
Abstract
Background:
Obese youth demonstrate the same obesity-associated morbidities observed in obese adults, including poor cardiorespiratory fitness, poor quality of life, and reports of musculoskeletal pain. The purposes of this study were to compare the prevalence of cardiovascular risk factors and evaluate the odds of metabolic syndrome in obese youth based on measures of cardiorespiratory fitness, quality of life, and pain.
Methods:
A medical chart review of 183 obese youth in a medical weight management program was conducted. Measures of cardiovascular risk and metabolic syndrome were recorded. Groups were categorized based on Progressive Aerobic Cardiovascular Endurance Run (PACER) score, Pediatric Quality of Life (PedsQL)–Physical Function score, PedsQL–Psychosocial Health score, and reports of musculoskeletal pain. Statistical analysis included independent t-tests, Mann–Whitney U-test, chi-squared test, and logistic regression.
Results:
Thirty-three percent of the entire sample had C-reactive protein (CRP) levels >3.0 mg/dL and 30% were categorized as having metabolic syndrome. Patients with lower PACER scores demonstrated a greater prevalence of CRP levels >3.0 mg/dL versus those with higher PACER scores (45% vs. 12%; P=0.01). There were no other differences in the prevalence of cardiovascular risk factors or metabolic syndrome when categorized by PACER, PedsQL, or pain. Those with CRP levels >3.0 mg/dL demonstrated increased odds of metabolic syndrome—[odds (95% confidence interval, CI): 4.93 (1.24–19.61); P=0.02].
Conclusions:
Overall, results do not show differences in cardiovascular risk in obese youth when categorized by PACER, PedsQL, or reports of MSK pain. Elevated CRP may be a useful predictor of metabolic syndrome in obese youth and warrants further investigation.
Introduction
T
Increased cardiovascular risk is multifactorial. As such, obesity is a component of metabolic syndrome, which is a significant risk factor for cardiovascular disease (CVD) in adults. 5,6 Metabolic syndrome in adults is also associated with other cardiovascular risk factors such as elevated C-reactive protein (CRP) and elevated glycated hemoglobin (HbA1c). 7,8 In both nonobese and obese adults, metabolic syndrome, elevated CRP, and elevated HbA1c have been linked to clinical measures of decreased cardiorespiratory fitness, 9,10 poor health-related quality of life (HRQoL), 11 and complaints of MSK pain. 12,13 While obese youth demonstrate these same obesity-related morbidities observed in obese adults (e.g., metabolic syndrome, MSK pain, decreased cardiorespiratory fitness, poorer HRQoL, etc.), 1 –4 the associations among these factors are not known. Further, cardiovascular risk factors such as metabolic syndrome, elevated CRP, and elevated HbA1c develop over time, and children may be able to compensate for the negative effects of obesity. Better understanding the relationships of other clinical measures of health and function may be useful in identifying obese youth who are at higher risk for CVD.
The purposes of this retrospective study were to: (1) compare the prevalence of CVD risk factors and metabolic syndrome by cardiorespiratory fitness, HRQoL, and reports of MSK pain and (2) evaluate the odds of metabolic syndrome based on common clinical and laboratory measures of health in obese youth. We hypothesized that: (1) CVD risk factors and metabolic syndrome would be more prevalent in obese youth with lower cardiorespiratory fitness scores, lower HRQoL scores, and reports of MSK pain compared to obese youth with higher cardiorespiratory fitness scores, higher HRQoL scores, and no reports of MSK pain; and (2) the odds of metabolic syndrome would be greater in obese youth with lower cardiorespiratory fitness, lower HRQoL, reports of MSK pain, CRP above 3.0 mg/dL, and HbA1c above 5.7% compared to obese youth with higher cardiorespiratory fitness scores, higher HRQoL scores, no reports of MSK pain, CRP levels less than 3.0 mg/dL, and HbA1c levels less than 5.7%.
Methods
For the current study, we used a database of 183 obese youth (ages 9–19 years) who were enrolled in a hospital-based multidisciplinary medical weight management program from 2009–2011. 14 A body mass index (BMI) of equal to or greater than the 95th percentile for age and gender was required to be enrolled in the program. Data for this study are part of a concurrent study examining MSK pain in obese youth, and details regarding the methods have been described previously. 14 This study was approved by the appropriate institutional review boards. Data of interest were extracted from both electronic and paper medical charts specific to the patient's initial visit to the program. Medical charts were excluded from analysis if there was a documented history of orthopedic surgery, neuromuscular disease, inflammatory disease, or chronic arthritis. These factors may contribute to reports of pain and systemic inflammation due to the primary disease state rather than being weight related.
