
Abstract
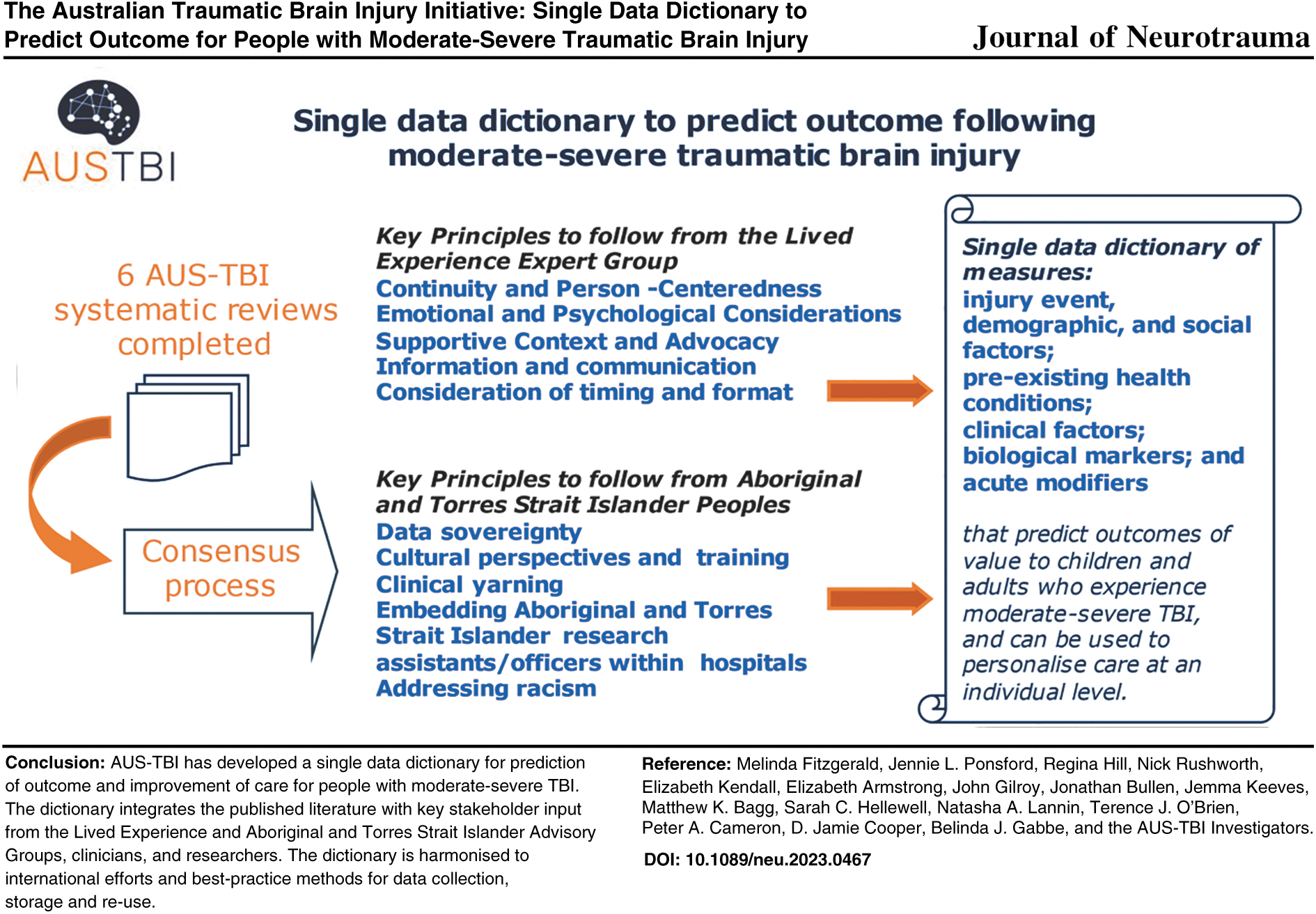
In this series of eight articles, the Australian Traumatic Brain Injury Initiative (AUS-TBI) consortium describes the Australian approach used to select the common data elements collected acutely that have been shown to predict outcome following moderate-severe traumatic brain injury (TBI) across the lifespan. This article presents the unified single data dictionary, together with additional measures chosen to facilitate comparative effectiveness research and data linkage. Consultations with the AUS-TBI Lived Experience Expert Group provided insights on the merits and considerations regarding data elements for some of the study areas, as well as more general principles to guide the collection of data and the selection of meaningful measures. These are presented as a series of guiding principles and themes. The AUS-TBI Aboriginal and Torres Strait Islander Advisory Group identified a number of key points and considerations for the project approach specific to Aboriginal and Torres Strait Islander peoples, including key issues of data sovereignty and community involvement. These are outlined in the form of principles to guide selection of appropriate methodologies, data management, and governance. Implementation of the AUS-TBI approach aims to maximize ongoing data collection and linkage, to facilitate personalization of care and improved outcomes for people who experience moderate-severe TBI.
Introduction
The need for personalized prediction of outcomes following TBI
Traumatic brain injury (TBI) results from many causes including road trauma, workplace incidents, interpersonal violence, and falls. It can be catastrophic, with lifelong impact on patients, their families, workplaces, the criminal justice system, and society as a whole. An incidence of 790 TBI cases per 100,000 person-years has been reported, 1 equating to 190,000 to 200,000 cases per year in Australia, of which about 20,000 are moderate to severe injuries. Other estimates have been lower, 2 indicating the difficulty of accurately defining incidence in this population. The rate and degree of recovery after moderate-severe TBI varies greatly, due in part to the complex and diverse nature of these injuries. Severe TBI has a high mortality rate of 30–40%, and less than 50% of patients achieve long-term independence. 3 New injuries add $2 billion in lifetime direct costs to the Australian health care system annually. 4 Between 2006 and 2015, there was no change in survival or functional outcomes following TBI, proving the need for better, targeted treatments to reduce mortality and improve quality of life for these individuals, and reduce negative impacts on families and society. 5
Despite decades of empirical research, prediction of outcomes after TBI at the level of the individual remains imprecise. We have only partial understanding of what it is about the person, their injury, their environment, or their care that moderates and/or determines the multiple outcomes that contribute to quality of life. At present, there is no indicator or group of indicators that can sufficiently predict treatment outcome or responsiveness to allow for personalized acute care and rehabilitation for individual patients with TBI.6–8 There is an urgent need to standardize approaches to data capture and harmonizse measures when assessing interventions and outcomes across sites and contexts.
