 35°C for 24-hour biofilm formation. After incubation period, nonadherent cells were removed, and wells were washed three times with 200 µL sterile physiological saline. The remaining cells were suspended with 100 µL of Mueller Hinton broth (MHB, Becton Dickinson) and 100 µL of antibiotic solution prepared in twofold decreasing concentrations was added to wells. Microtiter plates were incubated at 35°C for 20 hours. After that, the supernatant was discarded and wells were stained with crystal violet and read at 450 nm with a microplate reader as described above. Overall, 200 µL of MHB and biofilm-producing S. aureus ATCC 25923 and biofilm-producing S. epidermidis ATCC 35984 were used as positive controls. In total, 200 µL of 95% ethanol was used as negative control, and MBIC was determined as the lowest antibiotic concentration in the well closest to negative control. MBIC analysis was performed in two series. One series was used for the crystal violet experiment while the other series was used for MBEC analysis. For MBEC analyses, the first step of the analysis mentioned above was carried out and MBIC was determined as the last well in which there was no visible growth. Then, 10 µL of the sample was taken from the well with no visible growth and subcultured on MHA. Agar plates were incubated at 35°C for 24 hours. The lowest antibiotic concentration that kills bacteria with a rate of >99.9% was determined as MBEC. All experiments were performed in triplicate. Results were averaged and standard deviations were calculated.
Statistical analyses
Crosstab was used to compare the groups (MIC, MBC, MBPC, MBIC crystal violet, MBIC conventional culture, MBEC) for each antibiotic pairwise. To account for multiple comparisons, post hoc corrections were applied using the Bonferroni method. The difference was considered significant at p < 0.05. The statistical analysis was conducted using the SPSS 25.0 (Statistical Package for Social Sciences). Ten isolates of Staphylococcus species were used in the study. Additionally, to ensure reproducibility and minimize interassay variability, all experiments were performed in triplicate and results were averaged and standard deviations were calculated.
Results
Results of MIC and MBC of antibiotics on planktonic bacteria
According to the results of MIC analyses, C1, C3, and C6 bacteria were sensitive to all antibiotics. C2 bacterium was resistant to clarithromycin, C4 bacterium was resistant to cefepime, meropenem, clarithromycin, and trimethoprim/sulfamethoxazole, C5 and C7 bacteria were resistant to clarithromycin and trimethoprim/sulfamethoxazole. C8 bacterium was resistant to amikacin, cefepime, meropenem, clarithromycin, trimethoprim/sulfamethoxazole, and rifampicin; C9 bacterium was intermediately sensitive/resistant to teicoplanin and resistant to amikacin, cefepime, meropenem, clarithromycin, and trimethoprim/sulfamethoxazole; and C10 bacterium was resistant to amikacin, cefepime, meropenem, clarithromycin, and trimethoprim/sulfamethoxazole (Table 2). Six of the bacteria developed resistance to more than one antibiotic. Teicoplanin, linezolid, and rifampicin had a growth-inhibitory effect on most bacteria except rifampicin on C8. Also, it was found that MBC values were higher than the MIC values for many antibiotics (Table 2). Statistical analyses showed significant differences between MIC and MBC for antibiotics (p < 0.05).
Minimum Inhibitory Concentration and Minimum Bactericidal Concentration Values of Planktonic Bacteria
N.C.: Not cultivated due to the growth could not be inhibited even with the highest concentration of antibiotic used in the experiment.
Units of antibiotics: µg/mL.
Bold indicates the resistant bacteria according to Clinical and Laboratory Standards Institute 2024, 27 EUCAST 2025 (European Committee on Antimicrobial Susceptibility Testing), 30 and EUCAST quality control recommendations for MIC determination 2025. 31
MBC, minimum bactericidal concentration; MIC, minimum inhibitory concentration.
Results of MBPC of antibiotics on developing biofilms
It was also determined that the MBPC values were higher than the MIC values for many antibiotics. These results showed that the MICs of antibiotics used for planktonic bacteria are not effective in the prevention of biofilm formation (Table 3).
Minimum Biofilm Prevention Concentration Values of Developing Biofilms
Units of antibiotics: µg/mL.
