
Abstract
Nucleic acid therapeutics are an established class of drugs that enable specific targeting of a gene of interest. This diverse family of drugs includes antisense oligonucleotides, siRNAs, and mRNA replacement therapies, which can elicit both gene repression and activation, primarily at the RNA level. Recent advances in medicinal chemistry have increased drug potency and enhanced delivery and distribution to a broad array of tissue and cell types. A key advantage of nucleic acid therapeutics is in their application to monogenic diseases. Cystic fibrosis (CF) is one such disease that affects ∼70,000 people globally. This severe disease is an excellent candidate for nucleic acid therapies, as it is due to a genetic defect in a single epithelial chloride channel. Although CF affects many tissues, the primary cause of patient mortality is lung disease. Here we review the various nucleic acid therapeutic modalities and their mechanisms of action, the opportunities and challenges associated with application of nucleic acid drugs to the lung pathology of CF, and the current state and prospects for nucleic acid drugs for the treatment of CF.
Introduction
N
The focus of this review is the application of mRNA-targeting nucleic acid therapeutics to the severe lung disease cystic fibrosis (CF). CF is one among several chronic lung diseases which lack effective treatment, but it is unique in that it has a clear genetic basis: a defect in an epithelial chloride channel, the cystic fibrosis transmembrane conductance regulator (CFTR) [1]. While considerable effort has been made toward developing treatments for CF, existing drugs focus on minimizing symptoms of the disease or on a specific patient subpopulation [2]. There is still a substantial unmet need for a treatment which benefits all CF patients.
With recent advances in chemical modifications and conjugates that improve potency and delivery of nucleic acid therapies, application of these drugs to lung diseases is increasingly attractive. Through mRNA-specific targeting and technologies for both mRNA inhibition and modulation of mRNA processing and translation, nucleic acid drugs have the potential to change the landscape of treatment for CF. This review will briefly introduce the various classes of nucleic acid therapies and their mechanisms of action, describe the opportunities and challenges associated with nucleic acid therapeutics for CF, and reflect on the current state of nucleic acid therapies for CF.
Classes of Nucleic Acid Therapeutics and Their Mechanisms of Action
Nucleic acid drugs are well-established therapeutic modalities. While there are several distinct classes of these drugs, they share some key characteristics to achieve activity. Specifically, nucleic acid therapeutics require bioavailability and effective delivery to the desired tissue or cell type, as well as nuclease resistance and affinity for the target. Chemical modifications enhance these properties and vary depending on the class of drug and the desired effect on the target. These include, but are not limited to, backbone modifications to a phosphorothioate (PS) linkage or to a phosphorodiamidate morpholino oligomer and alteration of the 2′ hydroxyl to a fluoro (F), methoxy (OMe), or methoxyethyl (MOE). Our discussion of chemical modifications to nucleic acid drugs is not comprehensive, and we refer the reader to other publications for in-depth review [3,4]. Here we outline the different classes of nucleic acid drugs and their mechanisms of action, with a brief overview of the chemistries that enable these applications.
Antisense oligonucleotides
Antisense oligonucleotides (ASOs) are single-stranded moieties that enable mRNA degradation, upregulation of translation, and splice modulation through distinct mechanisms of action [3].
RNase H-mediated cleavage is a well-studied mechanism and a broad approach utilized by ASOs [3,5]. After Watson–Crick base pairing of the ASO to the target RNA, RNase H recognizes the ASO-RNA hybrid and endonucleolytic mRNA cleavage occurs, reducing target mRNA levels in the cell (Fig. 1a; “RNase H1 Mechanism”). To effectively recruit RNase H and induce cleavage of the target mRNA, the ASO is designed as a “gapmer,” with two “wings” of modified nucleotides surrounding an unmodified DNA-like “gap.” The “wings” protect the ASO from degradation before target mRNA hybridization, and the “gap” facilitates recognition of the ASO-mRNA duplex as a “DNA-RNA” hybrid by RNase H. This approach is extensively used to knockdown RNAs that code for genes responsible for a disease, demonstrated in the clinic by the FDA-approved hypercholesterolemia drug Mipomersen and over 30 programs in preclinical and clinical development [3,6].

Nucleic acid therapeutic modalities and their mechanisms of action.
