
Abstract
Background:
The metabolic syndrome is a global health problem and is associated with subsequent development of cardiovascular disease (CVD). However, data are scarce concerning prospective association of the syndrome and CVD in populations free of diabetes and previous CVD that also is free of all cardiovascular drugs. The aim of this study was to assess the risk of cardiovascular events due to the metabolic syndrome in a population-based cohort of initially healthy, low-risk, and medication-free 58-year-old Swedish men during 13-years of follow-up.
Methods:
From a total population sample of 1728 subjects, a stratified and randomly selected group of 391 subjects was included. The metabolic syndrome was defined according to the National Cholesterol Education Program. Cardiovascular events and cause of death were investigated by contact with the Centre of Epidemiology at the National Board of Health and Welfare.
Results:
The metabolic syndrome increased the risk of cardiovascular events with a hazard ratio of 2.1 [95% confidence interval (CI) 1.3–3.4], P=0.003. When adjusted for the factors of leisure-time physical activity, smoking habits, alcohol intake, and low-density lipoprotein cholesterol (LDL-C), the hazard ratio was 2.0 (95% CI 1.1–3.4), P=0.016.
Conclusion:
In a 13-year follow-up in initially healthy men, the metabolic syndrome increases the risk of cardiovascular events by two-fold. This risk was maintained also after adjustment for lifestyle factors.
Introduction
Few long-term epidemiological follow-up studies on NCEP-defined cardiovascular disease (CVD) are available on European populations. The Kuopio Ischaemic Heart Disease risk Factor Study (KIHD) and the Hoorn study investigated the association between metabolic syndrome and CVD in subjects free from diabetes and history of CVD, respectively. 6,7 The Hoorn study as well as the KIHD study showed that the NCEP definition was associated with a two-fold increase in risk of CVD when adjusted for conventional risk factors. 6,7 However, we have not been able to find data on metabolic syndrome and CVD in a population free of diabetes and previous CVD that is also free of all cardiovascular drugs, such as treatment of ischemic heart disease, heart failure, hypertension, and hyperlipidemia.
Therefore, the objective of the current study was to assess the association between NCEP-defined metabolic syndrome and cardiovascular events during a mean follow-up of 13 years in a population-based cohort of initially healthy, 58-year-old Swedish men who did not have previous CVD, diabetes, other established cardiovascular disease, or treatment with cardiovascular drugs.
Materials and Methods
Study population and study design
From a total population sample of 1728 58-year-old men, a stratified and randomly selected group with varying degrees of obesity and insulin sensitivity (n=391) was included, as previously described in detail. 8 Briefly, the goal was to screen approximately 800 subjects, who in connection with the screening examination were divided into quintiles of a body mass index (BMI)/blood glucose score, which allowed immediate stratification for further studies. A random sample of every 4th man in quintile 1 and quintile 5 and every 20th man in quintiles 2–4 was invited for further examinations. 8
All subjects were of Swedish ancestry and lived in the Gothenburg region. Exclusion criteria were cardiovascular disease, clinical diabetes mellitus (fasting blood glucose ≥6.1 mmol/L (109.8 mg/dL) or medication) or other clinically overt disease, untreated diastolic blood pressure >100 mmHg, treatment with cardiovascular drugs (i.e., treatment of ischemic heart disease, heart failure, hypertension, hyperlipidemia, or diabetes mellitus), or unwillingness to participate. These inclusion and exclusion criteria ascertained that no previous cardiovascular disease would confound our follow-up results and at the same time the number of subjects with metabolic syndrome would be sufficient. The subjects received both written and oral information before they gave their consent to participate. The ethics committee at Sahlgrenska University Hospital approved the study.
Baseline measurements
Previously described questionnaires were used to evaluate history of previous and current disease, smoking habits (current smoker, former smoker, or never smoked), and alcohol consumption. 8 Alcohol consumption was expressed as grams of alcohol per day. Body weight, waist and hip circumference, and sagittal abdominal diameter (i.e., the distance from the back to the upper abdomen, midway between the top of the pelvis and the bottom of the ribs, measured in a supine position) were measured with subjects dressed in underwear. Blood pressure was measured twice after 5 min of supine rest. Heart rate was recorded from a 12-lead standard electrocardiogram (ECG).