When we compared the MBC and MBPC values of antibiotics, it was revealed that MBC values and MBPC values were the same for some antibiotics such as cefepime on C3 (8 µg/mL), meropenem on C7 (4 µg/mL). C3 and C7 bacteria were sensitive to cefepime and meropenem, respectively. However, for some antibiotics, MBPC values were lower than MBC values but again higher than MIC values such as teicoplanin on C4 (MIC = 4 µg/mL, MBC = 32 µg/mL, MBPC = 8 µg/mL), linezolid on C10 (MIC = 1 µg/mL, MBC >64 µg/mL, MBPC = 16 µg/mL). Statistical analyses showed significant differences between values of MBC and MBPC for teicoplanin and linezolid (p < 0.05). C4 and C10 bacteria were sensitive to teicoplanin and linezolid, respectively. Statistical difference was detected between values of MIC and MBPC for only linezolid (p < 0.05).
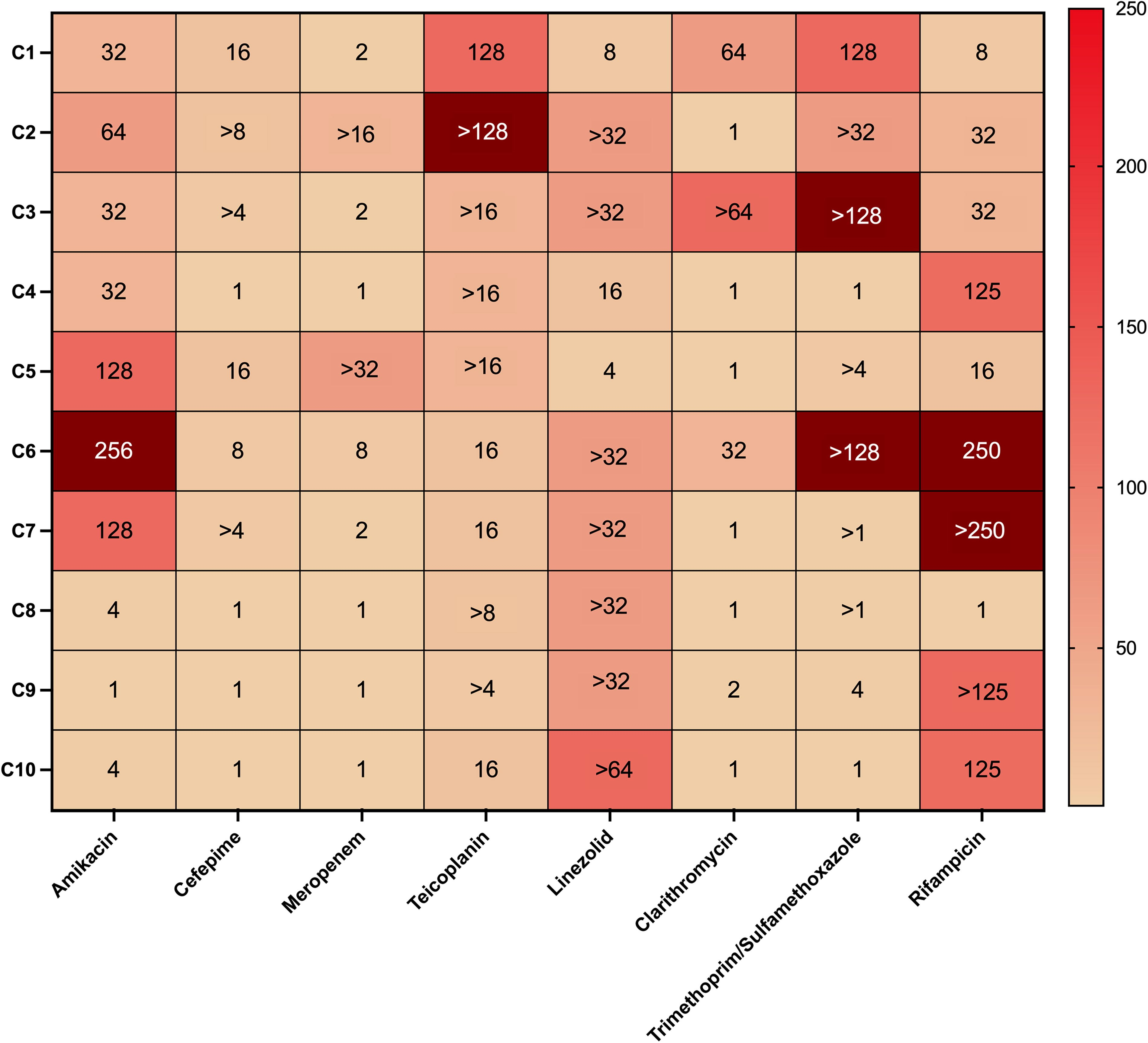
Results of MBIC and MBEC of antibiotics on 24-hour biofilms
According to the results of MBIC analyses, it was determined that MBIC values were higher than MIC values for many antibiotics. It has been shown that MIC values of many antibiotics as well as the highest concentrations used in the study were not effective for inhibition on the 24-hour biofilm (Table 4).