Other ASOs are uniformly modified with a PS backbone and 2′ modifications, such as 2′ OMe or 2′ MOE, to serve as “steric blocks” and modulate posttranscriptional events (Fig. 1a; “Steric Block Mechanism”). Uniform morpholino oligomers are also used for the same purpose. Steric blocking ASOs have been used to increase protein expression through blocking upstream AUG sites [upstream open reading frames (uORFs)] in the 5′UTR of mRNAs, thus increasing primary open read frame translation [7]. Similarly, steric blocking ASOs can prevent association of regulatory factors with a transcript of interest, exemplified by ASOs used to antagonize microRNAs and block exon junction complex assembly [8–10]. ASOs to modulate alternative splicing, termed splice-switching oligonucleotides (SSOs), are another form of steric block ASO. SSOs bind to a pre-mRNA at sites that either enhance or inhibit splicing of specific exons, thus promoting either exon skipping or exon inclusion. Nusinersen for Spinal Muscular Atrophy and Eteplirsen for Duchenne's Muscular Dystrophy are examples of FDA-approved SSOs in the clinic [11,12]. Nusinersen was also recently approved in Europe.
Delivery of ASOs to cells and many tissue types is efficient without modification or conjugation. Protein interactions with ASOs mediate uptake through various endocytic pathways that have recently been investigated in more detail [13]. Ligand conjugation of ASOs enables tissue-specific delivery through receptor-mediated uptake, and this selective delivery approach has been utilized primarily for hepatocyte targeting to date, through use of an N-acetylgalactosamine (GalNAc) conjugate that is recognized and taken up by the asialoglycoprotein receptor [14]. Other ligand conjugation approaches to additional cell types and tissues are under investigation.
siRNAs
siRNAs are therapeutically validated double-stranded RNA oligonucleotides that mediate degradation of the target mRNA [15,16] (Fig. 1b). The 20–24 nucleotide siRNAs are loaded into the RNA-induced silencing complex, and the leading strand of the siRNA then binds to the cognate site in the desired mRNA target, inducing cleavage and degradation of the target. Patisiran is the most advanced siRNA drug, which is in phase 3 clinical development for the treatment of hereditary transthyretin-mediated amyloidosis [17].
Due to the charge and double-stranded nature of siRNAs, delivery to the cell and tissues is challenging. siRNAs are often packaged in lipid nanoparticles (LNPs) and conjugated with ligands for tissue-specific receptors to facilitate intracellular distribution. LNPs are typically made up of four different lipids that serve distinct functions [18]. All four lipids are necessary to destabilize the lipid bilayer for optimal intracellular delivery and to achieve ideal stability of the nanoparticle. Due to the charge and size of the nanoparticles, immune responses and liver damage are common at high doses of LNP-packaged drugs [18,19]. Thus, careful selection of lipids and the optimal ratios of different lipid components are critical for LNP delivery systems. As for ASOs, ligand conjugation of siRNAs is most common for delivery to the liver through GalNAc conjugation [20]. Additional ligand conjugation approaches will enable selective delivery to other tissues and cell types, thus mitigating toxicity and increasing activity.
Gene therapy
Nucleic acid therapeutics enable gene therapy as well. Gene therapy approaches include directed genome editing strategies using CRISPR-Cas9 or zinc finger nucleases and the more transient mRNA replacement therapy. Since gene editing requires delivery of exogenous nucleases in protein form and targets DNA rather than RNA, this review will focus on mRNA replacement strategies. Gene therapy and editing approaches for CF have recently been reviewed in Ref. [21].
mRNA replacement is the delivery of a desired mRNA to cells in a tissue of interest, to replace the mutated or dysfunctional endogenous RNA (Fig. 1c). This approach has not yet been validated in the clinic. Preclinical research has focused extensively on modifying the LNPs and the mRNA to facilitate delivery to the cell, improve stability of the RNA in the cell, reduce the immune response to the exogenous mRNA, and promote efficient translation of the delivered mRNA [22–26]. Initial proof-of-concept studies have been conducted, demonstrating the utility of LNPs for delivery of mRNA for efficient translation, using hemophilia mice and Factor IX mRNA [27,28].
