
Abstract
Background:
Metabolic syndrome has been identified as a condition of childhood relatively recently. The aim in this study was to describe the prevalence of metabolic syndrome in children allowing for differences in metabolic syndrome definitions.
Methods:
This was a systematic review of the OVID, EMBASE, and CINAHL databases, capturing details of overall prevalence and prevalence within groups categorized by obesity, gender, age, and ethnicity.
Results:
In all, 378 studies published since 2003 were identified, and of these 85 papers were included in the present review. When all studies were considered, the median prevalence of metabolic syndrome in whole populations was 3.3% (range 0%–19.2%), in overweight children was 11.9% (range 2.8%–29.3%), and in obese populations was 29.2% (range 10%–66%). Within-study analyses confirmed higher prevalence for obese compared to overweight (P=0.012) and obese compared to nonobese, nonoverweight children (P<0.001). Within-study analyses also revealed higher median metabolic syndrome prevalence for boys compared to girls (5.1% versus 3.0%, P<0.001) and also in older compared with younger children (5.6% versus 2.9%, P=0.001). Limited evidence was found to suggest differences between ethnic groups, and there were insufficient studies to determine whether metabolic syndrome prevalence was increasing over time.
Conclusions:
This is the first systematic review of all of the relevant literature. It describes the magnitude of associations between metabolic syndrome and obesity, age, and gender. We find evidence that ethnicity and geography may be important to metabolic syndrome prevalence in children and these associations require further study.
Introduction
Metabolic syndrome was first considered to be a condition of adulthood and linked to cardiovascular morbidity and mortality. 4 More recently, children have been identified to have metabolic syndrome 5 and, given the rising prevalence of childhood obesity 6 and the link between obesity and metabolic syndrome, 5 there is the potential that metabolic syndrome prevalence in children will rise, with implications for future increases in cardiovascular morbidity and mortality.
But what is the prevalence of metabolic syndrome in children? Estimating the prevalence of metabolic syndrome in children is not straightforward because many different criteria have been used to define metabolic syndrome. Forty different definitions were used in one review of 27 studies 7 ; in a second paper, metabolic syndrome prevalence varied between 0% and 60% in the same group of children, depending on the diagnostic criteria applied, 8 and a third paper applied 14 definitions to a population of girls and observed metabolic syndrome prevalence between 0.4% and 24%. 9 In addition to the different components measured, e.g., insulin resistance versus fasting plasma glucose, the threshold values for “abnormal” components of metabolic syndrome vary, e.g., obesity cutoffs of 85th, 95th, or 98th body mass index (BMI) centile. A final difference between definitions is that one of the three main diagnostic criteria has obesity as an essential criterion, whereas a second has insulin resistance as a prerequisite (Table 1).
NA, not applicable.
Our group was interested in the prevalence of metabolic syndrome in children in the United Kingdom, but was not able to find a community-based study. One systematic review of the literature published between August, 2007, and January, 2009, 10 reported the prevalence in the general pediatric population to be between 1.2% and 22.6% in countries other than the United Kingdom. Here we report the results of our systematic review of international metabolic syndrome prevalence in children. Although metabolic syndrome is generally understood to be higher in children who are obese, male, and older, the magnitude of this association across studies is not described. The relationship between metabolic syndrome prevalence and ethnicity, and whether prevalence is increasing, has not been explored using a systematic approach. Our primary aim was to describe the prevalence of metabolic syndrome while considering differences in diagnostic criteria. Our secondary aim was to explore whether metabolic syndrome prevalence was influenced by gender, age, and ethnicity and whether it has changed over time.
Methods
Literature search
A literature search was run in the OVID, EMBASE, and CINAHL databases using the terms “prevalence” “metabolic syndrome X” and then limiting papers with both these terms to “child.” Papers that were not available as full text in the English language, which did not explicitly give a prevalence of metabolic syndrome, or which included less than 100 participants were excluded. The remaining full papers were reviewed by two members of the team, who individually decided whether a paper was eligible. Where there was discordance for eligibility between the two team members, the whole team met to agree on paper eligibility. For each eligible study, one of the group extracted the following fields from the paper: Date of study (or date of publication if not available), country/ies of study, criteria used for diagnosis of metabolic syndrome, individual cutoff values, mean age, gender, ethnicity of subjects, and prevalence in the following groups (if given)—whole population, nonoverweight and nonobese, overweight, obese, morbidly obese, boys, girls, and older and younger age ranges within the population.