Minimum Biofilm Inhibitory Concentration and Minimum Biofilm Eradication Concentration Values of 24-Hour Biofilm
N.C.: Not cultivated due to the growth could not be inhibited even with the highest concentration of antibiotic used in the experiment.
Units of antibiotics: µg/mL.
Bolds indicates the minimum biofilm inhibitory concentration values obtained with the conventional culture method are different from the minimum biofilm inhibitory concentration values obtained with the crystal violet method.
MBEC, minimum biofilm eradication concentration; MBIC, minimum biofilm inhibitory concentration.
The study results showed that there are significant differences between the MIC and the MBIC-MBEC values of antibiotics. MBIC/MIC and MBEC/MIC ratios were illustrated using GraphPad Prism Software ver. 10.0 (California, USA) in Figures 1 and 2, respectively. It has been confirmed that MIC values of antibiotics determined for planktonic bacteria were not effective in inhibition and eradication of biofilm bacteria (p < 0.05).
MBIC/MIC ratios of antibiotics. MBIC, minimum biofilm inhibitory concentration; MIC, minimum inhibitory concentration.
According to the results of MBEC, it was found that only teicoplanin has a lethal effect on C6 at 32 µg/mL. The remaining antibiotics had no lethal effect on biofilm at the concentrations used in the study (Table 4). When we compared the MBC and MBEC values of antibiotics, it was found that MBEC values were higher than MBC values for most antibiotics such as amikacin on C1 (MBEC >128 µg/mL, MBC = 4 µg/mL), rifampicin on C6 (MBEC >1 µg/mL, MBC = 0.004 µg/mL). The results of the study indicated that MBC values of antibiotics did not kill the biofilm bacteria. Statistical analyses showed significant differences between values of MBC and MBEC for all antibiotics (p < 0.05). So, biofilm bacteria had higher MIC and MBC values than their planktonic form. Also, when we compared the values of MBIC and MBEC, statistical differences were detected for all antibiotics (p < 0.05).
Also, results show that MBPC values of antibiotics that prevent the biofilm formation did not inhibit the 24-hour biofilm bacteria such as trimethoprim/sulfamethoxazole on C1 (MBPC = 8/152 µg/mL, MBIC = 32/608 µg/mL), clarithromycin on C6 (MBPC = 1 µg/mL, MBIC = 16 µg/mL). It is revealed that inhibition of biofilm bacteria is harder than prevention of biofilm formation (p < 0.05).
MBIC values were measured spectrophotometrically after crystal violet staining and determined with traditional culture and the same results were obtained with little exception such as rifampicin for C2 and C3. It was revealed that the sensitivity of both methods for the determination of MBIC is the same (Table 4).
