
Abstract
Background:
We compared the early endocrine and metabolic changes associated with sleeve gastrectomy (SG) and gastric bypass (GB) in grade III obese patients.
Methods:
Fifty morbidly obese patients were randomized into two groups on the basis of their position in the queue—group A comprised SG and group B was GB. Comparison between the two groups was based on clinical and laboratory variables such as fasting blood glucose, insulin, homeostasis model assessment of insulin resistance (HOMA-IR), glycated hemoglobin (HbA1c), lipids, albumin, and ferritin. Patients were assessed after 7, 14, 30, 60, and 90 days and additional laboratory tests were done on the 90th day.
Results:
The following mean values were recorded for groups A and B, respectively: Age (years), 36.4 and 31.1; weight (kg), 123.2 and 128.3; and body mass index (BMI; kg/m2), 45.6 and 47.3. In the first postoperative week, group B showed a greater weight loss (P=0.047) that was not observed after 14, 30, 60, and 90 days (P>0.05). Group A had an average excess weight loss of 31.09 kg compared to 32.69 kg in group B (P=0.222). Glycemic control was better in group B (P=0.023), whereas the control of systemic arterial pressure was better in group A (P=0.026). There were no significant differences in early lipid control and micronutrient deficiencies between the two groups.
Conclusions:
SG and GB were equally effective in promoting weight loss after 90 days. However, whereas SG was associated with better early remission rates for hypertension, GB was more effective in fasting blood glucose control but not in HOMA-IR and HbA1c levels. There was no difference in the protein or vitamin deficiencies of the two groups.
Introduction
I
Among the bariatric and metabolic surgeries used to treat obese patients, gastric bypass (GB) is currently the most commonly performed by surgeons around the world. 5 GB is a mixed surgery that involves a restrictive component, characterized by a new gastric pouch of ∼30 mL, associated with a malabsorptive component corresponding to ∼2 meters of the small bowel. Among the various mechanisms of metabolic surgery, the most important metabolic effect of GB is gastric and duodenal exclusion of the gastrointestinal transit and promotion of the arrival of undigested food earlier in the terminal ileum (incretin effect). 6
Sleeve gastrectomy (SG) has been gaining popularity among surgeons worldwide, and its frequency may reach that of GB in a few years. This procedure is rapidly becoming the favorite of many surgeons, although there are some questions regarding its efficacy. 7 SG is a purely restrictive surgery during which much of the stomach is removed while preserving the pylorus; there is no malabsorption. SG retains the normal transit time of the digestive tract, reduces the risk of dumping syndrome, and allows normal absorption of nutrients, vitamins, minerals, and drugs. Theoretically, this should avoid the metabolic effect (incretin) and result in lower rates of malnutrition. 8,9 Because SG does not exclude the stomach and duodenum, its metabolic effect has been questioned. However, some studies have concluded that the long-term endocrine and metabolic effects of GB and SB are similar. 10,11
On the basis of our experience and the monitoring of medical practice, we have observed that many obese patients show a reduction in metabolic syndrome or even interrupt the regular use of medication in the initial days after either type of surgery, regardless of the amount of weight loss. For this reason, we designed a randomized clinical trial to compare the early changes in endocrine–metabolic parameters associated with SG and GB, particularly with regard to the early remission of co-morbidities before significant weight loss.
Methods
Study design
This was a randomized clinical trial designed to evaluate the metabolic effects of two different techniques of bariatric surgery (with or without duodenal exclusion) in the early remission of co-morbidities related to grade III morbidly obese patients with inadequate medical control. This study was done in the Department of Bariatric Surgery at Andaraí Federal Hospital run by the Ministry of Health in Rio de Janeiro, RJ, Brazil. The study was approved by the Ethics and Research Committee of Fluminense Federal University (protocol number 363.683). Clinical Trials.Gov Identifier: NCT02394353
Patient selection and randomization
Fifty-nine patients with a diagnosis of grade III morbid obesity were selected to participate in this study on the basis of the following inclusion criteria: Body mass index (BMI) ≥40 kg/m2 (grade III) and age between 18 and 65 years old. The exclusion criteria were: Age <18 years or >65 years old, chronic disease (heart failure, chronic liver disease), alcohol abuse (abuse was defined as the consumption of >14 drinks per week), and the presence of diseases that contraindicated one of the techniques, e.g., human immunodeficiency virus (HIV) patients should not undergo a disabsorptive procedure such as GB and obese individuals with severe gastroesophageal reflux should not undergo SG.
