
Abstract
Background:
It is still uncertain whether food insecurity increases the risk of metabolic syndrome. Recent reports from the United States and developing countries have shown conflicting results on this issue. This study aimed to investigate the association between food security status and metabolic syndrome in Korean adults.
Methods:
We performed a nationwide population study using data for 18,782 adults obtained from the 2012 to 2015 Korean National Health and Nutrition Examination Surveys. The 18-item Food Security Survey Module was utilized to assess household food security status. We used multiple logistic regression models to determine the association between food security status and metabolic syndrome.
Results:
The overall prevalence of food insecurity was 8.2% and that of metabolic syndrome was 27.3%. The prevalences of metabolic syndrome were 26.2%, 32.3%, 30.2%, and 28.8% in the high, marginal, low, and very low food security groups, respectively. Food-insecure participants (participants in the low food security and very low food security groups) were significantly more likely to be female, divorced/widowed/separated, and current smokers compared to food-secure participants. Food-insecure participants also had lower incomes, lower education attainments, and lower physical activities (P < 0.05). Compared with the high food security group, the marginal (odds ratio [OR]: 1.34, 95% confidence interval [95% CI]: 1.19–1.50, P < 0.001) and low food security groups (OR: 1.22, 95% CI: 1.04–1.42, P = 0.01) had increased odds of metabolic syndrome in the unadjusted models. However, after controlling for covariates, including age, sex, marital status, education attainment, household income, smoking, alcohol intake, and physical activity, neither marginal food security (adjusted odds ratio [aOR]: 1.02, 95% CI: 0.87–1.19, P = 0.86) nor low food security (aOR: 0.88, 95% CI: 0.71–1.08, P = 0.22) was significantly associated with an increased risk of metabolic syndrome.
Conclusions:
Contrary to a prior report from the United States, food security status was not significantly associated with the risk of metabolic syndrome in Korean adults.
Introduction
Metabolic syndrome is a cluster of metabolic risk factors that increases the risk of heart disease, stroke, and type 2 diabetes mellitus. 1 Components of metabolic syndrome include raised blood pressure, atherogenic dyslipidemia (raised triglycerides and lowered high-density lipoprotein cholesterol), raised fasting glucose, and central obesity. Most expert groups have defined metabolic syndrome as the presence of three or more risk factors. 2 –4
The prevalence of metabolic syndrome has been rising worldwide in both high-income and low-income countries. 5 In Korea, a recent report has indicated that the age-adjusted prevalence of metabolic syndrome has also substantially increased over the last two decades. 6 Given the robust impact of metabolic syndrome on the occurrences of cardiovascular disease and type 2 diabetes, the early identification of metabolic syndrome and the reinforcement of various measures that could reduce the risk of cardiovascular disease, including lifestyle modification and drug therapy for hypertension, dyslipidemia, and diabetes mellitus, are important public health issues.
Food insecurity is a state of limited or uncertain availability of nutritionally adequate and safe foods. 7 A food insecure state not only refers to the status of having insufficient quantity of food but also refers to the state of having inadequate quality of food. Prior investigations have shown that food insecurity can be associated with increased risks of obesity, 8,9 diabetes mellitus, 10 dyslipidemia, 11 –13 hypertension, 11 and metabolic syndrome. 14 It has been postulated that individuals living in food-insecure households tend to buy cheaper, calorie-dense foods of low nutritional value, the consumption of which might lead to metabolic abnormalities. 14,15 Since food insecurity can be modified by intervention or economic support, the clarification of the association between food insecurity and metabolic syndrome can assist in the prevention and management of metabolic syndrome. However, it should be noted that most of those data were from Western countries and that only one study, performed more than a decade ago in the United States, showed that food security status was significantly associated with an increased risk of metabolic syndrome. 14
Recent large-scale studies conducted in the United States showed that food insecurity could be associated with multiple chronic conditions, including cardiac diseases, hypertension, diabetes, and stroke. 16,17 In contrast, a Malaysian group reported that reproductive-aged women in food-insecure households in low-income communities of Malaysia were less likely to suffer from metabolic syndrome. 18 Conversely, a smaller-scale Iranian study showed no significant differences in metabolic syndrome prevalence between food-secure and food-insecure groups. 19 These findings suggest that the association between food security status and metabolic syndrome can differ according to regional, cultural, and socioeconomic characteristics. Therefore, the objective of this study was to investigate the association between food security status and metabolic syndrome in Korean adults using nationwide population-based data.