CF: An Emerging Opportunity for Nucleic Acid Therapeutics
CF is an autosomal recessive genetic disorder that affects ∼70,000 individuals globally [29]. CF is caused by mutations in the CFTR gene, which encodes a cyclic AMP-activated chloride channel [1,30–32]. There are more than 2,000 identified disease-causing CFTR mutations that fall into six distinct mutation classes, based on the effect on CFTR mRNA and protein synthesis and posttranslational processing and function (www.genet.sickkids.on.ca). Mutations in CFTR result in epithelial defects in many tissues, but the primary cause of morbidity and mortality in CF patients is lung disease [33]. CFTR resides in the apical layer of the airway epithelium. Defects in chloride, water, and bicarbonate transport due to mutations in CFTR cause dehydration of the lung airways and subsequent mucus buildup. Airway blockage and mucus accumulation lead to persistent bacterial infections in CF patients, contributing to chronic inflammation and pulmonary deterioration, ultimately causing respiratory failure [33].
Recent reports suggest that pulmonary exacerbations in CF patients may be caused by factors other than water and chloride imbalances as well. Increased sodium transport in CF disease is partially due to hyperactivation of the epithelial sodium channel (ENaC), which can contribute to dehydration of the airways and mucus buildup [34,35]. Dysregulation of bicarbonate transport by CFTR is also a proposed mechanism of airway hydration defects [36].
Therapeutic approaches for CF have focused primarily on alleviating symptoms of lung disease. Patients undergo hours of treatment per day to resolve mucus buildup and clear airways. Nevertheless, life expectancy for CF patients is still only 40 years in developed countries [37]. Recent advances have resulted in the development of small molecules that facilitate increased CFTR folding and trafficking to the cell surface [2]. Other small molecules promote chloride transport through stabilizing the open conformation of the ion channel [2]. While these drugs are a significant step toward a cure for CF patients, they are effective for limited classes of mutations and, thus, are relevant for only a fraction of patients. For example, the leading small molecule drugs for CF, Kalydeco and Orkambi, are effective at increasing CFTR trafficking to the cell surface and its chloride transport function, but only for patients with a single class of CFTR mutation [2,38–40]. Additional small molecules to increase CFTR expression, as well as improved “corrector” compounds, are in development, but these also are limited in efficacy to specific subpopulations of CF patients. Thus, there remains a need for therapies that can be used by all CF patients.
A significant challenge in the drug discovery and development space for CF is the variety of CFTR mutations that cause CF. Nucleic acid therapeutics, through their nucleotide specificity for a single gene and the potential for mRNA replacement, represent a promising venue for novel CF drugs that could be impactful for all CF patients. Recent advances in the delivery of siRNAs, mRNA replacement therapy, and the understanding of ASO distribution in the lung have paved the way for nucleic acid drugs to treat CF disease specifically in the lung.
Delivery of Nucleic Acid Therapies to the Lung
Aerosol inhalation is a common and proven route of pulmonary drug delivery. For treatment of lung diseases, inhalation affords a noninvasive and specific delivery route with minimized systemic exposure. However, the lung has defense mechanisms in place to protect against entry of foreign substances, and these mechanisms create a barrier for entry of drugs. In addition, the diseased lung, particularly in the case of CF, has a very different airway architecture and mucociliary landscape, which presents unique challenges for drug delivery. Various factors contribute to efficacious and broad distribution of drug in the lung, several of which can be controlled by the delivery device. This review will focus primarily on the challenges associated specifically with nucleic acid drug delivery to the CF lung, and not on device strategies, which are reviewed in detail in Refs. [41,42].
The respiratory system is divided into the upper and lower respiratory tracts. The nose, nasal cavity, and pharynx comprise the upper respiratory tract, while the lower tract consists of the larynx, trachea, bronchi, and alveoli of the lungs [43]. The lungs are composed of various cell types, including vascular cells, fibroblasts, macrophages, and epithelial cells. Within the epithelial layer, which lines the airways, are both mucus-producing goblet cells and ciliated cells. These two cell types together are paramount to the lung's ability to eliminate foreign substances. Penetrating this system requires optimal particle size, which can be achieved using modern nebulizer devices. In the diseased lung, particularly in CF, mucociliary clearance is aberrant, thus altering drug deposition by nebulizer devices to some extent [43–45].