On the basis of the exclusion criteria, eight charts were excluded from further review, leaving 175 medical charts to be included in the final analysis. As previously reported, 14 height, weight, age, sex, and Tanner stage 14 were recorded to describe the sample (Table 1). BMI was calculated and then BMI Z-scores were generated in STATA 12.0 (StataCorp, College Station, TX) using the Centers for Disease Control and Prevention 2002 data. 14,15 Because of the low numbers of Tanner stage I in the sample (n=7), Tanner stages I–II and III–V were categorized as prepubescent and pubescent/postpubescent groups, respectively. 14 Previously reported demographic, anthropometric, cardiorespiratory fitness, and HRQoL results for the entire sample are presented in Table 1. 14
Mean±standard deviation.
Sample size differences as a result of missing data.
BMI, body mass index; PedsQL, Pediatric Quality of Life; PACER, Progressive Aerobic Cardiovascular Endurance Run.
Musculoskeletal pain
Reports of current or recent MSK pain were obtained from a detailed medical problem list and self-report history questionnaire completed by both the participants and parents. For the current analysis, the sample was categorized into two groups—those who reported MSK pain in any location and those with no reports of MSK pain.
Cardiovascular risk factors and metabolic syndrome
As part of clinical evaluation for the medical weight management program, serum blood samples following an overnight fast were obtained. For this analysis, recorded laboratory data included markers of potential cardiovascular risk: High-sensitivity CRP, HbA1c, triglycerides (TGs), high-density lipoprotein (HDL-C), and glucose (GLU). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were also recorded. Cardiovascular risk related to high CRP and HbA1c was defined as levels being above 3.0 mg/dL 16 and 5.7%, 17 respectively. The presence of metabolic syndrome was determined based on the clustering of cardiovascular risk factors determined by the International Diabetes Federation (IDF) Consensus definition for children and adolescents (Table 2). 18 Measures of waist circumference (WC), one of the factors considered in the diagnosis of metabolic syndrome, were limited in our sample (n=62). Instead, a BMI Z-score of 2 was used as a surrogate for central obesity, which has been done in previous work in obese children. 19
BP, blood pressure; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol; GLU, glucose; WC, waist circumference.
Cardiorespiratory Fitness
The Progressive Aerobic Cardiovascular Endurance Run (PACER) score was recorded from the medical chart as a measure of cardiorespiratory fitness (n=146). The PACER is a common valid and reliable tool used to assess aerobic fitness in children and involves running between two lines (20 meters apart) in pace with audible cues. 20 The PACER was multistaged, as the time between the audible cues becomes progressively shorter each minute, thus requiring a progressive increase in running speed as time progresses. The test was discontinued if the participant experienced extreme fatigue or could not maintain the required speed to keep up with the audible cues. The PACER score was recorded from the medical chart as the number of laps completed. 14 Poorer aerobic or cardiovascular fitness align with lower PACER score. 20 The PACER results were dichotomized by median score (12.50) to designate a relative low group and high group within the sample.
Health-related quality of life
HRQoL was recorded from the medical charts using the Pediatric Qualify of Life Inventory 4.0 Generic Scales (PedsQL). The PedsQL is valid a 23-item questionnaire used to assess physical, emotional, social, and school functioning in children aged 2–18 years from which physical function and psychosocial health are determined. 21 The questionnaire uses a five-point Likert response scale for each question, and scores are transformed into a 0–100 scale, with higher scores indicating better well-being. The child report of the PedsQL–Physical Function summary score (PedsQL–Physical) and the PedsQL–Psychosocial Health summary score (PedsQL–Psychosocial) were recorded for analysis from the medical record. PedsQL data were available from 145 medical charts. 14 The PedsQL–Physical and –Psychosocial summary results were dichotomized by median score (81.25 and 75.00, respectively) to designate a relative low group and high group for each subscale within the sample.