Injuries are a key driver of health inequalities for Aboriginal and Torres Strait Islander Australians. 9 Research in the indigenous context raises further complexities and challenges, particularly when endeavoring to standardize approaches. Research with indigenous remote/rural communities identified that indigenous people struggle to rehabilitate after hospital discharge, experiencing significant impacts on families, home finances, and accessing services. 10 Clinical decision-making is inconsistent 11 and outcomes are not improving. 5 Inequalities persist, including hospital staff making racial judgements of indigenous peoples, such as assumption of alcohol consumption. 12
Existing prognostic models for moderate-severe TBI to assist early clinical decision-making have been derived from hospital admission data, for example, from the International Mission on Prognosis and Analysis of Clinical Trials (IMPACT) and Corticoid Randomization After Significant Head Injury (CRASH) trials. Age, the motor score component from the Glasgow Coma Scale (GCS), and pupillary reactivity, extended with specific computed tomography (CT) findings, provide percentage risks for poor outcome (area under the curve 0.801 and 0.796 for mortality and unfavorable functional outcome at 6 months, respectively). 13 Recent Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) studies have validated the IMPACT and CRASH models, finding that the models adequately identify groups of patients at high risk for mortality or unfavorable outcome. 14 The models are generally accepted to have insufficient precision to guide routine clinical use in individual patients. Notably, these models were designed to predict the Glasgow Outcome Scale (GOS) score, which may not adequately capture all outcomes of value to patients and their families, 15 including community participation.6,8
A 30-year prospective longitudinal outcome study of 3000 adults with moderate-severe TBI receiving rehabilitation in Victoria, Australia, has significantly informed prediction of long-term outcomes more broadly and allowed for international comparison of outcomes.13,16,17 However, models need to be refined for application to the broader TBI population across Australia and to consider prediction of neurodegeneration. Specific models for Aboriginal and Torres Strait Islander peoples are required that acknowledge the complexities of understanding, presentation, and treatment in these populations, and the relatively limited relevant data available. 18 Even less is known about the predictors of long-term participation and quality of life following TBI in children. The Pediatric Intensity Level of Therapy (PILOT) scale 19 has been used for prognosis, but it correlates only moderately with functional outcomes. 20 Overall, there are few longitudinal studies, risk of bias in studies is high, and there are only weak to moderate associations with variables considered crucial by people with lived experience of TBI, including quality of life, participation, employment, and education.21,22
The AUS-TBI approach to prediction of outcomes following TBI
The Australian Traumatic Brain Injury Initiative (AUS-TBI) national consortium presents this series of articles describing the national approach used to select the common data elements collected acutely that are hypothesized to predict outcome following TBI across the lifespan. 23 The consortium conducted a review of methodologies to identify best practice for identifying common data elements in neurological conditions. 24 Systematic literature reviews were conducted for five study areas, namely: social, 25 health, 26 clinical, 27 biological (including imaging and fluid biomarkers), 28 and acute interventions 29 to identify potentially predictive data elements collected in the acute phase of care. Another systematic review focused on the measurement of longer-term outcomes. 30
Identified data elements and the recommended measures were examined by clinicians and researchers in facilitated consensus group meetings. Prioritization of potentially predictive data elements was based on reliability, comparability, and feasibility of collection; data elements required for comparative effectiveness research were also identified.24–29 Long-term outcome measures were also prioritized based upon psychometric properties, demonstrated sensitivity to change across time and following interventions, cost and time of administration, potential to administer via phone or Internet, representation of perspectives of person with brain injury, close others and clinicians, international use, and translation into other languages. 30
In a series of facilitated sessions, people with lived experience of TBI were consulted about their preferences for data collection methods and topics (the Lived Experience Expert Group). The methodology and outcomes of the consultations are described in a preceding article of this series. 30 The AUS-TBI Aboriginal and Torres Strait Islander Advisory Group also met several times and considered the data elements and provided recommendations regarding the ways of collecting data and considerations for the project approach specific to Aboriginal and Torres Strait Islander peoples. The data elements will need further refinement to reflect an Aboriginal and Torres Strait Islander worldview, using assessment tools developed with Aboriginal and Torres Strait Islander peoples or alternative methodologies.18,31,32 The prioritized data elements for each study area24–29 were refined in accordance with lived experience input, and the long-term outcome measures were re-presented to people with lived experience for final review. 30 Thematic analysis of the guiding principles and values from the groups has informed the approach throughout.
The AUS-TBI Single Data Dictionary
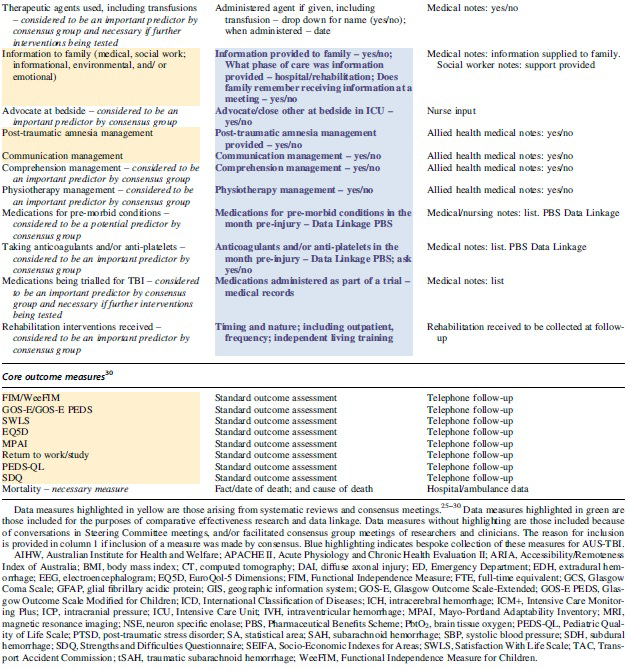
Using the approach described above, the AUS-TBI consortium developed a single data dictionary collated from each of the study areas. The acute common data elements that were potentially predictive of outcome, identified through literature review and consensus in each study area (articles 2–6), have been collated into a single data dictionary, together with demographic information that would be needed for identification of individuals and subsequent data linkage. A list was compiled consisting of these potentially predictive data elements, the means of collection identified at the consensus meetings, and the actual measure to be collected from clinical records or analyses (Table 1). Each data element has been classified as either currently available from existing data collection methodologies or requiring bespoke data collection.