All patients in this study were from the public health system in the State of Rio de Janeiro, Brazil. The patients had a “key number” through which they were registered in a local, state-run regulatory system. Because this registration was on-line, the computer system periodically sent a “key number” automatically to the federal hospital, and this number was used to call in the corresponding patient. Hence, the patient “next in line” was determined by an independent system run by the State Department of Health and forwarded to us in the federal hospital (tertiary center). This approach ensured random allocation of the patients to the groups. The first “key number” was allocated in to group A, the next to group B and so on. To determine the procedure to each group, we picked out by lot group A for SG and group B for GB. Because the “key number” was sent to us by another system, we assumed that the number allocation by the system was random. We randomized the patients on the basis of their position in the queue—one patient to group A and the next in line to group B. Four patients were excluded because they started micronutrients on their own before the 90th postoperative day. Three patients were excluded because of contraindications to the procedure proposed by randomization (all of these patients had severe reflux disease and erosive esophagitis that, in our view, contraindicated the SG). One patient refused to participate and another did not complete the 90-day follow-up (Fig. 1). In all, 50 patients were randomized into two groups—group A, SG (n=25), and group B, GB (n=25).
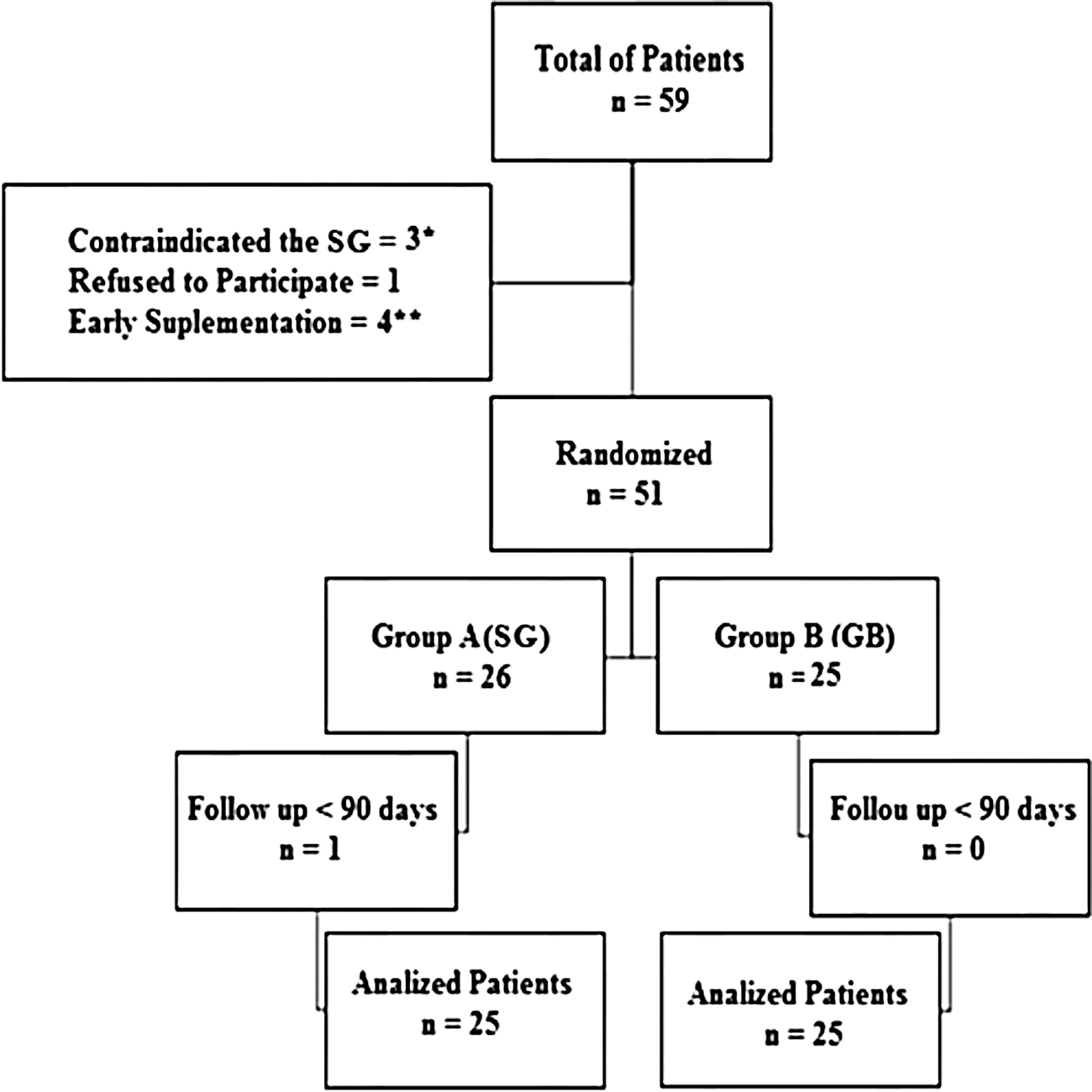
Selection of patients and random allocation to groups. (*) Three patients had severe esophagitis with erosions that, in our view, contraindicated the sleeve gastrectomy (SG). (**) Four patients undertook supplementation on their own before 90 days postsurgery.
Parameters measured