Definitions identified
There were three overarching criteria that most studies had used (with or without modification), and these were: (1) International Diabetes Federation (IDF), 11 (2) National Cholesterol Education Program's Adult Treatment Panel III (ATP), 12 and (3) World Health Organization (WHO) 13 (Table 1). Some studies applied adult IDF and ATP criteria to pediatric populations, whereas others adopted pediatric or age-specific criteria (Table 1). All WHO criteria were age-specific. There were no studies identified that did not include some version of IDF, ATP, or WHO criteria.
Synthesis of results
Summary statistics were used to report the findings. Populations were categorized by: (1) Definition used (i.e., IDF, WHO, ATP III, or modifications thereof), (2) inclusion criteria (i.e., whole population or only overweight/obese/morbid obese), (3) data collection started before or during 2000 or after 2000 (cutoff date chosen arbitrarily; studies where years of data collection were not stated were excluded from this part of the analysis due to the variation in length of time between data collection and publication), (4) geographic area [Europe, Americas (including North, Central and South), Middle Eastern (including Tunisia, Turkey, and Iran), and Far East (including India, South Korea and China)].
Statistical analysis
Overall prevalences were expressed as a median and range of values. Due to the different criteria applied between studies, statistical analysis was limited to within-study comparison of metabolic syndrome prevalence using the Wilcoxon signed ranks test. Standard statistical software was used (SPSS 19.0.0) and significance was assumed at P<0.05.
Results
Systematic review
The initial search in March, 2011, identified 378 abstracts; 85 full papers were reviewed. Of these, 63 had applied variants of the ATP III, 26 the IDF criteria, and 15 the WHO criteria (Fig. 1; see Tables S1–S3) (Supplementary Data are available at or

Venn diagram showing the number of studies included in this review which report metabolic syndrome prevalence using Adult Treatment Panel III (ATP), World Health Organization (WHO), and International Diabetes Federation (IDF) criteria.
Prevalence in obese and nonobese populations
For all studies, the median (range) prevalence of metabolic syndrome in the whole population was 3.3% (range 0%–19.2%); it was 11.9% (2.8%–29.3%) in overweight and 29.2% (10.0%–66.0%) in obese populations. For nonobese, nonoverweight populations, the range was 0%–1%. Within studies, metabolic syndrome prevalence was lower in non obese non over-weight compared with overweight (P=0.011) 18,24,31 –35 and obese (P<0.001) 14,15,19,24,25,31 –34,36 –46 and in overweight compared with obese (P=0.012). 24,31 –34,36,37,47 –49 The WHO criteria were applied predominantly to obese populations, and this invalidated any comparison in metabolic syndrome prevalence between WHO and ATPIII and IDF criteria (see Supplementary Data). There was significant heterogeneity in the thresholds for studies that applied ATP III or IDF making comparison between these two criteria invalid. Table 2 summarizes metabolic syndrome prevalence in groups categorized by weight, IDF, WHO, or ATP criteria and also by whether age-specific or adult criteria were applied.
Studies within each criterion are separately considered “adult” cutoffs (i.e., apply adult ranges) or “age-specific” cutoffs (i.e., apply age specific cutoffs); X=no data available.
Prevalence up to and including 2000 compared with afterward
There were 62 studies where year of data collection was stated; 23 of these commenced before or during 2000. When stratified by criteria and whether age-specific values were used, there was no obvious change in metabolic syndrome prevalence comparing studies published before or during 2000 with those published after 2000 (Supplementary Table S4; see also Supplementary Data). There were four studies where the same methodology was applied in different cross-sectional surveys. Two studies applied the IDF criteria (National Health and Nutrition Examination Survey) and found that the prevalence in the United States was 4.5% in 1999 and 3.7%–3.9% in 2003, 50 whereas among South Koreans, metabolic syndrome prevalence rose from 2.2% in 1998 to 3.6% in 2001 before falling to 1.8% in 2005. 51 A third study from Iran used ATP III criteria and reported metabolic syndrome prevalence as 7.4% for 1998–2001 and 6.7% for 2003–2006. 19 A further study compared metabolic syndrome prevalence in U.S. children assessed in cross-sectional surveys in 1988–1994 and again 1999–2000 and reported an increase in prevalence from 9.2% to 12.7%. 52
Prevalence in different countries/ethnic groups
The metabolic syndrome prevalence in children from different continents varied widely (Table 3). There were 10 studies 16,42,44,53 –59 where metabolic syndrome prevalence was compared between different ethnic groups (see Supplementary Data). Although differences in metabolic syndrome prevalence between ethnic groups were present, there was no consistent pattern for one ethnic group to have a higher or lower metabolic syndrome prevalence compared to another.