Single Data Dictionary


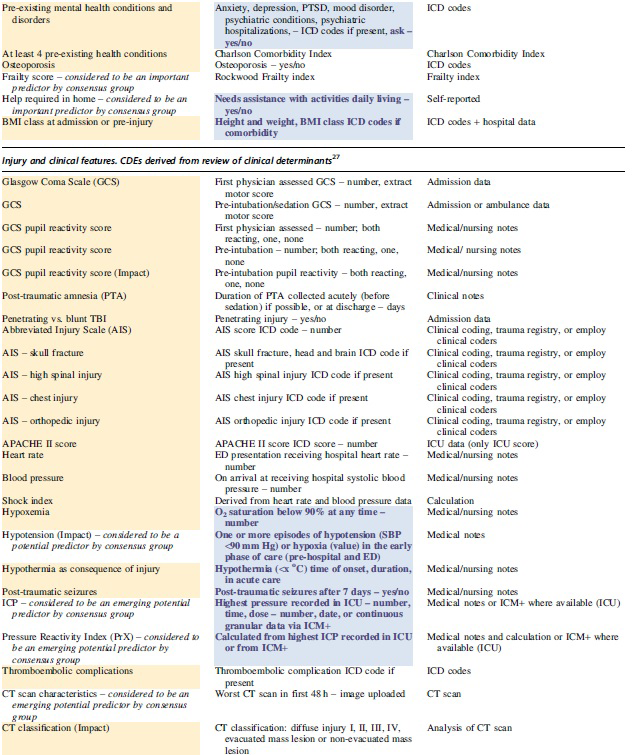
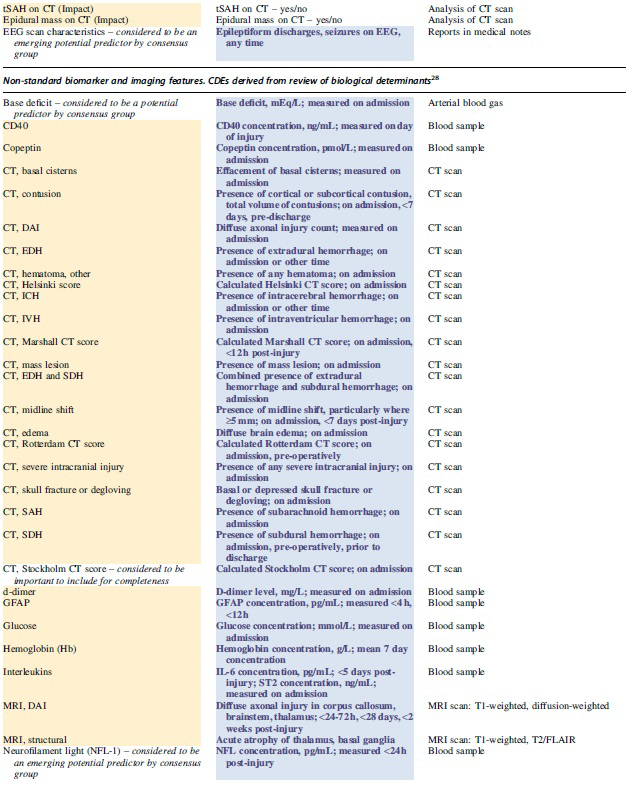
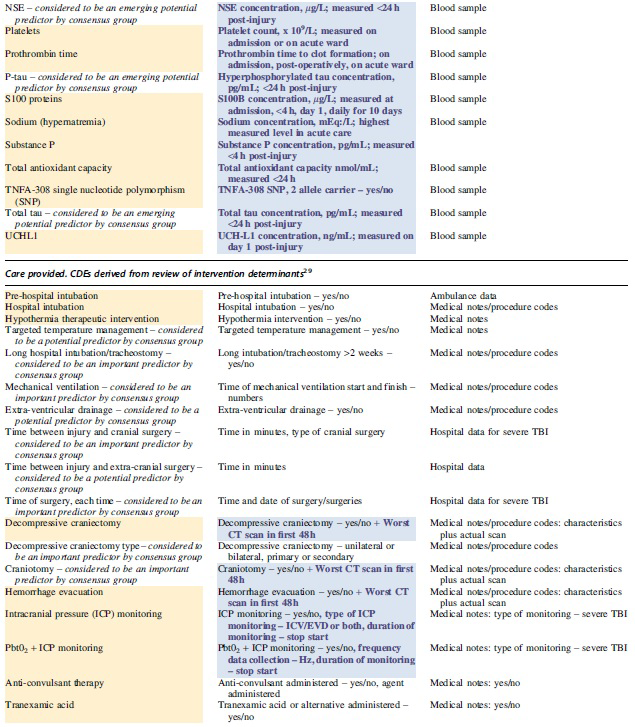
In addition to demographic elements that may predict outcome, additional demographic elements are included to facilitate analytical logistics, including data linkage. Features of care, such as length of stay, are included to facilitate comparative effectiveness research. The common data elements are grouped into areas of personal information, pre-hospital factors (social, article 2), pre-morbid conditions (health, article 3), injury and clinical features (clinical, article 4), care provided (interventions, article 6), and non-standard biomarker and imaging features (biologicals, article 5). The dictionary lists each element name, the measure to be collected, and the means of collection within the Australian context. Additional measures that were deemed to be important arising from conversations in steering committee meetings and by clinicians and researchers in facilitated consensus group meetings are included in the single data dictionary, separately color-coded to allow delineation from those measures arising from systematic reviews. The reason for inclusion of each additional measures is provided in column 1 of Table 1.
As noted above, a data dictionary fully reflecting Aboriginal and Torres Strait Islander perspectives requires further time and careful consideration as recommended by the Aboriginal and Torres Strait Islander Advisory Committee. This is acknowledged as a necessary ongoing body of work, the principles of which are defined below.