The same surgeon collected all anthropometric variables, including weight, height (measured with Welm® scales), and BMI. The ideal weight (IW) was calculated using the Lorentz formula: [(Height−100)−(Height−150)]÷K, where K is 4 for men and 2 for women. 12 Overweight was calculated as the weight of the patient minus the IW. This allowed calculation of the excess weight loss (EWL) on the 90th postoperative day (EWL90)=(weight loss90÷overweight)×100. All patients were evaluated by our multidisciplinary team (consisting of a nutritionist, psychologist, endocrinologist, and cardiologist) and underwent surgery only after documented evidence of the failure of medical treatment for at least 1 year. Blood samples were collected 1 day prior to surgery at the hospital, after a 12-hr fast, and were screened for total cholesterol, triglycerides (TGs), hemoglobin, iron, ferritin, vitamin B12, folic acid, albumin, uric acid, fasting blood glucose (FBG), glycated hemoglobin (HbA1c), insulin, and the homeostasis model assessment of insulin resistance (HOMA-IR). The HOMA-IR was calculated using the formula: (FBG×0.0555×insulin)÷22.5, with normal values ≤3.40.
Intervention study
All surgeries were done laparoscopically and always by the same surgeon, with standardization of the procedures associated with each technique. For group A (SG) we used a French 32 (32 Fr) orogastric tube. The first shooting started 4 cm from the pylorus with a green load of 45 mm, followed by seven additional shots with a blue load of 45 mm in the direction to the angle of His. At the end of the procedure, the Methylene Blue test was done to assess impermeability of the staple line and to measure the volume of the new gastric pouch (70–80 mL). In group B (GB), we produced a gastric pouch (∼30 mL) with four shots of a blue load of 45 mm. The biliopancreatic limb was 80 cm and the alimentary limb was 120 cm. A 32 Fr orogastric tube was used to perform the gastrojejunal anastomosis and guarantee a calibrated anastomosis of 1.8 cm. An abdominal drain was placed in all patients to monitor the blood loss.