Methods
Design and study population
We performed a cross-sectional analysis using nationwide population-based data from the Korean National Health and Nutrition Examination Surveys (KNHANES) conducted by the Korea Centers for Disease Control and Prevention (KCDC). The KNHANES is a stratified multistage probability sampling design study to survey the health and nutrition status of the noninstitutionalized civilian Korean population. Components of KNHANES include a face-to-face interview, health examination, and nutrition survey. Since 18-item food insecurity questionnaire (see below Food Security Status section) was used between 2012 and 2015, data of 2012–2015 KNHANES were combined following the instructions provided by the KCDC. The KNHANES was approved by the Institutional Review Board of the KCDC. Written informed consent was obtained from all participants. Only publicly available data on the KCDC Website were used.
Figure 1 shows the selection process of the study population. Among 24,327 adult participants aged 19 years or older, participants with missing data for household food security (n = 1901), pregnant women (n = 103), and those with missing data for metabolic syndrome components (n = 3541) were excluded. The final analytic sample consisted of 18,782 adults.
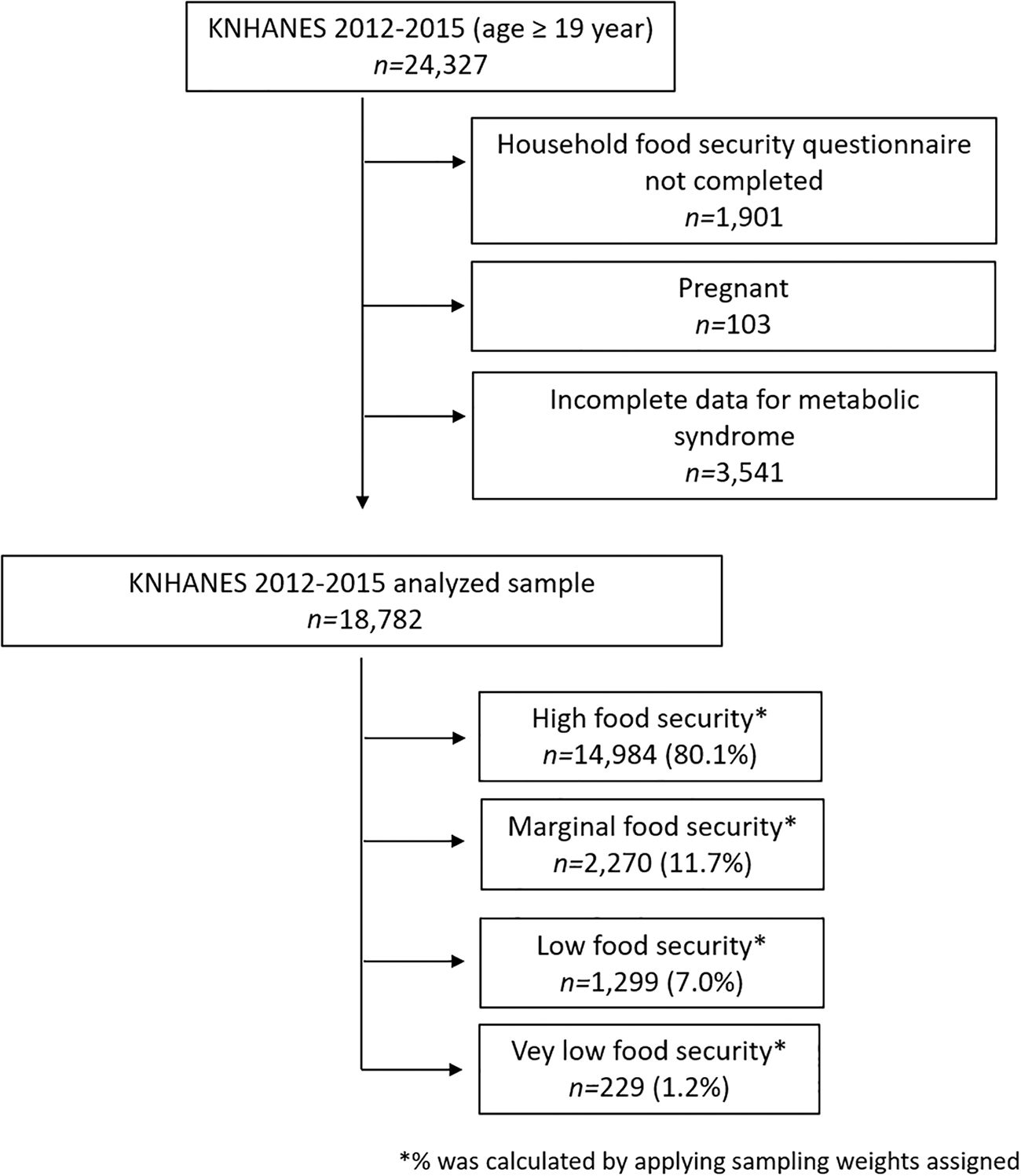
Enrollment process for adults with reasons for exclusion.