Key messages from consultation with the Lived Experience Expert Group
The consultations with the Lived Experience Expert Group provided insights on the merits and considerations regarding the nature of data elements for some of the study areas, as well as general principles to guide the collection of data and the selection of meaningful measures. The discussions were not focused on specific data elements, but they provided general insights as to the groups' perception of the importance of these types of measures and how best to collect them. The findings of these consultations are presented as a thematic collation prepared by the independent facilitator (RH) and EK. First, specific discussion points pertaining to each study area and regarding issues of ethics and consent are summarized. General conclusions are drawn, and these are collated into five principles to guide this and other similar studies.
Social study area: Information about personal support for the person with TBI
The amount, quality, and timing of information received by the person with TBI and/or their family is important for recovery. Information may not be remembered or may be poorly understood. Tailored and sensitive delivery is important. People with TBI and their families often feel left to cope alone after leaving the hospital, which is a difficult period of time. Having access to personally relevant and comprehensible information is important.
The timing, method, and wording used to ask questions about the support provided by family and/or close others prior to the injury and post-injury should take into account diverse social situations. It was noted that people may not have a “loved one” to “love and care” for them, so asking about this topic may trigger negative emotions. The Lived Experience Expert Group considered it better to use words such as “support” and “advocate,” which could refer to support sources other than close family.
Health study area: Information about medical history
The way questions are asked at the early stage following TBI requires excellent interpersonal skills and understanding of TBI. Family and friends will remember details of the acute care setting and experience and may be disturbed if seemingly inappropriate questions are asked at such a critical time. The level of detail required about this time should be carefully considered and, if significant detail is required, supporting information about the study will be helpful in assisting participants to understand the importance of providing these data.
Biological study area: Additional samples
The Lived Experience Expert Group noted that it would be acceptable to request additional biological samples to be taken (e.g., blood samples) if it was made clear how the data and results would be used. Any risk to the person with TBI arising from additional testing must be made clear to the participant or family. It would be preferable to ensure that any findings are useful for clinical care by making them available to the regular practitioner if feasible. Providing feedback to the participants about these results is very important.
Interventions study area: Information about treatment for the TBI
The group also considered that it would be acceptable to gather information about the treatment provided by the hospital because this information is important to recovery. It confirmed that the delivery of appropriate care at the appropriate time is important for return to work/study. The group described how new problems may continue to surface over time, so treatment information may be relevant to different people at different times. Support networks with other people who have experienced similar injuries can be helpful because treatment information can be shared. Formal support often stops abruptly on discharge from the hospital, so ongoing peer-to-peer support and social networks and social media groups can provide much needed ongoing information about treatment, contributing significantly to recovery.
Considerations regarding ethics and consent
The Lived Experience Expert Group emphasized that it was not appropriate for the group to be viewed as representative of all people with TBI. Nevertheless, some valuable insights were offered that the group believed could be universally useful. The group noted that it is particularly important that the participant derives value from the data collection process and results. Data collected needs to be personally meaningful and helpful for the person themselves. It must also be emphasized that answers to questions collected for the study will not affect the care received by the person with TBI.
The group also noted that existing family conflict can be exacerbated by the pressure of TBI. Thus, it is important to ensure that the person providing consent and contributing data is the most appropriate person to do so from the perspective of the injured person.
Conclusions and Principles from the Lived Experience Expert Group
The consultation process and independent analysis of key messages identified six general conclusions that can guide decision-making about how to conduct research with people who have TBI. The consultation also revealed five important principles that should guide TBI research.
People with TBI can appreciate the importance of research if its purpose and potential benefit are carefully explained using easy-to-understand English and accessible formats. The benefit of the research project for individuals and people with TBI should be thoroughly considered and explored with people who have lived experience, prior to beginning data collection.
The need for comparisons to pre-injury status is understood. People with TBI understand that family members may have a different perspective from theirs, but neither perspective is necessarily correct in response to this complex issue. This type of questioning must be handled with sensitivity to avoid distress of all parties.
Data should be collected using multiple methods to allow people choices about how they respond. Due to fatigue or preference, people may elect to change methods during the data collection process and this option must be made available.
Following a traumatic event such as TBI, all questions have the potential to raise uncomfortable and distressing emotions, particularly comparisons with the past, speculations about the future, or questions about social supports and family relationships. People with TBI do not believe these questions should be avoided, but they need to be asked sensitively and in the context of a supportive interaction. Time must be taken to develop rapport with participants, allowing sensitive information to emerge at the participant's own pace and with dignity.
Particular words can become triggers for emotional responses, and therefore words should be chosen carefully. Consideration needs to be given to words that imply a particular type of relationship, social situation, or status, noting that circumstances following TBI can be complex, family relationships and friendships can be strained, living arrangements may be suboptimal, and participation in life events can be restricted. All wording should be checked for assumptions.
Data collection should include consideration of the potential need for post-interview support, and this should be discussed with participants prior to beginning. Timing of data collection should consider the presence of supports, other activities required of the person on the day, and other events currently happening in the individual's life.
Five key principles represented the values people with TBI wanted to experience when participating in research. Each of these values should be checked against the proposed data collection process.
Principle 1
Continuity and Person-Centeredness: The importance of knowing the person before the injury and focusing on the uniqueness of each person rather than generalizing is emphasized. The assessment needs to be contextual, deeply embedded in the life of the person, and include attention to their passions, interests, work-related skills and experiences, and other health concerns. It is also crucial to consider the time of life and situation of the person and involve family members in the assessment process.
Principle 2
Emotional and Psychological Considerations: There is a clear distinction between physical and psychological data, with physical data having less emotional attachment, but psychological recovery having significant implications for participants and requiring adequate support systems. Probing psychological recovery may be upsetting, so assessment must be appropriate and questions must be asked in an appropriate manner because these conversations can influence recovery.
Principle 3
Supportive Context and Advocacy: The supportiveness of the assessment context is important, and the presence of an approved advocate who can speak for the person and provide support and care should be considered. It is also important to ensure that people do not fall through gaps and to follow up with action after the assessment (i.e., a research assessment implies a moral responsibility).