Discussion
Antimicrobial susceptibility tests used to determine MIC show planktonic bacteria’ antibiotic susceptibility.32,33 While MIC is a gold standard for predicting antibiotics for planktonic bacteria, it fails to provide adequate information for treating biofilm infections, which are more resistant to antibiotics34,35 Consequently, traditional antimicrobial susceptibility tests may cause treatment failure and infection recurrence.2,35 Assessing antibiotic susceptibilities of biofilm bacteria can guide the treatment of indwelling medical device-related infections. 35
Various methods were developed for determining the antibiotic susceptibilities of diverse biofilm bacteria; however, they lack standardization.14,21–25,28,29,33,35–37 One of the analyses performed using these methods is the determination of MBPC. Our study results indicated that MBPC values were higher than MIC values for many antibiotics. For example, 1- to 16-fold higher concentration of amikacin, 1- to 32-fold higher concentration of teicoplanin were required to prevent biofilm formation than to inhibit the growth of planktonic bacteria. Laplante and Mermel examined the impact of daptomycin and vancomycin on preventing biofilm formation by S. aureus and S. epidermidis. They found similar results to our study, their study results revealed that effective antibiotic concentrations for preventing biofilm formation were greater than MIC breakpoints determined by CLSI. 14
Another analysis of antibiotic susceptibility of biofilm was the determination of MBIC and MBEC. According to the results of our study, 1–256 times higher concentration of amikacin and 1 to >128 times higher concentration of trimethoprim/sulfamethoxazole were needed for growth inhibition of biofilm bacteria than planktonic bacteria (Fig. 1). As stated in the main hypothesis of the study, biofilm bacteria are more resistant to antibiotics than their planktonic forms. El-Azizi et al. analyzed the efficacy of several antibiotics on intact and disrupted biofilm by S. aureus and S. epidermidis. They found increased antibiotic resistance in both, although intact biofilm had higher resistance to antibiotics than disrupted biofilms. The researchers found that 100–4,000 times higher concentrations of quinupristin/dalfopristin and 25–1,000 times higher concentrations of vancomycin and linezolid were needed for growth inhibition of biofilm bacteria than planktonic bacteria. Also, all these high concentrations of antibiotics did not kill 99.9% of microorganisms in disrupted biofilm. 38 Melchoir et al. analyzed antibiotic susceptibilities of S. aureus isolates from bovine mastitis, and they found that MBEC values of antibiotics were roughly 100–1,000 times higher than MIC values of planktonic bacteria. Furthermore, MBEC values were predominantly higher than the concentration of antibiotics used in analyses. 26 According to the results of our study, MBEC values of amikacin >4 to >512 times higher for amikacin and >4 to >256 times higher for trimethoprim/sulfamethoxazole than MIC values of these antibiotics (Fig. 2).

MBEC/MIC ratios of antibiotics. MBEC, minimum biofilm eradication concentration; MIC, minimum inhibitory concentration.
Based on our study findings, among all antibiotics, MBEC values were 1 to >8 times higher than MBIC values such as teicoplanin on C6 and meropenem on C1 (Table 4). Furthermore, when assessing the MBIC/MIC and MBEC/MIC ratios of all bacteria, the ratios varied between 1–256 and >2 to >512, respectively (Figs. 1–2). For example, MBIC/MIC ratios of rifampicin were 1 to >250 (Fig. 1) and MBEC/MIC ratios of rifampicin were >32 to >500 (Fig. 2). MBIC/MIC ratios of teicoplanin were >4 to >128 (Fig. 1) and MBEC/MIC ratios of teicoplanin were 16 to >256 (Fig. 2). Also, all bacteria were sensitive to linezolid in planktonic form, but MBIC/MIC ratios of linezolid were 4 to >64 (Fig. 1). Our results are consistent with the results of prior studies. Reiter et al. showed that MBEC values of gentamycin, linezolid, rifampicin, and vancomycin were one to seven times higher than MBIC values of S. epidermidis isolates. Also, when they evaluated MBIC/MIC and MBEC/MIC ratios, they found that biofilm required a higher concentration of antibiotics to inhibit and eradicate than planktonic bacteria. Additionally, they found that all methicillin-resistant S. epidermidis were sensitive to linezolid and linezolid exhibited superior effectiveness on biofilm bacteria. According to their study, the MBIC range was 2–128 µg/mL and the MBEC range was 4–256 µg/mL for linezolid. 37 Laplante and Mermel analyzed the daptomycin and vancomycin susceptibilities on 24-hour established biofilm by S. epidermidis and S. aureus and they found that MBEC values were four to six times higher than MIC values for daptomycin and MBEC values were two to four times higher than MIC values for vancomycin, respectively. 14