All patients started a fractionated liquid diet on the day after surgery and were discharged on the second postoperative day without any protein or micronutrient supplementation. The follow-up on postoperative days 7, 14, 30, 60, and 90 was done in the hospital, always by the same professional. At each visit, the patient's weight, height and BMI were determined. On the 90th postoperative day, additional blood samples were collected and analyzed as described above to allow comparison with the preoperative values in each group.
Outcome variables
The primary outcome was glycemic control 90 days after surgery. The control was satisfactory in patients with FBG<126 mg/dL (<0.0555 mmol/L) and associated with HbA1c<6.5% without the use of oral hypoglycemic agents or insulin. 13 The secondary end points were the EWL90, a fall in HbA1c, systolic blood pressure (SBP), diastolic blood pressure (DBP), 14 and lipid profile, 15 and changes in hemoglobin, iron, ferritin, vitamin B12, folic acid, albumin, and uric acid.
Statistical analysis
All results were expressed as the mean, minimum, and maximum values. Continuous variables were compared between the two groups using the Mann–Whitney U-test. Differences in the proportions of the variables within the groups were assessed using the Fisher exact test. The Student t-test was used to compare the baseline values of the parameters between groups. All analyses were done using SPSS IMB® Statistics® software, version 20.0.0, with P<0.05 indicating significance.
Results
Characteristics of patients
We evaluated 50 patients (46 women, 92%; four men, 8%, with two men in each group). The mean age of group A was 38.24 years (range, 24–56 years), whereas that of group B was 35.20 years (range, 19–53 years) (P=0.297). The mean weight of group A was 123.22 kg (range, 98.9–177.0 kg) and that of group B was 128.27 kg (range, 93.6–170.8 kg) (P=0.391). For BMI, the mean for group A was 45.62 kg/m2 (range, 40–67.4) and that for group B was 49.24 kg/m2 (range, 40.4–69.6) (P=0.085). There was no significant difference in the proportion or in severity of patients with a particular co-morbidity (P>0.05 for all co-morbidities) after randomization. All procedures were done by laparoscopy, with no clinical or surgical complications. We did not have any major accident in the 50 procedures (bleeding). We also measured blood loss during postoperative time by looking at the silicone drain placed in all procedures (SG and GB). We routinely keep this device for 7 days postoperatively. It allows us to observe the blood lost. All patients returned with less than one reservoir of fluids (less than 125 mL).
The mean operative time for SG was 64.5 min (range, 48–125 min) whereas that for GB was 98 min (range, 61–150 min) (P<0.001).
Comparison between groups
The weight loss curve was significant in both groups (Fig. 2). However, there was no significant difference in the EWL90 of the two groups (Fig. 3). In the first postoperative week, group B had a greater weight loss compared to group A (P=0.047), but this difference was not maintained on days 14, 30, 60, and 90 (P=0.562, P=0.457, and P=0.746, respectively). The mean EWL90 in group A (30.6%; range, 12.8–50.9%) was not significantly different from that of group B (33.3%; range, 13.9–55.3%) (P=0.222).