Nucleic acid therapeutics have been delivered by aerosol to the lung in many forms. Naked mRNA, LNP-encapsulated siRNA, ASOs, and other modalities all have been administered to the lung in animal models and, in some cases, in patients [43,46–49]. However, there are significant considerations for delivery of similar moieties to human CF lungs, particularly for patients with extensive mucus buildup and undergoing other treatments for CF. The lack of robust small rodent models for CF lung disease and the significant differences in rodent and human lung architecture prevent this issue from being thoroughly addressed in preclinical studies [50,51]. The expanded use of recently developed animal models that more accurately recapitulate the human CF lung, including CF ferret and pig models, will enable more relevant preclinical evaluation of drug delivery and distribution [51,52].
In addition, effective deposition of drug into the lung does not translate to efficient delivery to all lung cell types. Thus, ligand-conjugation approaches may prove useful for specifically targeting a cell population of interest. Initial studies with a peptide derived from the urokinase plasminogen activator (uPA) demonstrated enhanced gene transfer to airway epithelial cells through the uPA receptor [53]. Further investigation into cell surface receptors unique to airway epithelial cells in the lung will enable use of ligands that may improve drug delivery for CF, which would allow for lower dosing and improved efficacy.
Drug composition also plays a significant role in distribution and delivery. Small molecules are easily formed into particles that can deposit in the airways and alveoli of the lung; however, their short half-life necessitates at least daily dosing for therapeutic benefit [54]. Nucleic acid therapies vary in size, but are all much larger than small molecules. LNP packaging can control the particle size to some degree. However, lipid composition and potential ligand conjugation of nucleic acid therapies will alter the viscosity, size, and charge of the drugs. These factors will all have to be carefully considered and optimized to achieve optimal viscosity and particle size for effective deposition into the desired lung compartments and cell types. A significant advantage for nucleic acid therapies is their longer half-life than small molecule drugs, which may allow for less frequent dosing.
Finally, an important consideration for delivery of any novel therapy to the lung for CF is the potential of drug–drug interactions with any of the drugs a CF patient may already be taking. This is particularly true for the drug Pulmozyme (dornase alfa), a DNase alpha mucolytic taken by CF patients to promote airway clearance [55,56]. Since nucleic acid drugs are highly modified, sometimes strongly resembling DNA, it is important that these drugs are tested in combination with Pulmozyme treatment to ensure that they do not get degraded and therefore lose efficacy.
Current Nucleic Acid Therapies in Development for CF
RNase H ASO programs
ASOs are effective at eliciting RNase H-mediated degradation of a desired target. While CF disease is caused by loss-of-function mutations in CFTR, other genes also have a role in disease progression and severity. The sodium channel ENaC, for example, has been reported to be hyperactivated in response to CFTR defects, contributing to dehydration of the airways and mucus accumulation [57]. ENaC inhibition is therefore an attractive path for mucus reduction and airway clearance. A significant advantage of ENaC inhibition is that it can be a therapeutic option for all CF patients, irrespective of genotype.
Ionis Pharmaceuticals recently published data for an aerosolized mouse ENaC ASO [58]. A human ENaC inhibitor is now in preclinical development for the treatment of CF (Fig. 2). The published compound is a 16-nucleotide gapmer ASO, which elicits RNase H-mediated degradation of the mouse ENaC mRNA. This aerosolized ENaC ASO potently and specifically reduced lung ENaC mRNA and protein in mouse models with mucus accumulation and CF-like lung disease. Furthermore, ENaC ASO treatment downregulated mucus marker expression and ameliorated goblet cell metaplasia, inflammation, and airway hyperresponsiveness with no effect on renal ENaC. ENaC regulates sodium transport in other organs, including the kidneys, and small molecule approaches to ENaC inhibition have in some cases resulted in hyperkalemia, an effect believed to be due to kidney ENaC inhibition [59]. Consistent with the lack of systemic exposure, ENaC inhibition was not observed in organs outside of the lung, and no toxicities were found after ENaC ASO administration in multiple distinct mouse models. While these preclinical data are promising, the clinical benefit of ENaC ASO administration to CF patients remains to be seen.