Mottola et al. analyzed the susceptibilities of 10 antibiotics on Staphylococcus isolates in both planktonic and biofilm forms. They found that all MBIC and MBEC values were greater than MIC values. For example, they found that for linezolid, MIC range was 1–2 μg/mL, MBIC range was 1 to >1,024 μg/mL, MBEC range was 4 to >1,024 μg/mL; for meropenem, MIC range was 0.015–16 μg/mL, MBIC range was 0.5–32 μg/mL, and MBEC range was 0.5 to >1,024 μg/mL. 25 These results are consistent with the results of our study. According to results of our study, for linezolid, MIC range was 1–4 μg/mL, MBIC range was 8 to >64 μg/mL, and MBEC range was >64 μg/mL; for meropenem, MIC range was 0.125 to >4 μg/mL, MBIC range was 0.5 to >4 μg/mL, and MBEC range was >4 μg/mL. Brady et al. examined the antibiotic susceptibilities of 20 Staphylococcus isolates in both biofilm and planktonic forms. They found that while the most planktonic form of bacteria was susceptible to most antibiotics, they exhibited high MBEC values in biofilm. 33 Our results are similar to this study. Based on our analysis, all bacteria were susceptible to teicoplanin and linezolid. However, MBEC values of teicoplanin were >64 µg/mL (except C6), and MBEC values of linezolid were >64 µg/mL. These values exceeded the MIC of planktonic bacteria and the MIC breakpoints of these antibiotics.
According to the results of our study rifampicin was one of the most effective antibiotics on biofilm. All bacteria (except C8) were sensitive to rifampicin in planktonic form. When we compared the MBPC, MBIC, and MBEC values of rifampicin on these susceptible bacteria, it was found that a concentration range of 0.004 to >1 μg/mL was needed for MBPC, a range of 0.125 to >1 μg/mL was needed for MBIC, and a concentration >1 μg/mL was needed for MBEC. It is thought that the penetration ability of rifampicin in biofilm, its ability to reach high levels in the cell, and its bactericidal effect have important roles in antibiofilm activity of rifampicin.39,40 A prior study conducted by Koch et al. analyzed the susceptibilities of seven antibiotics on S. epidermidis in biofilm and planktonic form. They found that among the different antibiotics only rifampicin and doxycycline (concentrations ranging from 32 to 2,000 µg/mL) eradicated the bacteria in established biofilm. 34
According to our findings, most antibiotics did not inhibit the growth of biofilm bacteria with studied antibiotic concentration. Also, when we compared MBIC and MBEC values, it was revealed that MBEC values were higher than MBIC values for all antibiotics (except teicoplanin on C6). These findings demonstrated the presence of living bacteria in biofilm, despite the application of antibiotics that inhibit the growth of biofilm bacteria. As a result, persister cells of biofilm required a considerably greater concentration of antibiotic to completely eradication. Moreover, MBEC analyses revealed that vast majority of antibiotics with studied concentration did not kill biofilm bacteria. When we compared the MBC and MBEC values of antibiotics, significant differences were detected. For example, 2 µg/mL cefepime killed the C5, while >16 µg/mL cefepime was required to kill biofilm formed by C5. 0.063 µg/mL rifampicin killed the C4, while >1 µg/mL rifampicin was required for killing biofilm formed by C4. So, it is apparent that MBC values of antibiotics do not kill the biofilm bacteria. Okae et al. investigated antibiotic susceptibilities of S. aureus in vivo biofilm and found that if antibiotics cannot penetrate the deeper part of the biofilm, bacteria continue growing during the recultivation and a much higher concentration of antibiotic is required for eradication of these persister bacteria. 36