Metabolic syndrome prevalence in studies of only overweight children was combined with obese children (rather than nonoverweight nonobese). Among children in Australia, the prevalence of metabolic syndrome in the whole population was 14% using age-specific ATP III criteria 65 and 33% in obese children using WHO criteria 45 .
Gender
There were 35 comparisons of metabolic syndrome prevalence between boys and girls reported in 27 studies (8 studies reported prevalence in boys and girls using more than one definition). 14,15,18,20,24,30,31,34,36,37,40,49,50,51,57,58,60 –70 The median prevalence in boys was 5.2% and girls was 3.1% (Wilcoxon signed rank test P<0.001) (Fig. 2), and when studies of obese children were excluded, the respective prevalences were 4.2% and 2.4% (P=0.031).
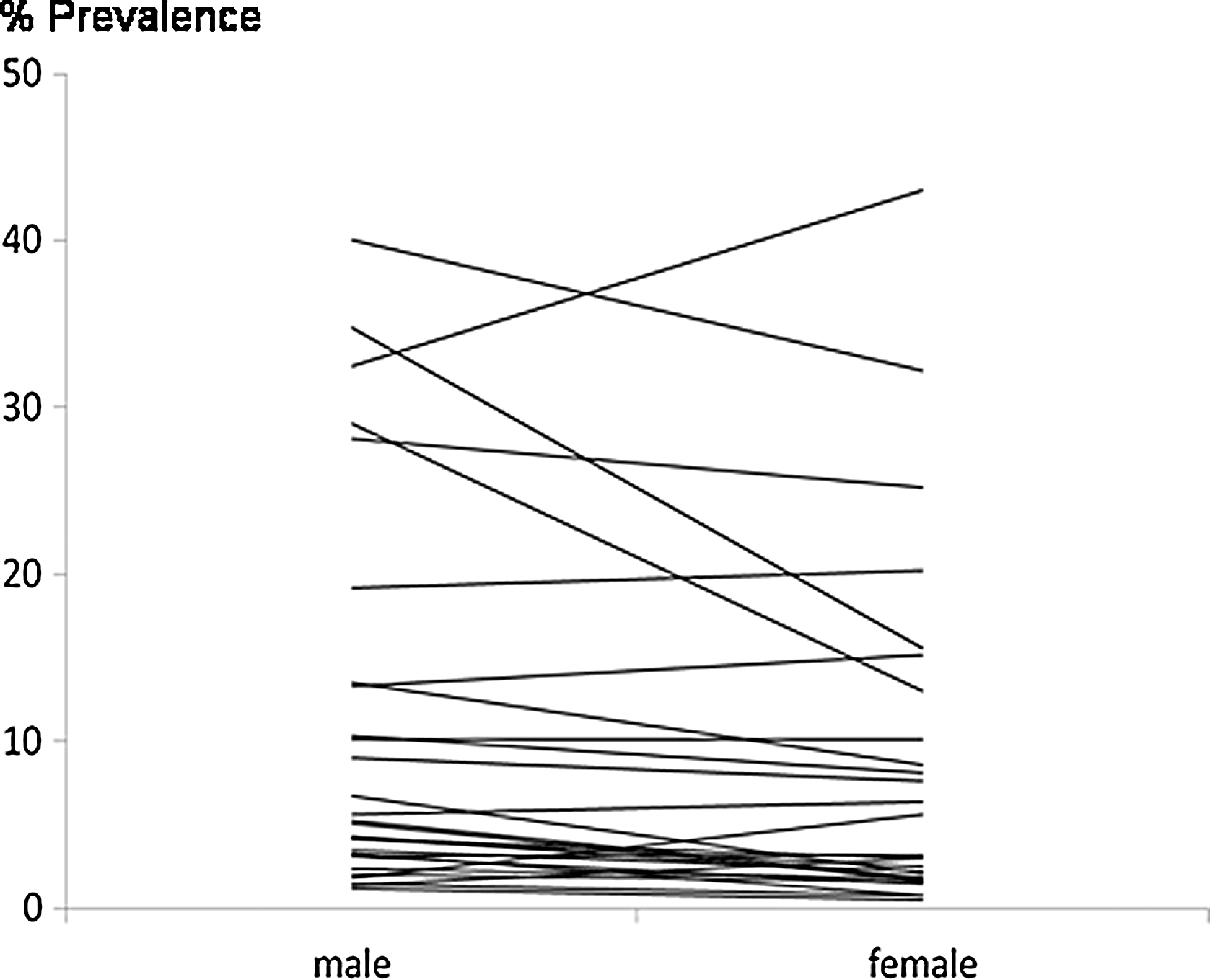
Mean percent prevalence of metabolic syndrome in boys and girls. The median prevalence in boys was 5.2% and in girls was 3.1% (Wilcoxon signed rank test, p<0.001).
Age
Nine studies (using a total of 10 metabolic syndrome definitions) reported prevalence in older and younger children within a single population. 21,50,53,54,56,57,60,71,72 Different age groups were compared, including: Child versus adolescent, 53 10 versus 15 years 57 ; 10–15 versus 16–18 60 ; 12 years versus 16–17 years 50 ; under 10 years versus adolescence 21 ; 7–11 versus 12–18 57 ; 7–11 versus 12–18 71 and 9–10 years versus 18–19 years. 54 The median metabolic syndrome prevalence for the younger age groups was 2.9% and 5.6% for the older age groups, Wilcoxon signed rank test P=0.001 (see Fig. 3). In an additional study, different criteria were applied to the same population; metabolic syndrome prevalence increased with age, but only among boys. 17