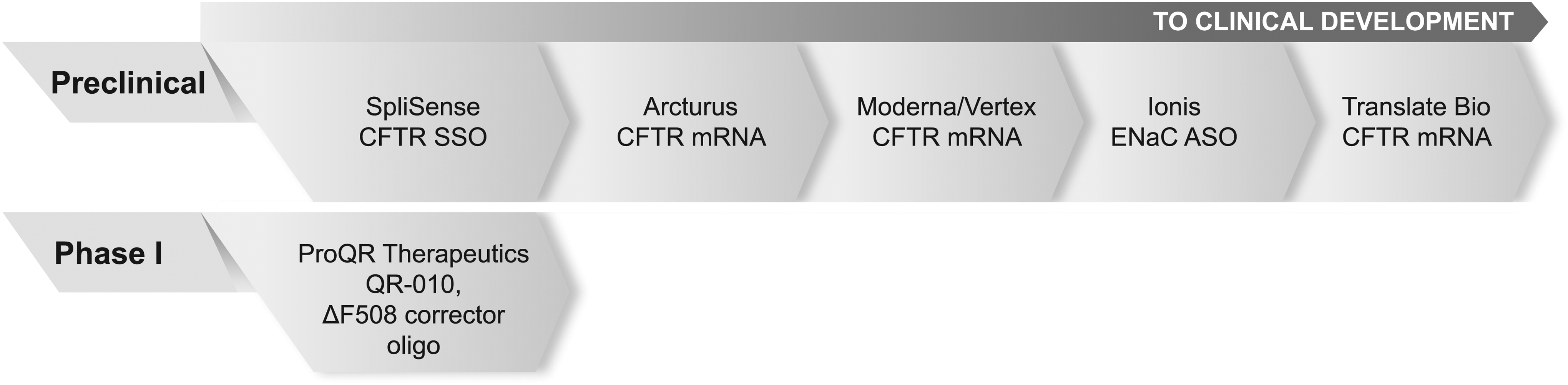
Nucleic acid therapeutics in development for CF. CF, cystic fibrosis.
There are other potential targets for ASOs as treatments for CF as well. For example, significant effort has been made toward understanding the proteins involved in turnover of CFTR at the membrane, and this research has yielded valuable information about factors that can be inhibited to promote CFTR stability at the cell surface [60]. ASO and siRNA approaches to knock down these factors and others that contribute to CF disease are yet to be explored.
Splicing modulation ASO programs
Approximately 13% of CF-causing mutations affect splicing of the CFTR pre-mRNA [61–63]. Some of these mutations result in inclusion of a cryptic exon harboring a pretermination codon (PTC). Thus, the mutated mRNA is targeted for degradation by the nonsense-mediated mRNA decay pathway. SSO strategies to prevent cryptic exon inclusion for a few CFTR mutations are in early-stage research. Other splicing defects caused by CFTR mutations have not yet been addressed by SSO approaches.
SpliSense has developed a strategy utilizing 2′ OMe PS SSOs to promote correct splicing of the 3,849 + 10 kb C-to-T CFTR mRNA (Fig. 2) [64]. They have demonstrated increased levels of correctly spliced mRNA and improvements in CFTR channel function in human nasal epithelial cells through SSO treatment. However, this is still an early-stage preclinical approach and has yet to be evaluated in animal models.
A similar SSO strategy has been applied to the c.2657 + 5G>A CFTR mutation [65]. SSO treatment increased CFTR mRNA and protein levels and improved CFTR channel function in an expression mini-gene reporter cell line for the c.2657 + 5G>A mutation. Evaluation of this approach in more relevant CF cell and animal models will be of interest.
mRNA replacement programs
mRNA replacement is an attractive therapeutic option for CF, as various mutations give rise to the disease. Delivery of a wild-type CFTR mRNA would thus be an effective treatment for any patient with CF, irrespective of the underlying mutation in CFTR that gives rise to their disease. Three companies have mRNA replacement programs in place for CF (Fig. 2). All three mRNA replacement strategies rely on LNP-mediated delivery of mRNA and are expected to use aerosol delivery to the lung. While these programs are currently preclinical and no literature reports have been published on CFTR mRNA delivery in vitro or in vivo, first in human studies has been planned (https://translate.bio).
In 2016, Moderna Therapeutics entered a 3-year collaboration with Vertex Pharmaceuticals focused on discovery and development of a therapeutic mRNA molecule for CF (www.modernatx.com). This program is in early-stage discovery research. Moderna has demonstrated delivery, stability, and efficacy of LNP-encapsulated modified mRNAs in studies for influenza and Zika virus vaccines in mice, ferrets, and nonhuman primates [66–68].