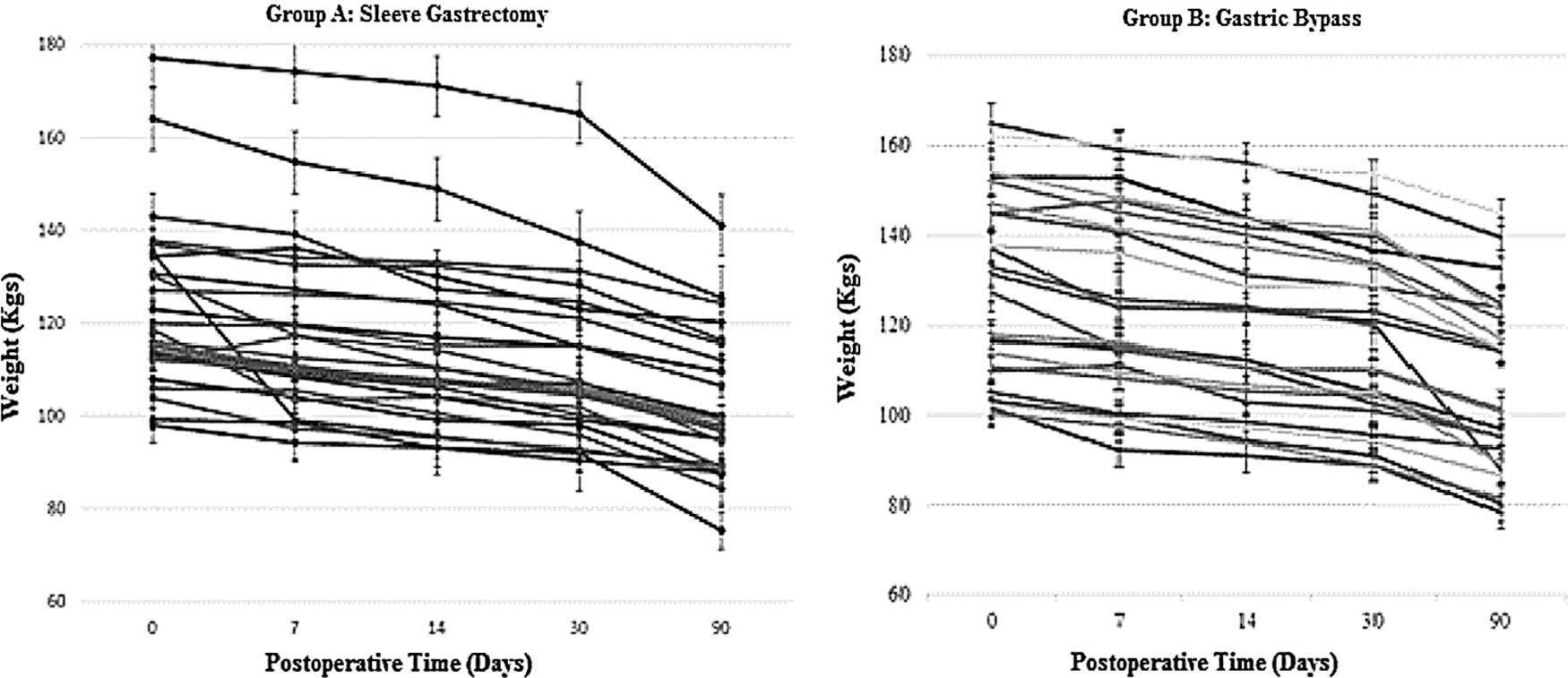
Weight loss curve. Group B showed a greater weight loss than group A 7 days after surgery (P=0.047), but there were no significant differences between the groups on days 14, 30, and 90 (P=0.562, P=0.457, and P=0.746, respectively).

Analysis of excess weight loss the 90th postoperative day (EWL90). There was no significant difference between the groups (P=0.222).
Table 1 shows the remission of co-morbidities. Ninety days after surgery, the rate of improvement in glycemic control was higher in group B compared to group A (P=0.023). In contrast, blood pressure control was higher in group A (P=0.026). There was no difference in the lipid profile of the two groups (P>0.05).
Glycemic control: glucose <126 mg/dL and HbA1c <6.5% without oral medication and/or insulin. Hypertension: systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg and/or use of antihypertensive medication. Altered levels: cholesterol >200 mg/dL, low-density lipoprotein cholesterol (LDL-C) >160 mg/dL, triglycerides (TGs) >150 mg/dL, high-density lipoprotein cholesterol (HDL-C) <40 mg/dL for men and <50 mg/dL for women.