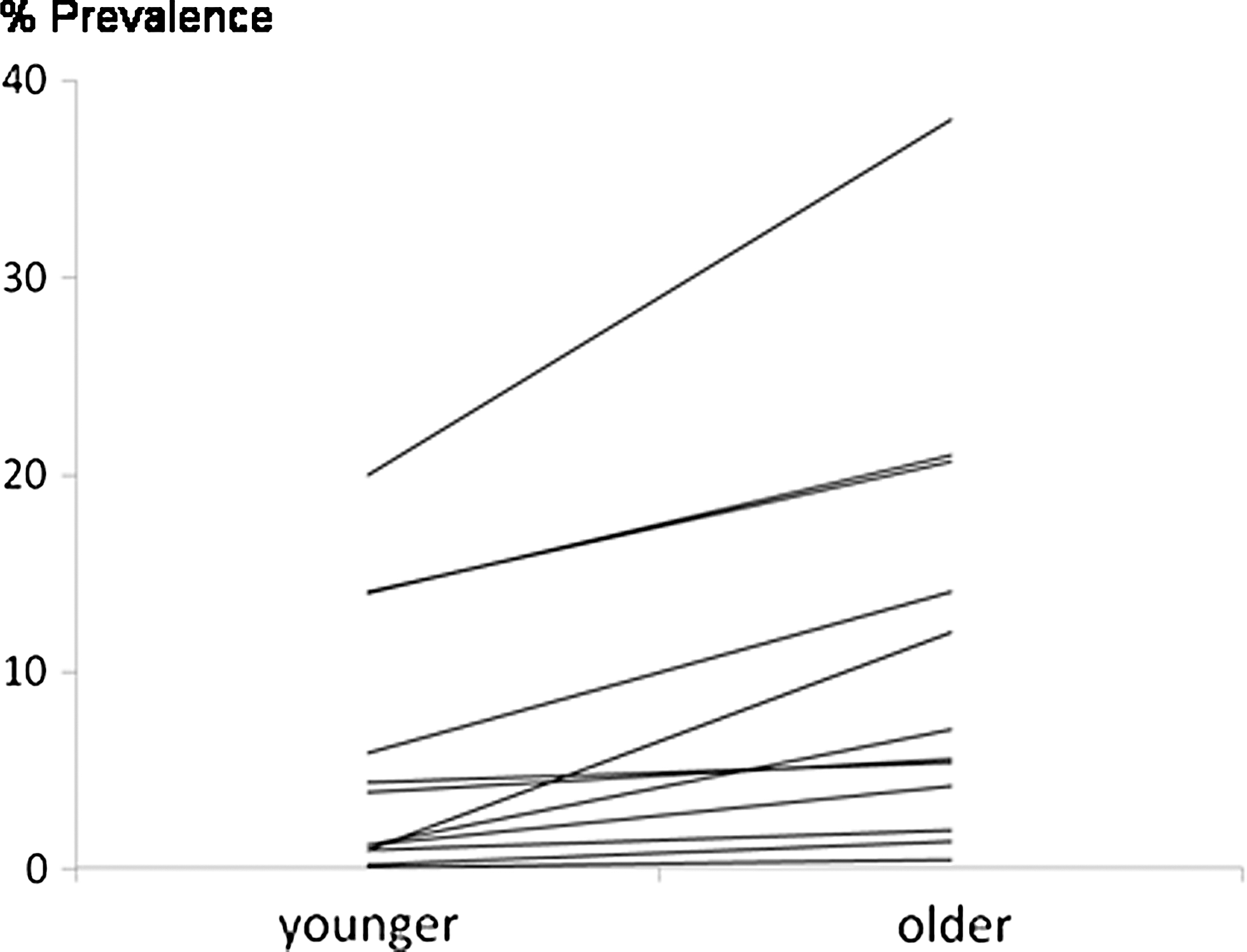
Mean percent prevalence of metabolic syndrome in younger and older children within study. Median prevalence in younger children was 2.9% and for older children was 5.6% (Wilcoxon signed rank test, p=0.001).
Discussion
This is the first systematic review of the entire literature describing the epidemiology of metabolic syndrome in children. Although metabolic syndrome prevalence is understood to be higher in children who are obese, male, and older, here we have described the magnitude of these associations after taking the whole literature into consideration. Our review also for the first time explored associations between metabolic syndrome prevalence and ethnic group and whether prevalence is increasing over time. This review summarizes the epidemiology of childhood metabolic syndrome in 2012 and identifies areas where future research could be directed.
Overall prevalence
One previous systematic review of 36 papers published between 2007 and 2009 10 and two reviews of selected studies 7,73 concluded that metabolic syndrome prevalence was highly variable between study populations and that it may prove difficult to estimate the likely prevalence of metabolic syndrome. Here we estimate metabolic syndrome prevalence for the whole population to be approximately 3% (using age-specific cutoffs), and this value is based on a large number of studies and is therefore relatively robust. Consistent with our estimated prevalence, a review article published in 2004 estimated metabolic syndrome prevalence in children at 3%–4%, 74 and a study that applied eight different metabolic syndrome definitions to the same population and reported that only 2% of children fulfilled all eight metabolic syndrome criteria. 17
Different prevalences for different definitions
There is consensus that (1) the prevalence of metabolic syndrome varies considerably depending on the criteria used, 7,73 (2) that metabolic syndrome prevalence is higher when age-specific criteria are applied to children compared to adult criteria, 16 and (3) that childhood prevalence differs when childhood and adolescent criteria are applied. 54 We were not able to add to the present understanding of how different definitions or cutoff values influenced prevalence because there were only a small number of studies where multiple criteria were applied to the same population. We were able to compare metabolic syndrome prevalence in different populations using different criteria and, although the median prevalence was often similar (Table 2), the range in prevalences varied considerably by criteria used. Although metabolic syndrome prevalence appeared to be highest in studies using WHO criteria, this observation can be at least partly explained by the fact that the majority of studies using the WHO criteria selected only obese populations. The issue of which criterion is “best” remains unresolved, although some advocate use of IDF-based criteria. 75 The systematic use of a single criterion would enhance research efforts into the epidemiology of metabolic syndrome in the paediatric population.