Principle 4
Information and Communication: Participants valued the combination of education with research, adequate follow-up, and ensuring that the information collected is consistent with other data sources to ensure translatability and minimize repeated data collection. It is crucial to assess the knowledge and skill levels in the family. Information must be simplified and written down for families, and people should be allowed to write notes during assessments, regardless of whether they are for clinical care or for research.
Principle 5
Timing and Format: The timing and format of the assessments should be tailored to the needs of the individual, with the length of the assessment depending on factors such as recovery status, fatigue, and concentration. Face-to-face, online, or survey formats are recommended, with the survey being quick and easy but not too wordy, including graphics and enhancing usability where possible. The telephone is not a preferred method of communication as it can be hard to concentrate.
In summary, it is important for researchers to take note of the main themes that emerged from the Lived Experience Expert Group in this study. Most importantly, it is essential to understand the unique circumstances and needs of the individual being assessed through supportive and respectful practices that focus on the person in their context and consider both physical and psychological aspects of recovery. Family members can provide valuable information and support during the assessment process. However, the recovery status of each individual should be considered when determining the time spent on assessment and a range of options should be available. It is also important to provide clear follow-up and share information, so participants feel assessment was useful to their own progress.
Key messages from consultation with the Aboriginal and Torres Strait Islander Advisory Group
The Aboriginal and Torres Strait Islander Advisory Group met and considered the proposed AUS-TBI data and collection approach with the assistance of an independent Aboriginal facilitator. The Aboriginal and Torres Strait Islander Advisory Group comprised the Aboriginal and Torres Strait Islander Chief and Associate Investigators in the AUS-TBI national consortium, as well as colleagues of EA, totaling 10 people, 8 females and 2 males. A number of key points and considerations for the project approach specific to Aboriginal and Torres Strait Islander peoples arose from the discussion and were collated by MF and BA, then reviewed for accuracy by the Advisory Group. These are outlined below in the form of principles that have also been reviewed by the group. The Advisory Group noted that the data dictionary to date reflects largely a Western-medicine-based model that may not yet incorporate Aboriginal and Torres Strait Islander perspectives on health, recovery, and social and emotional well-being. Development of the current approach to incorporate these perspectives requires further careful and detailed consideration.
Over time, the approach will result in validated potential predictive indicators that may include measures identified in the single data dictionary in Table 1 and/or that may replace measures with those that better suit Aboriginal and Torres Strait Islander peoples, and that may add deeper insights into TBI recovery for all TBI survivors. The principles outlined below provide a start to this process and reflect the Advisory Group's initial recommendations regarding culturally sensitive methodologies and ways of managing data that align with Aboriginal and Torres Strait Islander data sovereignty principles. The principles were:
Principle 1
Data sovereignty principles33–35
must be followed, and governance must be led by Aboriginal and Torres Strait Islander researchers and relevant community leaders. Examples include:
The way(s) in which Aboriginal and Torres Strait Islander status will be identified and cross-referenced should be determined. Data from Aboriginal and Torres Strait Islander peoples must be managed and analyzed in collaboration with Aboriginal and Torres Strait Islander people so as not to reinforce a deficit focus and a deficit narrative in subsequent research articles and policies. There is an onus on non-indigenous researchers to develop their skills and understanding of data sovereignty so that indigenous involvement in research is not limited to the auditing and advising on the appropriateness or otherwise of proposed approaches. Data must be shared back with the Aboriginal and Torres Strait Islander communities it has been derived from and used in ways led by Aboriginal and Torres Strait Islander peoples.
Principle 2
The type of data collected and the way(s) in which it is collected should be considered from a cultural perspective:
Questions must be tailored not to cause shame (e.g., household income questions).
Carefully consider how the data will be analyzed and whether certain questions should be asked of Aboriginal and Torres Strait Islander peoples.
Some proposed data types and questions may be too intrusive for Aboriginal and Torres Strait Islander participants—especially on first meeting.10,12 These should be carefully revised.
Date of injury and other injury details are often not available if recruitment occurs outside of the hospital context—methodology must be considered to ensure data accuracy.
Principle 3
Clinical yarning, which involves sharing experiences through conversation to create new knowledge36,37 should be the core approach to data collection and follow-up. The value of clinical yarning has been evidenced well through other projects such as the Healing Right Way trial 38 or the Guddi Way Screen 22 and time should be taken to investigate how this methodology could be incorporated into the data collection so as to best serve the aims of the project.
Principle 4
Embedding Aboriginal and Torres Strait Islander research assistants/officers within hospitals is needed to ensure the right people are there to both liaise with and support patients on their journey. The research assistants/officers would work with patients by yarning and gathering information over time.
Principle 5
Further cultural training for non-Aboriginal and Torres Strait Islander staff within the hospital system is needed so that staff are better able to care for Aboriginal and Torres Strait Islander peoples with TBI, while respecting their cultural rights, values, and expectations.
Principle 6
Address racism. All stakeholders involved in the project need to call out racism that is happening across the clinical and care setting for Aboriginal and Torres Strait Islander peoples with TBI (overarching principle).
Implementation of AUS-TBI
The Australian Government Mission for TBI has funded the current design process for AUS-TBI, through the Australian Medical Research Future Fund. The Implementation Plan for the Mission for TBI includes a large-scale project to implement optimal informatics approaches nationally that maximize ongoing data collection and linkage, to facilitate personalization of care and improved outcomes.
To guide this project, the AUS-TBI consortium has designed a single data dictionary consisting of common data elements (AUS-TBI CDEs) that are potentially predictive of clinical and long-term outcomes following TBI. Some of the AUS-TBI CDEs are routinely collected via multi-sectoral administrative data sets, whereas others will require bespoke data collection approaches. These elements and their measures were prioritized based on previous demonstration of predictive potential and consensus among clinicians, researchers, and people with lived experience of TBI. Only six of the studies identified in the systematic review of methodologies to identify common data elements (article 1 of the series) included consultation with people with lived experience of that neurological affliction. Of these, only one reported detailed findings of that consultation as a thematic analysis. 39 The AUS-TBI design process included careful consideration of the views of people with lived experience of TBI about how data should be collected. The data dictionary is accompanied by a set of guiding principles that will be fundamental to the ongoing health informatics approach and of value to other similar approaches in related conditions.