Venous blood samples were drawn after a fasting period of at least 6 h. Cholesterol and triglyceride levels were determined by enzymatic techniques (Thermo Fisher Scientific Oy, Vantaa, Finland). HDL-C was determined after precipitation of apolipoprotein B (ApoB)-containing lipoproteins, and low-density lipoprotein cholesterol (LDL-C) was calculated as described by Friedewald et al. 9
NCEP definition of the metabolic syndrome
According to the NCEP, the diagnostic criteria for metabolic syndrome are fasting hyperglycemia, high triglycerides, low HDL-C, hypertension, and central fat distribution (Table 1). 10 According to recommendations from the International Diabetes Federation (IDF) in studies of populations of Europid origin, prevalence should be given using both European and North American cut-points for waist-circumference. 11 Therefore, waist girth >94 cm was also used in the analyses.
NCEP ATP III, National Cholesterol Education Program Adult Treatment Panel III; HDL-C, high-density lipoprotein cholesterol.
Ascertainment of cardiovascular events
Cardiovascular events during 13 years of follow-up were defined as cardiovascular death or nonfatal myocardial infarction (MI), nonfatal stroke, claudication, or revascularization procedures (only one event, the first occurring was counted in each subject). The events and cause of death were collected searching The Swedish national inpatient register (IPR) after contact with the Centre of Epidemiology at the National Board of Health and Welfare. The IPR has a high external and internal validity for cardiovascular disease. 12
Statistics
Univariate comparisons between the groups were performed using the Mann–Whitney U-test or chi-squared test. Cox proportional hazard models were used to calculate hazard ratios (HR) for cardiovascular events in relation to metabolic syndrome. Statistical significance was considered to be a P value<0.05. All statistical analyses were performed using PASW Statistics 18 (SPSS Inc.). Kaplan–Meier curves were used to illustrate the cumulative event-free rate.
Results
As previously reported, 23% of the men in this group were diagnosed as having metabolic syndrome according to the NCEP criteria with waist circumference >102 cm. 13 When waist circumference ≥94 cm was used with the NCEP definition of metabolic syndrome, the prevalence was 28%.
In the 13-year follow-up, 69 cardiovascular events were recorded (17.8% of the population). In total, there were 34 cases of stroke, 19 cases of MI, 14 cases who went through revascularization procedures, and 2 cases with claudication. Clinical and biochemical parameters for the groups without and with cardiovascular events are shown in Table 2. Briefly, BMI, blood pressure, and ApoB/ApoA-I ratio were significantly increased in the group who had cardiovascular events during follow-up, whereas the other parameters did not differ between the groups.
Of the 391 men included in the study, 3 had missing triglyceride and high-density lipoprotein (HDL) blood samples and could not therefore be assessed for metabolic syndrome.
Mann–Whitney U-test.
Geometric mean.
Pearson chi-squared.
CVD, cardiovascular disease; HOMA, homeostasis model assessment.
Association with cardiovascular events
In a Cox proportional hazard regression analyses (model 1) for cardiovascular events in men with versus men without the metabolic syndrome, the metabolic syndrome was associated with a 2.1-fold increased risk (P=0.003) for the NCEP definition with a waist cutoff of 102 cm. The corresponding hazard ratio was 1.9 (P=0.007) for the NCEP definition with a waist cutoff of 94 cm (Table 3). In adjusted analyses (model 2), the metabolic syndrome was associated with a 2.0-fold increased risk (P=0.016) for the NCEP definition with a waist cutoff of 102 cm. For the NCEP definition with a waist cutoff of 94 cm, the corresponding hazard ratio was 1.8 (P=0.031) (Table 3). The Kaplan–Meier survival curve of metabolic syndrome subjects compared to non–metabolic syndrome subjects is illustrated in Fig. 1.