Changing prevalence over time
A rise in metabolic syndrome prevalence might be expected to parallel the increase in childhood obesity prevalence, 6 but there was insufficient evidence to determine whether the prevalence of metabolic syndrome is changing over time. The four studies that used the same definitions for metabolic syndrome in cross-sectional studies at different time points 19,50 –52 were inconsistent for a rise in metabolic syndrome prevalence. The literature describing metabolic syndrome prevalence is relatively new, with the first publication appearing in 2003 and the first data collected in 1988, 76 so any rise in metabolic syndrome prevalence prior to 1988 will be undetected and insufficient time may have passed since 1988 to detect a subsequent rise in metabolic syndrome. Although there are now agreed criteria for diagnosing metabolic syndrome in children, 75 researchers who repeat their cross-sectional studies of metabolic syndrome prevalence could also apply their previous criteria (i.e., ATP III, IDF, or WHO) to their datasets to give longitudinal insight into metabolic syndrome prevalence.
Different prevalence in ethnic groups
Comparison of studies from different countries suggested that metabolic syndrome prevalence may be higher in the Americas and Middle East compared to Europe and the Far East (Table 3). This hypothesis is supported by studies that applied the same criteria to American and South Korea children, 44 Iranian and German children, 62 and Brazilian and Italian children 58 ; for each comparison the metabolic syndrome prevalence was higher in the first ethnic group. Socioeconomic differences between nations and for ethnic groups within a country might be a confounder for metabolic syndrome prevalence (i.e., poverty is associated with increased metabolic syndrome), but there are no data to support this paradigm. In one study, 31 metabolic syndrome prevalence was 2.7% in low-income groups compared to 4.7% in high-income groups and there was no difference in a second study. 77 Although poverty is generally associated with increased obesity prevalence 78 and obesity linked with metabolic syndrome, at present (somewhat surprisingly) there is no evidence to link poverty to metabolic syndrome.
Differences in metabolic syndrome prevalence by gender and age
Metabolic syndrome prevalence was generally higher in boys compared to girls, although this was not a universal finding (Fig. 2). This male preponderance for metabolic syndrome is also seen in adults, although the gender gap may be narrowing in adults. 79 The prevalence of metabolic syndrome increases with age in adults, and we also observed a higher prevalence of metabolic syndrome in older children compared to younger children, although one study 17 found that the relationship between age and metabolic syndrome was only seen in boys and not girls.
Strengths and limitations
The strengths of this review include being the first to review all of the literature, application of a robust methodology, and intrastudy analyses that permitted statistical testing of some differences. The main limitation to any review of this literature is the heterogeneity in criteria used to define metabolic syndrome. A second limitation is the possibility that we have omitted some papers in this relatively large review, and third that papers published since March, 2011, are not included.
Conclusion
Metabolic syndrome appears to be a genuine phenomenon in children and is relatively uncommon among nonobese, nonoverweight children, but is highly prevalent among obese children. The association between obesity and metabolic syndrome is not surprising given that obesity is an essential requirement for IDF criteria for metabolic syndrome and one of the optional requirements for WHO and ATP criteria. However, not all obese children have metabolic syndrome and some nonobese children do have metabolic syndrome 3 ; the inconsistent relationship with obesity and the presence of metabolically obese normal weight and phenotypically obese metabolically normal youths suggests that metabolic syndrome is not simply a consequence of obesity. The clinical relevance of metabolic syndrome in childhood and adolescence remains uncertain because many individuals “lose” their metabolic syndrome, 80,81 but central obesity at 9–10 years is a risk for metabolic syndrome aged 18, 56 suggesting that intervention in early childhood may ameliorate later metabolic syndrome. What is required is a better understanding of metabolic syndrome prevalence and its underlying mechanism. The relevance of family history of metabolic syndrome or diabetes to childhood metabolic syndrome prevalence has not been elucidated. More cross-sectional and longitudinal surveys of children and adolescents are needed to determine the clinical relevance of childhood metabolic syndrome, especially in the United Kingdom where prevalence among obese children is described, 82 but not whole population prevalence.
Footnotes
Acknowledgments
Author contribution: S.T. conceived the idea. S.T., A.F., and L.C. performed the review of papers. S.T. and A.F. wrote a first draft of the manuscript. All authors made meaningful contributions to the final manuscript. S.T. is guarantor for the article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.