Data analysis
Tests for normality were performed on all data and residuals. On the basis of the tests of normality, independent t-tests and Mann–Whitney U-tests were used to evaluate differences in mean levels of potential cardiovascular risk factors between groups as defined by (1) higher or lower PACER scores, (2) higher or lower PedsQL scores, and (3) with and without reported MSK pain. Only subjects for which all data on the risk factors for metabolic syndrome were included in the analysis of prevalence of metabolic syndrome in the sample (n=112). Frequency and chi-squared statistics were used to identify the proportion of participants with (1) cardiovascular risk factors in the total sample, (2) cardiovascular risk factors per group, (3) presence of metabolic syndrome risk factors for the total sample and per group, and (4) presence of metabolic syndrome for the total sample and per group. Finally, two models of logistic regression were used to evaluate the odds of metabolic syndrome based on (1) based on levels of CRP and HbA1c and (2) clinical measures of PACER scores, HRQoL scores, and reports of MSK pain. Age and sex 22,23 were controlled for in all logistic regressions. Significance was set to P=0.05. Statistical analysis was performed with IBM SPSS Statistics version 21 (SPSS Inc., Chicago, IL).
Results
Total sample demographic characteristics, anthropometric measurements, PedsQL summary scores, and mean PACER scores of the participants are presented in Table 1. The number of participants with recorded cardiovascular risk factors was as follows: CRP (n=60), HbA1c (n=116), TGs (n=124), HDL-C (n=124), GLU (n=114), and blood pressure (n=172). Of the cardiovascular risk factors, low HDL-C was the most prevalent (75%) in the total sample, whereas high levels of GLU were the least prevalent (2.6%) (Table 3). Thirty-three percent of the entire sample had high CRP values, indicative of increased systemic inflammation and cardiovascular risk. Approximately 30% of those with metabolic syndrome risk factor data (n=112) were categorized as having metabolic syndrome (Table 3) with a mean of 2.04±0.86 metabolic syndrome risk factors per subject (e.g., blood pressure, TGs, HDL-C, GLU, BMI Z-score). Figure 1 illustrates the distribution of CRP values based on the presence of metabolic syndrome.
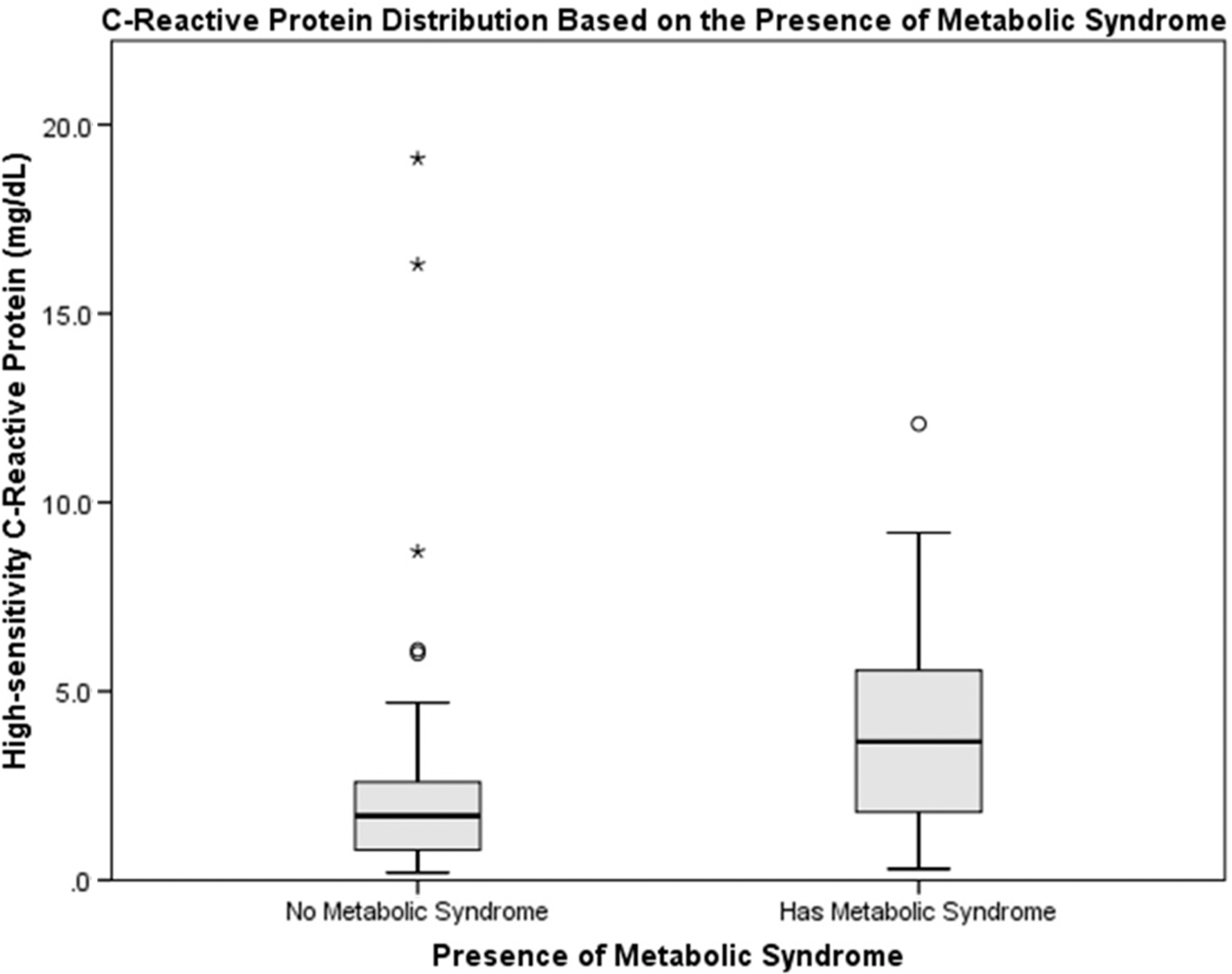