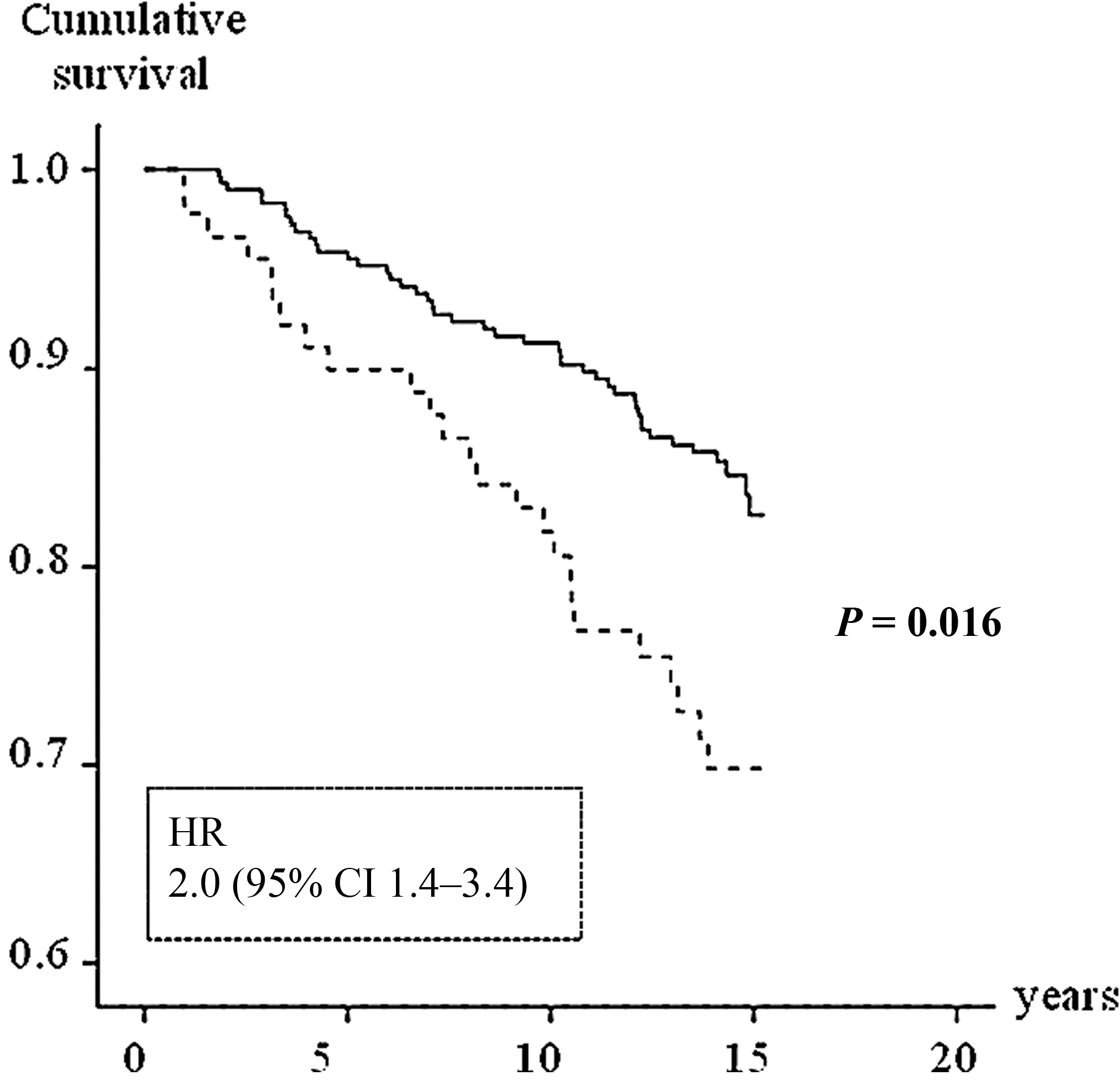
Kaplan–Meier survival curve free of cardiovascular events. The inside panel illustrates the hazard ratio (HR) of metabolic syndrome (dashed line) group versus the non–metabolic syndrome group (solid line) by the Cox regression model adjusted for leisure-time physical activity, smoking habits, alcohol intake, and low-density lipoprotein cholesterol. CI, Confidence interval.