Measures
Food security status
An 18-item food insecurity questionnaire modified from the U.S. Household Food Security Survey Module (HFSSM) was utilized to assess food security status at the household level. 20 The U.S. HFSSM contained an 18-item questionnaire about a household's food security status in the last 12 months. These questions assessed the existence, frequency, and severity of food insecurity-related events in a household. Ten of these 18 questions were for all households, whereas 8 were for households with children. This survey has been found to be a valid and reliable instrument for the Korean population. 20 According to the calculated food security scores, food security statuses were categorized into four groups: high food security (raw score: 0), marginal food security (raw score: 1–2), low food security (raw score: 3–7 for households with one or more children and 3–5 for households without children), and very low food security (raw score: 8–18 for households with one or more children and 6–10 for households without children). Households with low or very low food security were considered to have food insecurity.
Metabolic syndrome
The modified National Cholesterol Education Program-Adult Treatment Panel III (NCEP ATP III) criteria for metabolic syndrome were used in this study. 21 Metabolic syndrome was diagnosed as the presence of three or more out of the following five criteria: (i) central obesity (waist circumference: ≥90 cm in men and ≥80 cm in women); (ii) hypertriglyceridemia (triglycerides ≥150 mg/dL); (iii) reduced high-density lipoprotein cholesterol (<40 mg/dL in men and <50 mg/dL in women); (iv) hypertension (blood pressure ≥130/85 mmHg or antihypertensive medication); and (v) hyperglycemia (fasting blood glucose ≥100 mg/dL or antidiabetic medications).
Covariates
Confounding covariates included sex, age, marital status, education attainment, household income, smoking, alcohol intake, and physical activity. Age was categorized into three groups: 19–39 years, 40–59 years (reference group), and more than 60 years. Marital status was into three categories: never married, married (reference group), or divorced/widowed/separated. Participant's education was categorized into less than or equal to elementary school, middle school, high school, and greater than or equal to college education (reference group). Household income was categorized by quartiles: lowest, lower-middle, upper-middle, or highest (reference group). Smoking status was categorized as current, past, and never smoker (reference group). Alcohol intake was categorized into heavy (≥7 glasses for men or ≥5 glasses for women on at least 2 occasions weekly), moderate, and none (reference group). Physical activity was classified as regular (vigorous exercise >4 times/week; reference group), intermittent (vigorous exercise 1–3 times/week), and none. Body mass index (BMI) (kg/m2) was calculated as weight (kg)/height (m2). Participants were categorized into underweight (BMI <18.5 kg/m2), normal weight (18.5–24.9 kg/m2), and overweight (≥25.0 kg/m2) groups.
Statistical analyses
Survey sampling weights were applied in all analyses to produce estimates that could be representative of the total Korean population. Data are presented as a weighted percentage with a standard error for categorical variables or as mean with a standard error for continuous variables. Differences between categorical and continuous variables across food security categories were tested using the Rao-Scott chi-squared test and one-way analysis of variance (ANOVA) with Duncan's multiple range test, respectively. Multiple logistic regression analyses were carried out to calculate the odds ratio (OR) and 95% confidence interval (95% CI) for metabolic syndrome after adjusting for confounding covariates. Statistical models were adjusted for potential confounding covariates, including sex, age, education attainment, marital status, income, smoking, alcohol, and physical activity. Statistical significance was set at P value <0.05. Following the statistical guideline of the KCDC, all analyses were performed using SURVEY commands available for complex sample option in SAS 9.4 software (SAS Institute, Cary, NC).