Arcturus Therapeutics has a 2-year collaboration in place with the Cystic Fibrosis Foundation to develop a therapeutic mRNA delivered through their Lipid-enabled and Unlocked Nucleomonomer Agent modified RNA (LUNAR™) platform directly to the lung by aerosol inhalation. The neutral charge of the LUNAR nanoparticles is thought to minimize toxic effects observed with other positively charged lipid delivery systems. Arcturus has demonstrated liver delivery of human Factor IX (FIX) mRNA in mouse models of hemophilia with the LUNAR platform [28]. LUNAR-FIX mRNA was efficiently translated into FIX protein in the liver and circulated, restoring levels of FIX protein and normal clotting activity in FIX−/− mice for up to 6 days after initial dose administration. Arcturus plans to work closely with CFF to develop a similar approach with CFTR mRNA delivered to the lung.
Translate Bio, Inc., formerly RaNA Therapeutics, has recently joined the mRNA replacement therapy efforts through acquisition of Shire Pharmaceuticals' mRNA platform. Shire Pharmaceuticals has a proven LNP approach for delivery of mRNA in mice. Like Arcturus, Shire tested a LNP-encapsulated human FIX mRNA in hemophilia mouse models [27]. The mRNA was effectively delivered and translated, and therapeutic benefit was demonstrated up to 72 h after dose administration. Translate Bio is expected to begin Phase I clinical studies in early 2018 for CF.
Other nucleic acid programs
ProQR has developed an oligonucleotide drug (QR-010) that specifically “repairs” ΔF508 mutated CFTR mRNA in the cell (Fig. 2). This drug is currently in Phase 1B clinical trials. QR-010 is an oligonucleotide that is thought to act by inserting missing bases into the ΔF508 mRNA, restoring the wild-type CFTR mRNA sequence [69]. The mechanism of base insertion has yet to be elucidated.
ProQR has initiated two clinical trial studies to date. The first study completed at the end of 2016. Although the study was very small, QR-010 seemed to improve CFTR function in all 10 homozygous ΔF508 CF patients. Surprisingly, QR-010 was not effective for heterozygous ΔF508 patients. This proof-of-concept study used nasal potential difference as a measure of CFTR chloride transport after 4 weeks of topical treatment of QR-010 to the nasal mucosa. The second clinical trial study is a more detailed Phase 1B study with QR-010 delivered by aerosol (www.proqr.com). The data from this Phase 1B study will provide valuable information regarding the efficiency of duplex oligonucleotide deposition into human CF lungs, which may inform future development of nucleic acid therapeutics for CF and other lung diseases.
Conclusions and Perspectives
Nucleic acid therapeutics are a diverse class of drugs, utilizing distinct mechanisms to elicit both gene repression and activation at the mRNA level. The various therapeutic modalities, including ASOs, siRNAs, and mRNA replacement strategies, have advanced significantly in recent years, leading to increased potency and enhanced delivery and distribution to a broad array of tissues and cell types. This has enabled development of nucleic acid–based mRNA targeting strategies for the treatment of CF. While there are several different nucleic acid therapies in preclinical and clinical stages for CF, additional approaches require further investigation and effort, and delivery to the diseased lung has yet to be carefully evaluated.
mRNA replacement strategies to correct the CFTR defect are in preclinical programs. These strategies have significant promise for CF, as they can be used for all CF patients. The three programs differ somewhat in packaging and likely the chemical modification of the mRNA, and these factors affect the stability and durability of the delivered mRNA. The Arcturus LUNAR-FIX approach, for example, is much more durable than Shire's similar replacement strategy for FIX [27,28]. Approaches to replace the CFTR mRNA may have different effects, as chemical modifications and/or lipid packaging strategies may continue to improve. While mRNA delivery is an attractive option for CF therapy, there remain several key challenges. The CFTR mRNA is very long and, therefore, may be difficult to synthesize and deliver to the cell while maintaining proper translation and regulation of the mRNA. In addition, effective mRNA delivery to the appropriate cell populations in the lung is critical for therapeutic benefit. Finally, mRNA replacement is still a new therapeutic strategy, and the safety of mRNA delivery in human lungs has yet to be evaluated. Advances in LNP delivery mechanisms and chemical modifications of mRNAs for replacement strategies may mitigate previously observed inflammation and toxicity with these particles.