Model 1, unadjusted; model 2, adjusted for leisure-time physical activity, smoking habits, alcohol intake, and low-density lipoprotein cholesterol.
NCEP, National Cholesterol Education Program; CI, confidence interval.
Furthermore, we performed an analysis where the study subjects were divided into three groups—one group without any risk factors for metabolic syndrome, one group with one to two risk factors, and one group that fulfilled the metabolic syndrome diagnosis with three or more risk factors. The results showed a significant linear trend toward increased quantity of cardiovascular events with increasing amount of metabolic syndrome abnormalities (P=0.002). Figure 2 shows the Kaplan–Meier survival curve for the three different groups.
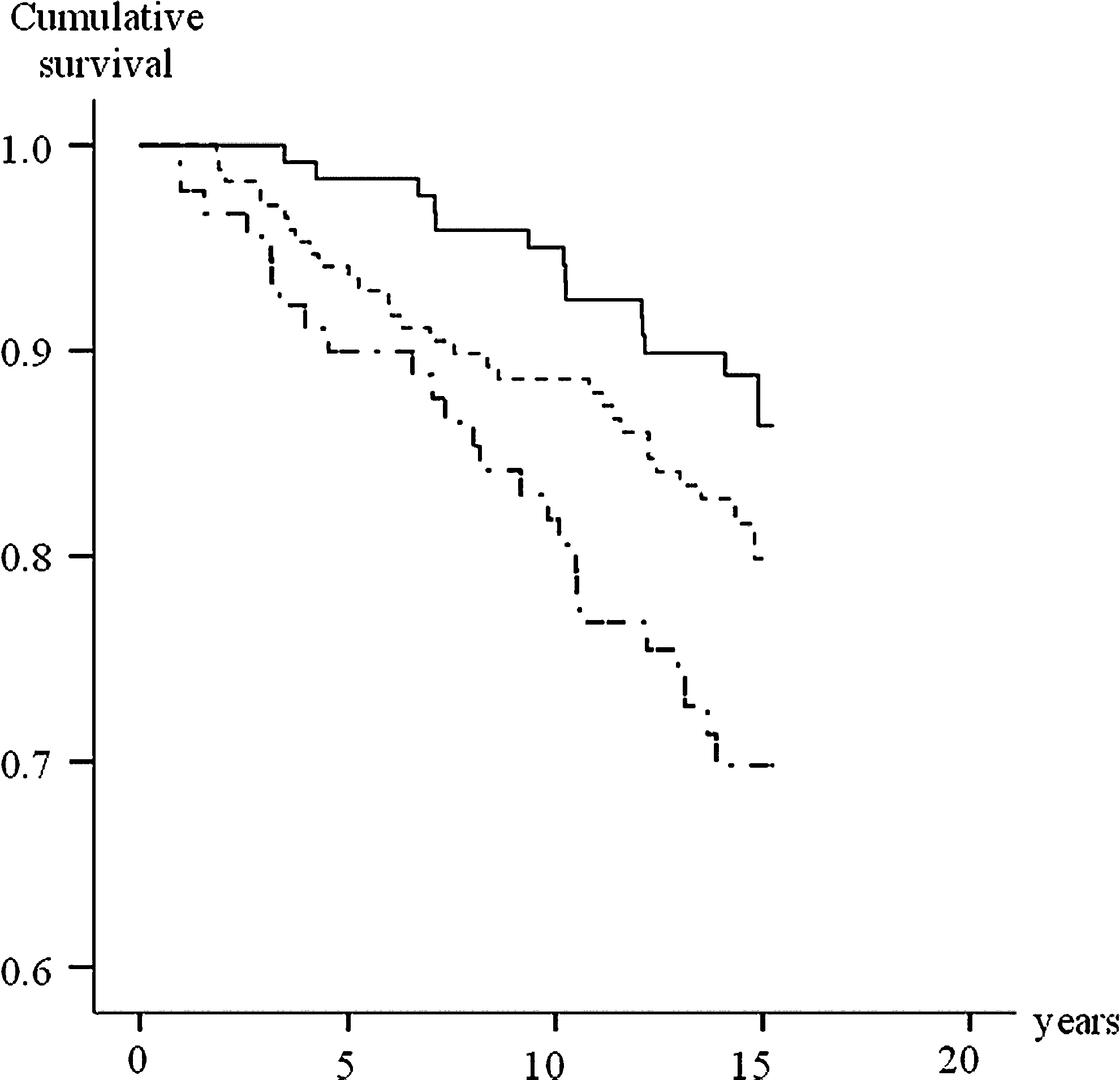
Kaplan–Meier survival curve free of cardiovascular events for the group with metabolic syndrome (dot-dashed line), the group with one to two metabolic syndrome factors (dashed line), and the group with no metabolic syndrome factors (solid line). The group with one to two