Data collection will require careful consideration of consent and data sovereignty, data governance ethics and privacy, data collection methodologies, data storage, data management, data linkage, and data access for analysis. The principles derived from the consultation described here will be followed and the AUS-TBI Consumer Advisory Group will regularly contribute to further iterative data methodology development. The AUS-TBI team is currently considering these matters together with multiple partner organizations, in light of the legislative, regulatory, and governance environment in Australia. The FAIR principles of Findable, Accessible, Interoperable, and Reusable will be adopted to ensure that the value of data to be collected is maximized. Likely uses of the data will be considered to ensure appropriate methodologies of access are recommended, considering a range of methodologies for data analysis including machine learning,40,41 to ensure formats and access parameters are suitable, including for imaging data. The AUS-TBI consortium plans to apply machine learning to the data collected, to develop accurate prediction models aimed at reducing TBI mortality and morbidity.
The Aboriginal and Torres Strait Islander Peoples Advisory Group will exercise control over the data systems that collect data from Aboriginal and Torres Strait Islander peoples, in line with indigenous data protocols such as the Lowitja Data Sovereignty Principles. 42 If enacted, the AUS-TBI informatics approach will facilitate international interdisciplinary TBI research that addresses the needs of consumers including Aboriginal and Torres Strait Islander peoples, through genuine co-design and culturally secure methodologies. For the AUS-TBI approach to succeed there will need to be considerable investment to support the bespoke data collection needed for novel potentially predictive indicators not collected via existing mechanisms. Researchers will be needed to extract data from clinical records and for some elements, to ask questions of patients or their close others. Collection of sensitive information from Aboriginal and Torres Strait Islander people will require labor-intensive clinical yarning-based methods for the data to be meaningful. Data linkage will facilitate data collection, but governance restrictions differ between Australian jurisdictions and may limit production of a complete data set. Cleaning of the data set will be required prior to application of machine learning, which may be costly if data collection systems are suboptimal. It will therefore be critical to ensure that the data collection approach is practical and pragmatic, maximizing automation to limit human error and variance in reporting.
AUS-TBI data will be designed to be analyzed using deep-learning techniques to generate novel and effective predictive algorithms for personalizing care. More accurate and individual patient-specific prognostication is critical for counseling patients and families of people with TBI. If enacted, the AUS-TBI data resource will be used to generate algorithms that will ideally enable patients to be classified according to treatments to which they will best respond, enabling early initiation of tailored interventions that can maximize outcomes. Individuals will be contacted by phone to assess long-term outcomes (series article 7), and there are plans to extend the duration of follow-up for as long as funding permits.
The use of algorithms may automatically disadvantage underrepresented groups including but not limited to Aboriginal and Torres Strait Islander peoples, culturally and linguistically diverse people, and other intersections such as rural/remote and LGBTQI+. Deliberate oversampling from underrepresented groups may be needed to generate separate algorithms to prevent bias. Through strong governance AUS-TBI will ensure AI algorithms do not perpetuate or amplify existing health disparities and inequalities and will be guided by ethical principles that prioritize equity. The informatics approach can also serve as the data backbone for integrating multiple trials of treatments and intervention, enabling robust, cost-effectiveness evaluations of alternate models of care or interventions in an adaptive trial design. Use of common data elements and outcome measures across Australian studies will minimize duplication and burden for patients and families and allow benchmarking and comparisons of cost-effectiveness between trials, with the ultimate aim of improving outcomes and quality of life for people with TBI.
Transparency, Rigor, and Reproducibility Summary
This study is a summary and perspectives piece of a series of eight systematic reviews. The rigor and process for each review are reported individually. Further information is available at the discretion of the corresponding author.
AUS-TBI Initiative Investigators
Tara Alexander, Australasian Rehabilitation Outcomes Centre & Australian Health Services Research Institute, Faculty of Business and Law, University of Wollongong, Wollongong, New South Wales, Australia; Vicki Anderson, Psychology Service, The Royal Children's Hospital, Melbourne, Victoria, Australia; Clinical Sciences Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Ana Antonic-Baker, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Elizabeth Armstrong, School of Medical and Health Sciences, Edith Cowan University, Perth, Western Australia, Australia; Franz E. Babl, Department of Emergency Medicine, The Royal Children's Hospital, Melbourne, Victoria, Australia; Departments of Paediatrics and Critical Care, University of Melbourne, Melbourne, Victoria, Australia; Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Matthew K. Bagg, Curtin Health Innovation Research Institute, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; School of Health Sciences, University of Notre Dame Australia, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Perth, Western Australia, Australia; Centre for Pain IMPACT, Neuroscience Research Australia, Sydney, New South Wales, Australia; Zsolt J. Balogh, Department of Traumatology, John Hunter Hospital and University of Newcastle, Newcastle, New South Wales Australia; Karen M Barlow, Acquired Brain Injury in Children Research Program, Queensland Children's Hospital, Brisbane, Queensland, Australia; Centre for Children's Health Research, University of Queensland, Brisbane, Queensland, Australia; Judith Bellapart, Department of Intensive Care Services, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Faculty of Medicine, University of Queensland, Brisbane, Queensland, Australia; Niranjan Bidargaddi, Flinders Digital Health Centre, College of Medicine & Public Health, Flinders University, Adelaide, South Australia, Australia; Erika Bosio, Centre for Clinical Research in Emergency Medicine, Harry Perkins Institute of Medical Research, Perth, Western Australia, Australia; School of Biomedical Science & School of Medicine, University of Western Australia, Perth, Western Australia, Australia; Peter Bragge, BehaviourWorks Australia, Monash Sustainable Development Institute, Monash University, Melbourne, Victoria, Australia; Michael Bynevelt, School of