There are three oligonucleotide programs for CF: CFTR splicing modulation, ENaC inhibition, and ΔF508-CFTR correction. Splicing modulation approaches for a few specific CFTR mutations are currently in preclinical evaluation. These strategies could offer a therapy for CF patients that have limited treatment options. An inevitable drawback to this method is that the SSO must be redeveloped for each individual CFTR mutation that results in a splicing defect. While SSOs to prevent cryptic exon inclusion show benefit in vitro, validation in relevant animal models and additional primary cell models is yet to be conducted. Thus far application of splicing modulation has only been to mutations resulting in cryptic exon inclusion. CFTR mutations result in a variety of splicing defects, necessitating the extension of splicing modulation approaches to other mutations.
The ENaC inhibitory ASO is in preclinical development at Ionis Pharmaceuticals. This ASO has great potential as a treatment for all CF patients, and it will be interesting to see how genotypically distinct groups of patients respond to lung-specific ENaC inhibition. This approach could be particularly beneficial to patients who are not responsive to existing CFTR modulators. Aerosol delivery of the ENaC ASO and QR-010 to patients will provide valuable information on ASO distribution to diseased human lungs.
QR-010 represents a novel strategy for ΔF508-CFTR correction, and further investigation of the underlying mechanism through which the oligonucleotide acts could prove very useful for future RNA editing approaches. The efficacy of this approach is still unclear, however, as the initial clinical study was small and therefore had very limited data. A significant drawback to QR-010 is the lack of clinical benefit for heterozygous ΔF508 patients, limiting the drug to a smaller patient subpopulation. This may suggest that QR-010 is acting through a distinct mechanism than what is published or that there is some unidentified CFTR regulation that may contribute to efficacy in heterozygous patients. In either case, further evaluation in additional patients and a more complete mechanistic understanding of QR-010 are needed.
There are currently no siRNA programs for CF, but some preliminary work has been done toward siRNA-mediated inhibition of ENaC in human cells and in non-CF mice [70,71].
There remain many alternative mechanisms to be explored for ASO and siRNA approaches. CFTR-regulatory factors, such as the ubiquitin ligase RNF5 and the endosome protein DAB2, are additional targets for inhibition by ASO or siRNA that could result in increased surface retention of CFTR [60]. Factors that facilitate turnover of misfolded CFTR in the ER, such as BAP31, also represent strong candidates for inhibition strategies [72,73]. In addition, increasing the correctable pool of CFTR for small-molecule correction could promote increased CFTR function. Steric blocking ASOs designed to target the uORF in CFTR could achieve this, as could ASOs that prevent association of miRNAs with the CFTR mRNA, as some miRNAs have been demonstrated to regulate CFTR [74,75]. Inhibition of nonsense-mediated decay factors by ASOs or steric blocking of exon junction complexes may be potential therapeutic approaches for nonsense-mutated CFTR [10,76,77]. ASO-mediated pseudouridylation or adenosine deamination of PTCs in CFTR could also be used for these mutations [78–80]. Future investigations of nucleic acid therapeutic applications to these CFTR-regulatory mechanisms will substantially advance progress toward the goal of a treatment for all CF patients.
Although the lung is amenable to local drug delivery through aerosol inhalation, the diseased lung presents a hurdle to nucleic acid therapy distribution. Thick mucus and sputum, which are characteristic of CF lungs, present a major challenge for delivery. Small molecules penetrate mucus and sputum in the airways effectively; however, nucleic acid therapies are much larger and often are encapsulated in LNPs. While distribution to healthy lungs is effective, potential ligand conjugation strategies to target specific lung cell types could augment delivery to desired cell populations. Future clinical studies will shed light on the limitations presented by mucus in the CF lung and on the ability of nucleic acid drugs to distribute throughout the lung and achieve a meaningful clinical benefit.
CF is an excellent candidate for nucleic acid therapeutic approaches. The advances made in the next few years, as nucleic acid drugs progress through clinical studies for CF, will pave the way for novel strategies for other chronic lung diseases as well. The structural and mucociliary changes present in CF lungs are common to chronic obstructive pulmonary disease (COPD), asthma, and other lung diseases. Determining optimal lung delivery strategies for CF may be broadly applicable to a variety of other lung diseases, thus offering promising avenues for future therapeutic approaches with nucleic acid drugs.
Footnotes
Acknowledgments
The authors thank Jeff Crosby and Melissa Keenan for review of the article and Tracy Reigle for help preparing the figures. S.S. is funded by a Cystic Fibrosis Foundation postdoctoral grant.
Author Disclosure Statement
S.S. and S.G. are employees of Ionis Pharmaceuticals.