metabolic syndrome factors had a hazard ratio (HR) of 1.7 [95% confidence interval (CI) 1.0–2.9, P=0.046] compared to the group with no metabolic syndrome factors.2 The group with metabolic syndrome factors had a HR of 2.9 (95% CI 1.5–5.6, P=0.001) compared to the group with no metabolic syndrome factors.
In a Cox proportional hazard regression analyses (model 1) for cardiovascular events in men with metabolic syndrome versus men without any risk factors for the metabolic syndrome, the metabolic syndrome was associated with a 2.9-fold increased risk (P=0.001) for the NCEP definition with a waist cutoff of 102 cm. The corresponding hazard ratio was 2.5 (P=0.006) for the NCEP definition with a waist cutoff of 94 cm (Table 4). In adjusted analyses (Model 2) the metabolic syndrome was associated with a 2.5-fold increased risk (p=0.016) for the NCEP definition with a waist cutoff of 102 cm. For the NCEP definition with a waist cutoff of 94 cm the corresponding hazard ratio was 2.0 (P=0.061) (Table 4). Figure 3 shows the Kaplan–Meier survival curve of metabolic sydndrome subjects compared to subjects without risk factors for metabolic syndrome.
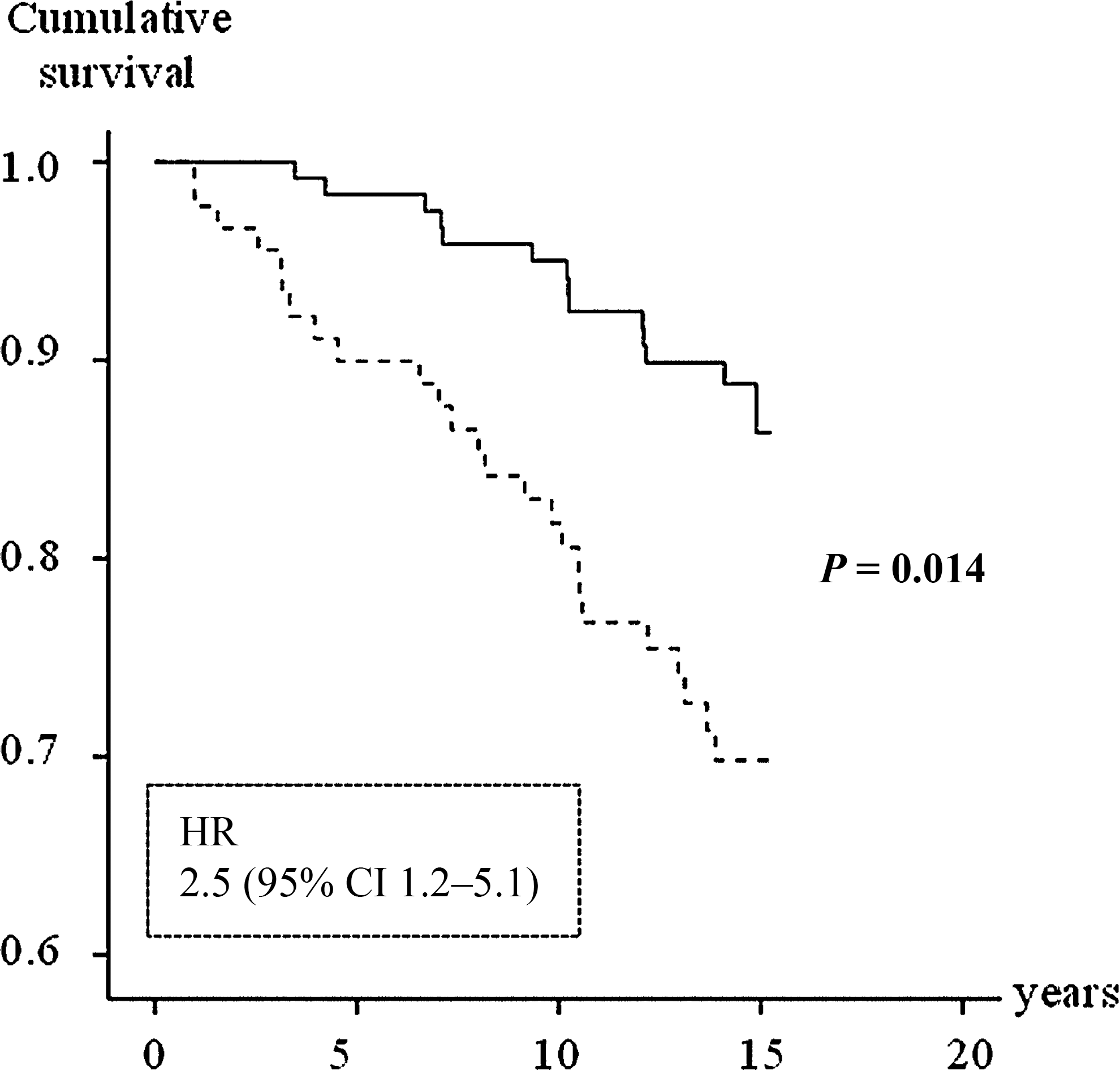
Kaplan–Meier survival curve free of cardiovascular events. The inside panel illustrates the hazard ratio of metabolic syndrome (dashed line) group versus the group without any metabolic syndrome factors (solid line) by the Cox regression model adjusted for leisure-time physical activity, smoking habits, alcohol intake, and low-density lipoprotein cholesterol (LDL-C). HR, hazard ratio; CI, confidence interval.
Model 1, unadjusted; model 2, adjusted for leisure-time physical activity, smoking habits, alcohol intake, and low-density lipoprotein cholesterol.
NCEP, National Cholesterol Education Program; CI, confidence interval.
Discussion
Prospective studies on the relationship between NCEP-defined metabolic syndrome and CVD in northern European populations are still scarce. The Hoorn study 7 and the KIHD study 6 have shown that the presence of the metabolic syndrome is associated with a significantly two-fold increased risk of CVD.