Results
Table 1 shows the descriptive characteristics of participants according to the status of household food security. Of finally enrolled 18,782 participants, 49.4% of participants were males. The mean age of all participants was 45.6 years. The majority (68.0%) of participants were married. Percentages (standard error) of those with high food security, marginal food security, low food security, and very low food security were 80.1% (0.6), 11.7% (0.4), 7.0% (0.3), and 1.2% (0.1), respectively. Proportions of food-secure and food-insecure participants were 91.8% and 8.2%, respectively. In subgroups of sex, age, marital status, education attainment, household income, smoking, alcohol intake, physical activity, and BMI were significantly different among the groups (P < 0.05).
Characteristics of a Representative Population of Korean Adults Stratified by Household Food Security Status in Korean National Health and Nutrition Examination Survey 2012–2015
Data are presented as weighted percentage (standard error) unless otherwise stated.
Same superscript letter means not significantly different by Duncan's multiple range test.
The overall prevalence of metabolic syndrome was 27.3%, showing an age-dependent increase (11.3%, 30.5%, and 50.8% for age groups of 19–39 years, 40–59 years, and ≥60 years, respectively). Of the total participants, 2.4% were categorized as having both metabolic syndrome and food insecurity. Table 2 shows the prevalence of metabolic syndrome and its individual components according to food security status. The prevalences of metabolic syndrome in the high, marginal, low, and very low food security groups were 26.2%, 32.3%, 30.2%, and 28.8%, respectively. Of the five individual components of metabolic syndrome, reduced high-density lipoprotein level was the most common (35.7%), followed by hypertension (34.0%), central obesity (32.4%), hyperglycemia (30.5%), and hypertriglyceridemia (28.9%). Compared to the high food security group, the marginal food security group showed higher prevalences of central obesity, hypertriglyceridemia, reduced high-density lipoprotein levels, and hypertension. The low food security group also had higher prevalences of central obesity, reduced high-density lipoprotein levels, and hypertension than the high food security group.
The Prevalence of Metabolic Syndrome and Its Individual Components According to Food Security Status
Data are presented as weighted percentage (standard error).
Boldface values indicate significant differences between the groups after adjusting for multiple comparisons using the Bonferroni correction method.
Of the total participants, the prevalence of metabolic syndrome was 26.4% in 2012, 26.2% in 2013, and 25.9% in 2014. It increased to 30.3% in 2015. This trend occurred in all subgroups of food security status except for the very low food security group. The increment of the prevalence of metabolic syndrome was the highest in the marginal food security group (an increase of 9.4%, from 29.4% to 38.8%), followed by that in the low food security group (an increase of 8.7%, from 27.2% to 35.9%) and the high food security group (an increase of 3.2%, from 25.7% to 28.9%).
Supplementary Table S1 shows the prevalence of metabolic syndrome according to participants' characteristics and food security status. In subgroups of the female sex, never married, married, middle school education attainment, never smoker, moderate and none alcohol intake, physical activity, and normal weight were significantly different among the groups (P < 0.05).
Unadjusted and adjusted odds ratio (aOR) and 95% CI for associations of metabolic syndrome and covariates are presented in Supplementary Table S2. Marginal food security (OR: 1.34, 95% CI: 1.19–1.50, P < 0.001) and low food security (OR: 1.22, 95% CI: 1.04–1.42, P = 0.01) were associated with increased risk of metabolic syndrome. However, after controlling for demographic and socioeconomic covariates, neither marginal food security (aOR: 1.02, 95% CI: 0.87–1.19, P = 0.86) nor low food security (aOR: 0.88, 95% CI: 0.71–1.08, P = 0.22) was significantly associated with increased risk of metabolic syndrome. Significant risk factors for metabolic syndrome in adjusted models included age ≥60-year old (aOR: 2.21, 95% CI: 1.93–2.52, P < 0.001), educational attainment less than elementary school (aOR: 1.85, 95% CI: 1.55–2.21, P < 0.001), divorced/separated/widowed (aOR: 1.29, 95% CI: 1.12–1.50, P < 0.001), current smoking (aOR: 1.28, 95% CI: 1.05–1.54, P = 0.01), no physical exercise (aOR: 1.26, 95% CI: 1.11–1.43, P < 0.001), and heavy alcohol intake (aOR: 1.14, 95% CI: 1.00–1.31, P = 0.001).