Surgery, The University of Western Australia, Perth, Western Australia, Australia; Neurological Intervention and Imaging Service of Western Australia, Sir Charles Gairdner Hospital, Perth, Western Australia, Australia; Karen Caeyenberghs, Cognitive Neuroscience Unit, School of Psychology, Deakin University, Geelong, Victoria, Australia; Peter A. Cameron, National Trauma Research Institute, Melbourne, Victoria, Australia; School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Emergency and Trauma Centre, The Alfred Hospital, Melbourne, Victoria, Australia; Jacquelin Capell, Australasian Rehabilitation Outcomes Centre & Australian Health Services Research Institute, Faculty of Business and Law, University of Wollongong, Wollongong, New South Wales, Australia; Kevin E.K. Chai, School of Population Health, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Curtin Institute for Computation, Curtin University, Perth, Western Australia, Australia; Lyndsey E. Collins-Praino, School of Biomedicine, University of Adelaide, Adelaide, South Australia, Australia; D.J. Jamie Cooper, Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Department of Intensive Care and Hyperbaric Medicine, The Alfred, Melbourne, Victoria, Australia; Gill Cowen, School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Louise M. Crowe, Clinical Sciences Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Victoria, Australia; Tim Cudmore, AUS-TBI Lived Experience Advisory Group; Jennifer Cullen, Synapse, Brisbane, Queensland, Australia; James Cook University, Townsville, Queensland, Australia; Menzies Health Institute Queensland, Griffith University, Brisbane, Queensland, Australia; Kate Curtis, Susan Wakil School of Nursing and Midwifery, Faculty of Medicine and Health, The University of Sydney, New South Wales, Australia; Illawarra Shoalhaven Local Health District, Wollongong, New South Wales, Australia; Illawarra Health and Medical Research Institute, Wollongong, New South Wales, Australia; George Institute for Global Health, Sydney, New South Wales, Australia; Anthony Delaney, Division of Critical Care, The George Institute for Global Health, Sydney, New South Wales, Australia; Malcolm Fisher Department of Intensive Care Medicine, Royal North Shore Hospital, Sydney, New South Wales, Australia; Northern Clinical School, Sydney Medical School, University of Sydney, Sydney, New South Wales, Australia; Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria Australia; Graeme Dibdin, AUS-TBI Lived Experience Advisory Group; Sandra Eades, Centre for Epidemiology and Biostatistics, Melbourne School of Population and Global Health, University of Melbourne, Melbourne, Victoria, Australia; School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Gary F. Egan, Monash Biomedical Imaging & School of Psychological Sciences, Monash University, Melbourne, Victoria, Australia; Daniel Y. Ellis, Department of Trauma, Royal Adelaide Hospital, Adelaide, South Australia, Australia; Statewide South Australian Trauma Service, South Australia, Australia; School of Public Health and Tropical Medicine, James Cook University, Queensland, Australia; Ari Ercole, Division of Anaesthesia, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Cambridge Centre for AI in Medicine, University of Cambridge, United Kingdom; Daniel M. Fatovich, Emergency Medicine, Royal Perth Hospital, University of Western Australia, Perth, Western Australia, Australia; Centre for Clinical Research in Emergency Medicine, Harry Perkins Institute of Medical Research, Perth, Western Australia, Australia; Murray J. Fisher, Susan Wakil School of Nursing and Midwifery, Faculty of Medicine and Health, University of Sydney, New South Wales, Australia; Royal Rehab, Ryde, Sydney, New South Wales, Australia; Mark Fitzgerald, National Trauma Research Institute, Melbourne, Victoria, Australia; Melinda Fitzgerald, Curtin Health Innovation Research Institute, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Perth, Western Australia, Australia; Jennifer Fleming, School of Health and Rehabilitation Sciences, The University of Queensland, Brisbane, Queensland, Australia; Roslyn Francis, Department of Health, Government of Western Australia, Perth, Western Australia, Australia; Belinda J. Gabbe, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Health Data Research UK, Swansea University Medical School, Swansea University, Singleton Park, United Kingdom; Adelle Gadowski, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; John Gilroy, Aboriginal and Torres Strait Islander Research, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Mitchell A. Hansen, Department of Neurosurgery, John Hunter Hospitals and University of Newcastle, Newcastle, New South Wales, Australia; James E. Harrison, College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia; Luke J. Haseler, Curtin Health Innovation Research Institute, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Leanne Hassett, Institute for Musculoskeletal Health & Sydney School of Health Sciences, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Sydney Local Health District, Sydney, New South Wales, Australia; Sarah C. Hellewell, Curtin Health Innovation Research Institute & School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Nedlands, Western Australia, Australia; Amelia J. Hicks, School of Psychological Sciences, Monash University, Melbourne, Victoria, Australia; Monash Epworth Rehabilitation Research Centre, Epworth Healthcare, Melbourne, Victoria, Australia; Brain Injury Research Center, Icahn School of Medicine at Mount Sinai, New York City, New York, United States of America; Andrew F. Hill, College of Science, Health and Engineering, La Trobe University, Melbourne, Victoria, Australia; Andrew J.A. Holland, The Children's Hospital at Westmead Clinical School, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Stephen Honeybul, Department of Neurosurgery, Sir Charles Gairdner Hospital, Perth, Western Australia, Australia; Department of Neurosurgery, Royal Perth Hospital, Perth, Western Australia, Australia; Rosalind L. Jeffree, Kenneth G. Jamieson Department of Neurosurgery, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Royal Brisbane Clinical School, School of Medicine, University of Queensland, Brisbane, Queensland, Australia; Chris Joyce, Intensive Care Unit, Princess Alexandra Hospital, Brisbane, Queensland, Australia; School of Medicine, University of Queensland, Brisbane, Queensland, Australia; Elizabeth Kendall, The Hopkins Centre, Griffith University, Brisbane, Queensland, Australia; Kate King, John Hunter Trauma Service, John Hunter Hospital, Newcastle, New South Wales, Australia; College of Health, Medicine and Wellbeing, University of Newcastle, Newcastle, New South Wales, Australia; Natasha A. Lannin, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Alfred Health, Melbourne, Victoria, Australia; Meng Law, Departments of Neuroscience and Radiology, Monash University, Melbourne, Victoria, Australia; Alfred Health, Melbourne, Victoria, Australia; Alzheimer's Disease Research Center & Department of Neurological Surgery, Keck School of Medicine, University of Southern California, Los Angeles, California, United