This observation is also made in the present study of initially healthy 58-year-old men, who had no history of CVD or diabetes and no treatment with cardiovascular drugs. The study showed that NCEP-defined metabolic syndrome was associated with a two-fold increase in risk of cardiovascular events. After adjustment for leisure-time physical exercise, smoking habits, and alcohol intake, the CVD risk was analogous. Furthermore, similar doubled CVD risk has been observed also in studies conducted in the United States, such as the second National Health and Nutrition Examination Survey (NHANES) 14 and the San Antonio Heart Study (SAHS) 15 and in a European study performed in a Mediterranean population. 1 However, comparisons between findings from different prospective studies have to be made with caution because of differences in characteristics of the study populations. 4
In the initial analysis performed in the present study, subjects without the syndrome were used as reference category. Many subjects without the syndrome have one or two risk factors and this may misleadingly soothe the increased risk in subjects with the syndrome. 16 Therefore, we performed an analysis in which the subjects were divided into three groups; one group with no risk factors for metabolic syndrome, that was used as reference group, one with one to two metabolic syndrome factors, and one that fulfilled the criteria for metabolic syndrome. The results showed a significant linear trend toward increased frequency of cardiovascular events with increased amount of abnormalities. When calculating the hazard ratio for CVD in this data set, the risk was nearly three-fold in the group that fulfilled the criteria for metabolic syndrome compared to the reference group. These results are in line with the Hoorn study, which showed that the CVD risk increased with the number of risk factors, 7 and with the West of Scotland Coronary Prevention Study (WOSCOPS) study, which presented a hazard ratio of 3.2 for CVD in men with three abnormalities (i.e., with the metabolic syndrome). 17 In men with metabolic syndrome as defined by the NCEP, cardiovascular events were more increased when using a waist cutoff of 102 cm than when using a waist cutoff of 94 cm, especially in the adjusted analyses.
Metabolic syndrome is an escalating public health problem that increases with age. 3,4 The prevalence of metabolic syndrome in this cohort of 58-year-old men was 23%, as previously published. 13 The prevalence is in accordance with another Swedish survey of 60-year-old men living in Stockholm, in which the observed prevalence was 24%, and with the WOSCOPS study, where the prevalence was 26% among men. 5, 7 This is to be compared with 47% in 50- to 59-year-old U.S. males in the NHANES. 18
Studies have demonstrated that lifestyle interventions such as increased physical activity have effects on prevalence of the metabolic syndrome. 5,19,20 Our research group has previously observed that metabolic syndrome was less common in a group of men who performed regular/competitive physical activities during their leisure time compared with men who spend their leisure time performing more sedentary activities. 13 Lifestyle interventions may be a relevant strategy for the management of metabolic syndrome and may reduce the risk of CVD associated with the syndrome. 4 However, our analysis showed that metabolic syndrome was an independent risk factor from leisure-time physical activity, suggesting a more complex relationship.
The strengths of this study include that the studied population consists of a well-characterized cohort of men in the same age of Swedish ancestry, living in the Göteborg area, which controls for variation in age, sex, and ethnicity. Furthermore, the included subjects were initially free of cardiovascular disease, clinical diabetes mellitus or other clinically overt disease, treatment with cardiovascular drugs, such as treatment of ischemic heart disease, heart failure, hypertension, hyperlipidemia, and diabetes mellitus that might otherwise have confounded the interpretation of results. On the other hand, a weakness of the study is that this cohort only included men of Swedish ancestry within a limited age category and with no cardiovascular drugs, so no results can be inferred to other age groups, women, other ethnicity groups or groups that are on cardiovascular medication.
In conclusion, we demonstrate in a cohort of 58-year-old Swedish men, with no previous CVD, diabetes, or treatment with cardiovascular drugs, that the presence of the metabolic syndrome according to the NCEP definition increased the risk of cardiovascular events by two-fold. We also observed a linear trend toward increased frequency of cardiovascular events with increased number of abnormalities. This suggests that it may be meaningful to detect the factors that are included in the syndrome before the sum of the parts fulfills the criteria for metabolic syndrome.
Footnotes
Acknowledgments
The authors would like to express their gratitude to all people involved in the AIR Study. Grants from the Swedish Heart-Lung Foundation, the Swedish Medical Research Council, the Swedish state under the agreement between the Swedish government and county councils concerning economic support for research and education of doctors (ALF-agreement), King Gustav and Queen Viktoria Foundation, and Astra Zeneca, Mölndal, Sweden supported this work.
Author Disclosure Statement
The authors state that they have no relationships that might lead to a conflict of interest.