When we compared the MBPC, MBIC, and MBEC values, it showed that MBIC and MBEC values exceeded MBPC values. These findings suggest that inhibiting and eradicating biofilm bacteria is harder than inhibiting biofilm formation. For instance, MBPC was 2 µg/mL, MBIC was 16 µg/mL, and MBEC was >16 µg/mL for clarithromycin on C1. While inhibition was possible at moderate concentrations of antibiotics, eradication was required at much higher concentrations. For instance, C1, C9, and C10 biofilms were inhibited with 32 µg/mL amikacin. However, eradication of biofilms required higher than 128 µg/mL amikacin. Fernandez-Olmos et al. investigated the susceptibilities of seven antibiotics on P. aeruginosa in planktonic and biofilm forms. They found that according to lower and upper limits of antibiotics, biofilm bactericidal concentration (BBC) values were greater than biofilm inhibition concentration (BIC) values and BIC values were greater than biofilm prevention concentration (BPC) values and were greater than biofilm values, such as BBC was 2 to >128 mg/L, BIC was 0.25–32 mg/L and BPC was 0.12–8 mg/L and for ciprofloxacin. 28 These results revealed that the detection of data related to biofilms such as MBEC can provide predictive results for the treatment of indwelling medical device-related infections, which are mostly based on MIC of planktonic bacteria, and do not respond to antibiotic therapy. 21
In our study, MBIC was measured spectrophotometrically after crystal violet staining and determined with the traditional culture method, and the same results were obtained (except rifampicin for C2 and C3). It was revealed that both methods were consistent in the determination of MBIC. Many of the articles mentioned above examined different methods for testing biofilm susceptibility of antibiotics including in vitro biofilm, in vivo biofilm, intact biofilm, disrupted biofilms, use of Calgary device, microplate surfaces, traditional culture, crystal violet staining, and measurement with spectrophotometer. All these results showed that biofilm analyses can be conducted with different methods and these methods give comparable results for understanding the antibiotic susceptibility of biofilm bacteria.
The limitation of our study is the number of clinical Staphylococcus isolates. Nevertheless, despite the limited number of isolates (10 isolates), our study indicates that biofilm bacteria have higher resistance than planktonic forms. These findings are consistent with numerous other studies in the scientific literature. Further research should be conducted to examine the antibiotic susceptibility on larger sample sizes and evaluate the combination of antibiotic susceptibilities in preventing, inhibiting, and eradicating biofilms. Recent studies on biofilm infections point out that combination therapy may be an important alternative for biofilm infections.41,42
Conclusion
MIC breakpoints are a reliable indicator of antibiotic susceptibility of planktonic bacteria however, it is not useful for eliminating biofilm infections. Even if the bacteria are sensitive to antibiotics in planktonic form, inhibiting and eradicating require much higher antibiotic concentration than the breakpoints of MIC. Standard and innovative methods should be developed for estimating the antimicrobial susceptibilities of biofilm bacteria to decrease the mortality rate of indwelling medical device-related infections. In the study, it was determined that preventing biofilm formation was easier than inhibiting and eradicating existing biofilm. However, most studies on antibiotic susceptibility of biofilms have been conducted to inhibit and/or eradicate existing biofilms. Our study results are very important in terms of drawing attention to the prevention of biofilm. Additionally, the results of this study will guide the practical use of these tests in determining antibiotic susceptibility of biofilms in indwelling medical device-related infection after being used in in vivo studies. Supporting the data obtained from in vitro studies with in vivo studies will increase the confidence in antibacterial susceptibility test results and will enable the routine use of tests such as MBIC and MBEC in a faster and more reliable manner. The routine use of MBPC, MBIC, and MBEC tests in determining antibiotic susceptibility of biofilm bacteria may increase treatment success rates for indwelling medical device-related infections.
Footnotes
Authors’ Contributions
The study was designed by C.V., N.A., B.A.A., and T.F. Collection of the samples was conducted by C.V., B.A.A., and T.F. Experimental analyses were performed by C.V. and N.A. Data analyses were performed by C.V. The research project was supervised by C.V. Article was written by C.V. All authors read and approved the article.
Ethics Approval
This study was conducted in conformity with the principles of the Helsinki Declaration and was approved by the Istinye University Ethics Committee (November 30, 2018/No. 2018/17).
Disclosure Statement
The authors declared that no conflicts of interest exist in the research, authorship, and/or publication of this article.
Funding Information
The Altınbaş University Scientific Research Fund supported this research project under Project Number: PB2018-GÜZ-ECZ-1.