Box plot of C-reactive protein distribution based on the presence of metabolic syndrome. Circles (○) indicate outliers that are 1.5 interquartile ranges away from the 75th percentile. Asterisks (*) indicate outliers that are 3 interquartile ranges away from the 75th percentile.
n (%).
Threshold values for increased cardiovascular risk: blood pressure, systolic ≥130/diastolic ≥85 mmHg; TGs, ≥1.7 mmol/L (≥150 mg/dL); HDL-C, male, <1.03 mmol/L (40 mg/dL), female, <1.29 mmol/L (50 mg/dL); GLU, ≥5.6 mmol/L(100 mg/dL); CRP, >3.0 mg/dL.
HbA1C: ≥ 5.7%
Metabolic syndrome risk factors include: blood pressure, TGs, HDL-C, GLU, and BMI Z-score.
Only participants with complete data for all risk factors of metabolic syndrome were included in the final analysis of regarding metabolic syndrome (n=112).
TGs, triglycerides; HDL-C, high-density lipoprotein cholesterol; GLU, glucose; CRP, C-reactive protein; HbA1c, glycated hemoglobin; BP, blood pressure.
Subject characteristics and mean laboratory values categorized by low/high PACER score, low/high HRQoL scores, and reports of MSK pain are reported in Table 4. A greater percentage of those with lower PACER scores demonstrated CRP values above the threshold for increased cardiovascular risk (45.5% vs. 12%; P=0.01) when compared to the percentage of those with higher PACER scores. However, there were no other differences in the prevalence of cardiovascular risk factors categorized by PACER, HRQoL, or MSK pain (data not shown). There were no differences in the prevalence of metabolic syndrome risk factors or metabolic syndrome classification between groups (data not shown).
n±standard deviation.
Mann–Whitney U-test.
Significance: p=0.05
PACER, Progressive Aerobic Cardiovascular Endurance Run; PedsQL, Pediatric Quality of Life; MSK, musculoskeletal; BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; CRP, C-reactive protein; HbA1c, glycated hemoglobin; BP, blood pressure; TG, triglycerides; GLU, glucose.
After controlling for age and sex, the logistic regression results indicated that those with high CRP demonstrated an increased odds of metabolic syndrome—[odds (95% confidence interval, CI): 4.93 (1.24–19.61); P=0.02] (Table 5). However, PACER scores, PedsQL scores, and reports of MSK pain were not significant predictors of metabolic syndrome (Table 5).
Significance, P=0.05
All results after controlling for age and sex.