Table 3 shows associations of food security status and individual metabolic syndrome components. In unadjusted models, central obesity (marginal food security OR: 1.34, 95% CI: 1.19–1.50, P < 0.001; low food security OR: 1.30, 95% CI: 1.10–1.53, P < 0.01), hyperglycemia (marginal food security OR: 1.19, 95% CI: 1.06–1.34, P < 0.01), high-density lipoprotein (marginal food security OR: 1.35, 95% CI: 1.21–1.51, P < 0.001; low food security OR: 1.26, 95% CI: 1.09–1.46, P < 0.01), and high blood pressure (marginal food security OR: 1.27, 95% CI: 1.13–1.43, P < 0.001; low food security OR: 1.35, 95% CI: 1.14–1.59, P < 0.01) were significantly associated with food security status. However, none of the five metabolic syndrome components was significantly associated with food security status in the adjusted model.
Unadjusted and Adjusted Odds Ratio and 95% Confidence Interval for Associations Between Food Security Status and Metabolic Syndrome Components
Discussion
This study investigated whether food security status was associated with a higher risk of metabolic syndrome in a representative population of Korean adults. Although marginal food security and low food security were associated with increased risk of metabolic syndrome in the unadjusted model, their associations were not significant in the adjusted model. Significant risk factors for metabolic syndrome included female sex, older age, lower attainment of education, current smoking, and none/intermittent physical activity. To the best of our knowledge, this is the first nationwide, general population-based study to investigate the association between food security status and metabolic syndrome outside the United States.
Consistent with a previous report from the United States, 14 the prevalence of metabolic syndrome was significantly higher in the marginal food security group without adjustment. Parker et al. have shown that marginal food security and very low food security adult groups had independently increased risks of metabolic syndrome (aOR: 1.8, 95% CI: 1.3–2.5 and aOR: 1.7, 95% CI: 1.1–2.4, respectively) compared to that in the food-secure group. They explained that extreme dietary behaviors of increased consumption of inexpensive and energy-dense foods of low nutritional value could increase the risk of metabolic syndrome in the United States. 14 In the current study, however, after controlling for important covariates, there was no significant association between food security status and metabolic syndrome in Korean adults. Differences in the general dietary patterns between the United States and Korea could be the main reason for this finding. Ordinary dietary patterns in Korean adults with food insecurity, especially in the older individuals, do not seem to be frequently associated with higher intakes of energy, fat, or sugar. For example, more microwavable or quick-cook frozen unhealthy foods have shown to be frequently associated with food insecurity in the United States. 22 However, such foods are much less familiar to many Korean older individuals. Different diet patterns reflect different sociocultural characteristics between the two countries. While examining adult dietary data from the 2003 to 2010 National Health and Nutrition Examination Survey (NHANES) in the United States, Nguyen et al. found that food insecurity was associated with significantly higher intakes of added sugars and empty calories. 23 In a study on adults in the United States, Leung et al. found that the food insecurity group had higher intakes of high-fat dairy products, salty snacks, and processed meat in low-income households from the 1999 to 2008 NHANES. 24 Recent cross-sectional studies based on the KNHANES survey compared food and nutrient intakes according to food insecurity status. 25,26 Using the 2012 KNHANES data, Kim and Oh compared dietary intakes between food-secure and food-insecure households in Korea. 25 They found that the mean daily intakes of protein, crude fiber, vitamins, and minerals were significantly lower in food-insecure adults than those in food-secure adults. However, the mean daily intakes of energy, fat, and carbohydrates were similar between the two groups. In a study of Korean older participants from the 2010 KNHANES, Lee et al. found that protein and vitamin intakes were significantly lower in the food-insecure group. 26 However, total energy and fat intakes were similar across food security status groups. Collectively, these data suggest that different dietary patterns in the food insecurity group are responsible for the different associations between food insecurity and metabolic syndrome. The results of the current study are also consistent with those in the reports on the association between food insecurity and obesity/metabolic abnormalities in several countries outside the United States. 18,27 –29
Another possible explanation for the association between metabolic syndrome and food insecurity is cyclic shortage of food with subsequent overeating of household members having food insecurity. 30,31 Food insecure households may often face both periods of food availability and food scarcity. The Supplemental Nutrition Assistance Program (SNAP), formerly called as Food Stamp Program, is a USDA program that provides food-purchasing assistance to low-income people. It has been hypothesized that it may create a “food stamp cycle.” Households receiving monthly aid often fall short of food at the end of the month. They may have feelings of hunger that is often followed by overeating in weeks immediately after the aid is received. 32 In contrast to food aid programs in the United States, Korean governmental food aid programs have been implemented mainly on daily provision of foods for low-income families, especially for children and the elderly. 33 It gives them minimal chance to have an overeating behavior. The food voucher system has been operated only to a limited extent in Korea. It also should be noted that, according to the National Basic Livelihood Security System, food support budget is being provided in the form of cash assistance, 26 which often can be used for other purposes. It also reduces the chance of cyclic overeating in food-insecure people. Therefore, different food aid programs might have contributed to these discrepancies between the United States and Korea.