Table 2 shows the results of the laboratory analysis. Iron and magnesium deficiencies were the most common deficits in the preoperative period [32% (8/25) and 28% (7/25), respectively]. None of the patients had pre- or postoperative folic acid deficiency. FBG was controlled better in group B (P=0.034), but there were no significant differences between the groups in any of the other variables. None of the patients showed signs or symptoms of calorie, protein or vitamin deficiency in the 90-day postoperative period.
For all comparisons, the P value was >0.05, except for FBG (P=0.034). Reference values were: FBG <126 mg/dL, HbA1c <6.5%, HOMA-IR >3.4, hemoglobin >13.5% for men and >12.5% for women, iron >60 mg%, ferritin >15 ng/mL, folic acid >3.0 ng/mL, vitamin B12 >200 pg/dL, calcium 8.5–10.5 mg/dL, magnesium 1.9–2.8 mg/dL, albumin >3 grams/dL, uric acid 2.4–5.7 mg/dL for women and 3.4–7.0 mg/dL for men. All of the changes in hemoglobin, iron, ferritin, folic acid, vitamin B12, calcium, magnesium, and albumin were considered as lower than the reference values, whereas all of the changes in blood glucose, HbA1c, HOMA-IR, and uric acid were considered higher than the reference values.
FBG, fasting blood glucose; HbA1c, glycated hemoglobin; HOMA-IR, homeostasis model assessment of insulin resistance.
Table 3 compares the presurgical baseline values and the postoperative values (90 days postsurgery) of the two groups. After randomization, there were no significant differences in the severity of the co-morbidities between groups A and B. However, 90 days after surgery, there were significant differences in FBG (P=0.015) and DBP (P=0.032), and a marginally significant difference in SBP (P=0.058).
The Student t-test was used to compare the two groups, with P<0.05 indicating significance.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; HbA1c, glycated hemoglobin; HOMA-IR, homeostasis model assessment of insulin resistance; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TGs, triglycerides.
Discussion
Bariatric surgery is currently more effective than medical therapy for treating morbid obesity. Of the two surgical procedures currently widely used (GB and SG), the latter is the most recent and has been questioned with regard to its short- and long-term efficacy. Unlike SG, the mechanisms by which GB leads to weight loss and optimizes co-morbidities have been extensively studied and are reasonably well understood. 6,10 The volume restriction promoted by decreasing the gastric pouch leads to early satiety, 16 whereas bypass of the excluded stomach inhibits the release of orexigenic hormones 16,17 and the presence of undigested food in the terminal ileum triggers the so-called incretin effect. 18 These mechanisms explain the early improvement in some aspects of the metabolic syndrome, independent of significant weight loss.
By definition, SG is a restrictive bariatric surgical procedure because there are no deviations of the gastrointestinal transit and undigested food does not arrive quickly in the terminal ileum. Does SG also provide early metabolic optimization of the patient before there is a significant weight loss? To address this question, it should be recalled that SG accelerates gastrointestinal transit through rapid gastric emptying and therefore may well trigger the incretin effect. 10 Furthermore, most of the ghrelin produced in the stomach fundus is completely removed during SG, which means that this procedure is also a metabolic surgery. 7 Our study did not investigate the biochemical and hormonal effects of each technique, but rather sought to identify possible differences in the early remission of metabolic disorders in the patients before weight loss.
In a randomized, double-blind clinical trial with 60 patients, Lee et al. 11 compared the effects of SG and GB in grade I obese patients. Even though these authors were dealing with patients who were less obese than those of the present study, it is interesting to note that there were no differences in the weight loss associated with each surgical procedure 1 and 3 months after surgery (P=0.85 and P=0.1, respectively). However, patients who underwent SG showed greater weight loss at 6 and 12 months (P=0.03 and P=0.02, respectively). Kehagias et al. 19 observed that in the first months, SG leads to a greater EWL than GB, whereas 3 years after surgery the losses were similar (62% and 68% for GB and SG, respectively; P=0.13).