CRP, C-reactive protein; HbA1c, glycated hemoglobin; OR, odds ratio; CI, confidence interval; HRQoL, health-related quality of life; MSK, musculoskeletal.
Discussion
Our results demonstrate minimal differences in cardiovascular risk factors between obsese youth with lower PACER scores, lower PedsQL scores, and reports of MSK pain, when compared to those with higher PACER scores, higher PedsQL scores, and no reports of MSK pain, respectively. Controlling for age and sex, these factors did not predict the presence of metabolic syndrome in obese youth. However, obese youth with CRP levels >3.0 mg/dL demonstrated almost five times the odds of metabolic syndrome.
Cardiovascular risk factors and metabolic syndrome
In general, the prevalence of cardiovascular risk factors and metabolic syndrome in our study are similar to others who have evaluated obese youth 24 and extend their findings by evaluating the relationship of metabolic syndrome with clinical measures (PACER, HRQoL, and MSK pain) and markers of inflammation (CRP) and glucose intolerance (HbA1c). Interestingly, when evaluating CRP levels in our study, even though there were no statistically significant differences between groups regarding CRP values (mean±standard deviation), those with lower PACER scores (CRP:4.78±5.37 mg/dL), lower PedsQL–Psychosocial score (CRP:3.45±3.64 mg/dL), and lower PedsQL–Physical score (CRP:3.61±3.88 mg/dL) demonstrated mean CRP values above threshold for increased cardiovascular risk (>3.0 mg/dL), whereas those in the higher groups were consistently below the threshold (Table 4). When divided by PACER scores, the percentage of those with CRP above threshold was greater in those with lower PACER scores compared to those with higher PACER scores (45.5% vs. 12%; P=0.01).
It could be hypothesized that the children and adolescents in our study are just beginning to show signs of chronic inflammation. Perhaps with continued exposure to an obese state from childhood into adulthood, a more definitive difference in mean CRP values would be evident. This is important because in overweight adults, the combination of elevated CRP and HbA1c has been associated with advanced early carotid atherosclerosis progression and the development of metabolic syndrome. 7,8 In addition, several large longitudinal studies in adults demonstrate an additive effect of metabolic syndrome and elevated CRP on the increased risk of cardiovascular events (hazard ratios range, 5.3–5.9) versus having no metabolic syndrome or normal CRP. 5,6 Longitudinal studies evaluating cardiovascular risk and metabolic syndrome present in obese youth from childhood into adulthood are warranted to help to discern the potential negative long-term impact and consequences.
Metabolic syndrome risk
The IDF Consensus Group has recommended that future research regarding metabolic syndrome include evaluating measures of systemic inflammation, including CRP and the risk of developing metabolic syndrome and CVD. 25 In adults, CRP has been shown to be associated with components of metabolic syndrome 26 and has been shown to predict the presence of metabolic syndrome (odds ratio=2.8–4.0). 27,28 Furthermore, adult women who are overweight have shown a higher incidence of metabolic syndrome compared to those who were considered of healthy weight. 27 Several large population-based studies have evaluated the association of metabolic syndrome and its components to levels of CRP in youth. 22,23 In general, results from these studies demonstrate higher levels of CRP in obese youth and youth with metabolic syndrome. However, none of the studies have examined the relationship between CRP and metabolic syndrome in obese youth. Our results extend the findings from these studies by evaluating the relationship between CRP and metabolic syndrome in obese youth and demonstrate for the first time that obese youth with high CRP levels have increased odds of metabolic syndrome. This finding has potential long-term implications because having already elevated levels of CRP as a child may exacerbate and potentiate the negative consequences of metabolic syndrome and CVD in adulthood. 5 –8
HbA1c has been suggested as a potential predictor and surrogate for metabolic syndrome for its utility in assessing long-term glycemic control in adults. 29,30 However, our results do not support the hypothesis that higher levels of HbA1c increase the odds of the presence of metabolic syndrome in obese youth. Poorer cardiorespiratory fitness 31,32 and HRQoL 11 have been shown to be associated with the presence of metabolic syndrome in adults and increased cardiovascular risk factors in children. Yet, our results do not support the hypothesis that poorer outcomes of these variables increase the odds of the presence of metabolic syndrome in obese youth. Our results also do not show an increased odds of metabolic syndrome based on reports of MSK.