The relationship between food insecurity and metabolic abnormalities might be different according to racial or ethnic group. Certain ethnic groups might be more frequently predisposed to several features of metabolic syndrome. Several previous studies have suggested that the prevalence of metabolic abnormalities can be varied according to the race/ethnicity. 34 –38 Type 2 diabetes mellitus and coronary artery disease show high prevalence in urban and migrant Asian Indians. 39 –41 Previous investigations have shown that, compared to age/height/weight-matched Caucasians, Indian adults have a higher percentage of visceral fat, 35 which is related to dyslipidemia and increased frequency of insulin resistance. 42 Recently, a Malayan group has determined the differences in the prevalence of metabolic syndrome across ethnicities in Malaysia, a multiethnic country. 37 Compared to ethnic Malay, ethnic Chinese had the lowest prevalence of metabolic syndrome (aOR: 0.84, 95% CI: 0.78–0.91), while ethnic Indians had the highest prevalence (aOR: 1.31, 95% CI: 1.20–1.44). Those findings suggest that exposure to similar food insecure status could lead to different levels of metabolic abnormalities. However, the current study was not designed to examine this issue. This needs further investigations.
Although food insecurity and the risk of metabolic syndrome were not directly related to our results, these are important contemporary public health issues. The older population is vulnerable to both conditions. In particular, older individuals living alone are more likely to be food insecure than those living with others. 17 In 2018, 1.3 million adults aged ≥65 (8.9%) who lived alone were food insecure in the United States. 43 Recent reports have demonstrated that the prevalence of food insecurity among the older Koreans who live alone was 15.3%–17.1%, which is approximately twice as high as that of the older population in the United States. 44,45 The number of older individuals with food insecurity is projected to increase with the rapid growth of the aging population. This suggests that protecting the older individuals from food insecurity has crucial public health importance to lessen the burden of food insecurity-related problems. We believe that efforts to prevent unhealthy dietary patterns, such as cyclic overeating or higher intake of foods with lower nutritional values, should be incorporated in the economic and social support programs for the older individuals living alone.
The current study has some limitations. First, this study used the modified NCEP ATP III criteria for the diagnosis of metabolic syndrome. The use of different criteria for metabolic syndrome might be associated with different prevalences of metabolic syndrome. Second, this study used the data of food insecurity measured at the household level. Individual food insecurity status can be different among the same household members. Third, this study did not evaluate the impact of food insecurity on children or adolescents. Fourth, we did not investigate the impact of geographic location in Korea, which may be an important factor in food security and metabolic syndrome. Finally, detailed analysis of dietary intake according to food security status was not performed in the current study. However, results of aforementioned KNHANES studies comparing food and nutritional intake between food-secure and food-insecure groups support our results. 25,26
In conclusion, contrary to a prior report from the United States, food security status was not significantly associated with an increased risk of metabolic syndrome in Korean adults. These results suggest that the association between food security status and metabolic syndrome can be different according to the region and sociocultural characteristics.
Footnotes
Author Disclosure Statement
No conflicting financial interests exits.
Funding Information
No funding was received for this work.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.