A large randomized clinical trial undertaken by Schauer et al. 2 evaluated 150 patients with a 12-month follow-up. Although there was no description of the early results, these authors observed greater weight loss in GB compared to SG and to patients on medication (P<0.001 for both). Although we did not study patients on medication, we nevertheless identified a significant difference in the EWL among the groups at 1 and 3 months (P=0.222), in agreement with Lee et al. 11 However, our GB group showed greater weight loss in the first week (P=0.047), possibly because of greater sequestration of intestinal fluid in the initial days after the bypass; the latter phenomenon could lead to a higher incidence of dumping syndrome and greater early weight loss.
Bayham et al. 20 described the retrospective analysis of a cohort of 38 patients with GB and 71 with SG, with both groups being studied up to the 60th postoperative day. Approximately 79% of patients with GB and 83% of those with SG were not on medication for diabetes in this period. In our prospective cohort that extended up to the 90th postoperative day, the number of patients free of medication for diabetes was higher in the GB group (from 72% to 12%) than in SG group (from 84% to 60%) (P=0.023).
In the same cohort, Schauer et al. 2 observed an improvement in glycemic control after 12 months in the three groups studied (GB, SG, and medication), with a mean HbA1c of 7.5 in the group on medication compared to 6.4 in the GB group (P<0.001) and 6.6 in the SG group (P=0.003). However, Lee et al. 11 observed a significantly greater improvement with GB (mean decrease of 3.0% in HbA1c) compared to SG (mean decrease of 4.2%) from the first month after the procedure onward (assessed after 1, 3, 6, and 12 months) (P<0.05 for all periods studied). In our series of patients, there was no significant difference in the decrease in HbA1c between the two groups (P=0.407 0.267) during the 90 days of the study.
A recent report 3 based on 3 years of monitoring the same patients studied in the original cohort of Schauer et al. 2 showed that, at the end of this period, the frequency of patients that achieved the desired goal for the treatment of diabetes continued to be best in the GB group (P=0.01). However, 3 years after surgery, when the EWL had reached >60%, it was difficult to precisely define which factor, i.e., the metabolic effect of the technique or the simple loss of excess weight per se, had been most important in reaching this goal.
In a cross-sectional study of individuals already operated, Jiménez et al. 21 compared SG and GB patients at different postoperative intervals. When subjected to a standardized liquid meal, GB patients showed a faster increase in FBG levels compared to patients with SG (88.2% and 42.9% of patients, respectively, attained an FBG peak >180 mg/dL; P<0.05). Interestingly, this report also showed that despite this faster increase there were no differences between the two groups in relation to the overall FBG (P=0.865), HOMA-IR (P=0.902), and HbA1c (P=0.722). This finding suggests that both techniques caused rapid improvement in metabolic control, but by different physiopathological mechanisms. In our study, at a given postoperative time, the proportion of patients with normal FBG levels was greater in the GB group (P=0.034), but there were no differences for HOMA-IR (P=0.327) and HbA1c (P=0.476).
We observed better resolution of hypertension in the first 90 days in SG patients compared to GB patients (P=0.026). Kehagias et al. 19 also reported better rates in the SG group and found no significant difference between the same groups of patients after a 3-year follow-up (P=0.05). On the basis of a systematic review of randomized clinical trials involving 6526 patients, Li et al. 22 reported better control of hypertension in GB patients compared to SG patients.
Woelnerhanssen et al. 23 analyzed the early changes and the effects of adiponectin and lipid metabolism in 12 GB patients and 11 SG patients. Both groups showed a significant reduction in adiponectin levels and adiponectin/kg (P<0.001 for GB and P<0.05 for SG) in the initial weeks after surgery, but there was no difference between groups. There was a significant improvement in the lipid profile with both techniques (P<0.05), but no difference in the responses between the two groups during the first year after surgery (P>0.05). However, in the first week after surgery, the SG group already showed a significant decrease in TGs levels compared to preoperative levels (P<0.05). Although we did not examine adiponectin levels, there was nevertheless a significant decrease in the levels of total cholesterol, low-density lipoprotein cholesterol (LDL-C), and TGs in both groups, but no early difference between them at 90 days after surgery (P>0.05).