Limitations
Authors have used a variety of definitions and criteria to identify metabolic syndrome in both adults and youth. 18,19,22 These differences may yield alternative results when applied to our participants. However, the IDF Criteria for Children and Adolescents 18 used in the current study is a common definition used in current literature. 33,34 This definition is also different than those used in adult populations, and it is not known how it may translate into adulthood. Second, unfortunately not all data were available for all subjects. Incomplete or missing information in the medical charts did not allow for a complete data set for the PACER, PedsQL, and laboratory variables in our analysis. PACER and PEDsQL scores were available for 82% and 83% of our sample, respectively. Reasons for absence of laboratory data included no referral for blood work, patients did not fast overnight, or patients did not receive the blood work for some nondisclosed reason. Further, only 64% of the participants had a complete data set of metabolic syndrome risk factors, 34% had CRP data, and 66% had HbA1c data. However, the prevalence of metabolic syndrome (30.4%) and elevated CRP (33%) is consistent with previous studies [metabolic syndrome, 29.2%; range 10–66%) 24 (CRP, 36%) 22 ]. Third, although PACER and PedsQL scores in obese youth are consistently lower compared to healthy weight youth, 4,35 there are no specific scores indicative of poor PACER or PEDsQL scores in obese youth. Fourth, other factors related to HRQoL (e.g., socioeconomic status, family dynamics) or measures of physical activity (e.g., participation, time, intensity, etc.) were not specifically collected or analyzed as part of this study. Finally, cause and effect of whether CRP predicts metabolic syndrome in obese children cannot be established by the current study. However, our findings do support previous studies indicating that elevated CRP is an important cardiovascular risk factor in obese children. 22,23
Future Research and Clinical Relevance
In our study, categorizing groups by median score may have an effect on the lack of significance between PACER, PedsQL, and MSK groups. Perhaps in a larger sample, categorizing by tertiles would permit a better delineation potential of differences in CRP levels. Second, although not within the scope of this study, our results and others 36,37 may suggest that measures of cardiorespiratory fitness (e.g., PACER score) may be useful in predicting at risk levels of CRP in obese youth. This should be evaluated in future studies. Future research should consider comparing multiple medical weight management programs to ensure generalizability of results. Other measures such of physical activity (e.g., intensity, time, participation, etc.) may also prove useful when evaluating cardiovascular risk. Finally, longitudinal studies should be performed to evaluate the long-term implications of elevated CRP in obese youth into adulthood and predictors of elevated CRP in obese youth, as well as to assess the efficacy of medical weight management programs and their ability to make potential changes to cardiovascular risk in obese youth. Ideally, results would then be used to personalize treatment strategies for program participants based on their cardiovascular profile to ultimately reduce their risk for a future cardiovascular event.
Conclusion
Our results provide a descriptive representation and comparison of cardiovascular risk factors related to metabolic syndrome in obese youth enrolled in a hospital-based medical weight management program. Overall, the prevalence of cardiovascular risk factors and metabolic syndrome in our sample is consistent with previous reports in the literature. Our results do not show differences in cardiovascular risk in obese children enrolled in a medical weight management program when categorized by cardiorespiratory fitness, HRQoL measures, or reports of MSK pain. Elevated CRP may be a useful predictor of metabolic syndrome in obese youth and warrants further investigation. Furthermore, the potential long-term impact of the presence of metabolic syndrome and elevated CRP in obese youth on CVD in adulthood should be evaluated.
Footnotes
Acknowledgments
We would like to thank the Center for Healthy Weight and Nutrition at Nationwide Children's Hospital for assisting in the data collection process and all of the patients who were included in this study.
Dr. Matthew Briggs is employed by OSU Sports Medicine and received funding from The Ohio State University Graduate School's Alumni Grant for Graduate Research and Scholarship to support this project. Dr. Sharon Bout-Tabaku is employed by Nationwide Children's Hospital and received funding from the Arthritis Foundation Clinical to Research Transition Award to partially support this project. Dr. Briggs reports grants from The Ohio State University Graduate School Alumni Grant for Graduate Research and Scholarship, during the conduct of the study. Dr. Bout-Tabaku reports support from the Arthritis Foundation Clinical to Research Transition Award during the conduct of the study.
Author Disclosure Statement
No competing financial interests exist.