Anemia has been a fairly common finding in bariatric patients, 24 although up to 1.5% of patients already have an iron deficiency in the preoperative state. 25 Rutz et al. 26 observed that even with a daily routine supplementation of 3.9 mg of iron in the first days after surgery there was a failure rate of 9% at 6 months and 38% at 18 months postsurgery in patients with GB. However, these authors did not assess patients with SG. In a paper titled “The gastric sleeve: Losing weight as fast as micronutrients?” based on a retrospective analysis of 60 patients undergoing SG, Aarts et al. 27 criticized this technique for the micronutrient deficit it caused; however, their study did not include a GB group for comparison. In a manner similar to Rutz et al., 26 these authors evaluated the responses during the first 6 months after surgery and observed a rate of 26% for anemia, 43% for iron deficiency, 15% for folic acid deficiency, and 9% for low vitamin B12. We also observed a high rate of iron deficiency (32%) preoperatively in both groups, but no patient was deficient in folic acid or suffered from protein malnutrition. The high rate of preoperative iron deficiency seen in the present study may reflect the rigorous screening that we applied to our patients, who were recruited from a public hospital. There were no significant micronutrient differences between the groups during the study, and we do not routinely initiate early micronutrient supplementation, primarily because of the comprehensive clinical surveillance that our patients undergo during the initial weeks after surgery.
Kehagias et al. 19 reported a randomized clinical trial in which they compared 60 morbidly obese patients (BMI <50 kg/m2) who underwent GB (n=30) and SG (n=30). The primary end points were weight loss and the incidence of micronutrient malnutrition. After a 3-year follow-up, there was no difference in micronutrient deficiency between the groups, except for vitamin B12, for which low levels were more common in the GB group (P=0.05). However, in this study, short-term deficiencies were not evaluated.
Compared to GB, SG is a relatively new procedure that is still undergoing acceptance by surgeons as an independent technique, even though it has historically been part of the duodenal switch procedure. Our group has had excellent results with SG and great acceptance by the patients. However, SG-associated complications, e.g., fistula of the angle of His, can be challenging to treat. Indeed, this particular complication can lead some surgeons to not choose this technique as the gold standard.
The major limitation of our study was the lack of measurement of intestinal hormones. Without data on the intestinal levels of hormones such as ghrelin, gastric inhibitory polypeptide (GIP), glucagon-like peptide 1 (GLP-1), and peptide YY (PYY), it is impossible to assess the onset of the early metabolic effects of each technique or to evaluate the mechanisms that optimize the associated co-morbidities. Another limitation was the lack of a control group on medication that would have facilitated investigation of the underlying physiopathological and biochemical mechanisms. Clinical studies in which these aspects are incorporated into the study design will be useful in addressing the biochemical and hormonal mechanisms of the early changes associated with each type of surgery. Studies with early changes have the limitation of long-term outcomes. However, they are important to clarify the possibility of any others mechanisms to improve the co-morbidities that are independent of weight lost. In addition, these metabolic and endocrine mechanisms probably are different between GB and SG.
Conclusions
Evaluation of the early changes associated with SG and GB showed that both techniques were equally safe and effective in causing weight loss in morbidly obese patients. Whereas SG was associated with early-improved resolution of hypertension, GB was more effective in FBG control but not in HOMA-IR and HbA1c levels. There was no significant difference in the micronutrient deficit with either procedure.
Footnotes
Acknowledgments
There was no specific funding for this work.
We thank all of the patients who participated in this study and the multidisciplinary team of the Department of Bariatric Surgery at Andaraí Federal Hospital. Fernando de Barros is grateful to postgraduate supervisor Prof. Sérgio Setúbal and co-supervisor Prof. José Manuel Martinho.
Author Disclosure Statement
No competing financial interests exist.