States of America; Andrew I.R. Maas, Department of Neurosurgery, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Adam Mahoney, Trauma Service, Royal Hobart Hospital, Hobart, Tasmania, Australia; 2nd General Health Battalion, Australian Defence Force; Peter Makin, AUS-TBI Lived Experience Advisory Group; Peter Mayhew, AUS-TBI Lived Experience Advisory Group); Alison McDonald (AUS-TBI Lived Experience Advisory Group; Skye McDonald, School of Psychology, University of New South Wales, Sydney, New South Wales, Australia; Stuart J. McDonald, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Ancelin McKimmie, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Robert McNamara, Department of Intensive Care Medicine, Royal Perth Hospital, Perth, Western Australia, Australia; School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Shiv Meka, Department of Health, Government of Western Australia, Perth, Western Australia, Australia; David K. Menon, Division of Anaesthesia, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Wolfson Brain Imaging Centre, University of Cambridge, Cambridge, United Kingdom; Gary Mitchell, Emergency and Trauma Unit, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Royal Brisbane Clinical Unit, University of Queensland, Brisbane, Queensland, Australia; Jamieson Trauma Institute, Brisbane, Queensland, Australia; Queensland Rugby Union; Brisbane, Queensland, Australia; Rowena Mobbs, Brain & Mind Centre, University of Sydney, Sydney, New South Wales, Australia; Macquarie University, Sydney, New South Wales, Australia; Fatima A. Nasrallah, Queensland Brain Institute, University of Queensland, Brisbane, Queensland, Australia; Virginia F.J. Newcombe, PACE Section, Department of Medicine, Addenbrooke's Hospital, University of Cambridge, Cambridge, United Kingdom; Terence J. O'Brien, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; John H. Olver, Epworth Healthcare, Melbourne, Victoria, Australia; Department of Medicine, Monash University, Melbourne, Victoria, Australia; Gerard M. O'Reilly, National Trauma Research Institute, Melbourne, Victoria, Australia; Emergency and Trauma Centre, The Alfred Hospital, Melbourne, Victoria, Australia; School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Tamara Ownsworth, The Hopkins Centre, Griffith University, Brisbane, Queensland, Australia; School of Applied Psychology, Griffith University, Brisbane, Queensland, Australia; Paul M. Parizel, University of Antwerp, Edegem, Belgium; Department of Radiology, Royal Perth Hospital & University of Western Australia, Perth, Western Australia, Australia; West Australian National Imaging Facility Node, Perth, Western Australia, Australia; Michael Parr, Intensive Care Unit, Liverpool Hospital, University of New South Wales, Sydney, New South Wales, Australia; Intensive Care Unit, Macquarie University Hospital, Macquarie University, Sydney, New South Wales, Australia; Jennie L. Ponsford, School of Psychological Sciences, Monash University, Melbourne, Victoria, Australia; Monash Epworth Rehabilitation Research Centre, Epworth Healthcare, Melbourne, Victoria, Australia; Bruce Powell, AUS-TBI Lived Experience Advisory Group; Patricia Ratajczak, AUS-TBI Lived Experience Advisory Group; Michael C. Reade, Faculty of Medicine, University of Queensland, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Joint Health Command, Australian Defence Force, Canberra, Australian Capital Territory, Australia; Sandy Reeder, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Christopher Reid, School of Public Health, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Julia Robertson, AUS-TBI Lived Experience Advisory Group; Suzanne Robinson, School of Population Health, Faculty of Health Sciences, Curtin University, Perth Western Australia, Australia; Stephen E. Rose, The Australian e-Health Research Centre, Commonwealth Scientific and Industrial Research Organisation, Brisbane, Queensland, Australia; Jeffrey V. Rosenfeld, Department of Neurosurgery, The Alfred Hospital, Melbourne, Victoria, Australia; Department of Surgery, Monash University, Melbourne, Victoria, Australia; F. Edward Hébert School of Medicine, Uniformed Services University of The Health Sciences, Bethesda, Maryland, United States of America; Jason P. Ross, Molecular Diagnostic Solutions, Health and Biosecurity, Commonwealth Scientific and Industrial Research Organisation, Australia; Danette Rowse, AUS-TBI Lived Experience Advisory Group; Nick Rushworth, Brain Injury Australia, Sydney, New South Wales, Australia; Adam Scheinberg, Neurodevelopment and Rehabilitation Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Victoria, Australia; Bridgette D. Semple, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Alfred Health, Melbourne, Victoria, Australia; Department of Medicine, Royal Melbourne Hospital, The University of Melbourne, Melbourne, Victoria, Australia; Sandy R. Shultz, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Grahame K. Simpson, Brain Injury Rehabilitation Research Group, Ingham Institute for Applied Medical Research, Sydney, New South Wales, Australia; John Walsh Centre for Rehabilitation Research, Sydney School of Medicine, University of Sydney, Sydney, New South Wales, Australia; Warwick J. Teague, Trauma Service & Department of Paediatric Surgery, The Royal Children's Hospital, Melbourne, Victoria, Australia; Surgical Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Victoria, Australia; Leanne Togher, Speech Pathology, School of Health Sciences, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Andrew A. Udy, Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Department of Intensive Care and Hyperbaric Medicine, The Alfred Hospital, Melbourne, Victoria, Australia; Kirsten Vallmuur, Centre for Healthcare Transformation, Australian Centre for Health Services Innovation, Queensland University of Technology, Brisbane, Queensland, Australia; Jamieson Trauma Institute, Brisbane, Queensland, Australia; Dinesh Varma, Department of Radiology, The Alfred Hospital, Melbourne, Victoria, Australia; Department of Surgery, Monash University, Melbourne, Victoria, Australia; National Trauma Research Institute, Melbourne, Victoria, Australia; James Vickers, Wicking Dementia Research and Education Centre, College of Health and Medicine, University of Tasmania, Hobart, Tasmania, Australia; Janet Wagland, Brightwater Group, Perth, Western Australia, Australia; James Walsham, Intensive Care Unit, Princess Alexandra Hospital, Brisbane, Queensland, Australia; School of Medicine, University of Queensland, Brisbane, Queensland, Australia; Adam J. Wells, Department of Neurosurgery, Adelaide Hospital, Adelaide, South Australia, Australia; Department of Surgery, University of Adelaide, Adelaide, South Australia, Australia; Neurosurgical Research Foundation, Adelaide, South Australia, Australia; Luke Whiley, Health Futures Institute, Murdoch University, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Perth, Western Australia, Australia; Gavin Williams, Department of Physiotherapy, Epworth Healthcare, Melbourne, Victoria, Australia; Department of Physiotherapy, University of Melbourne, Melbourne, Victoria, Australia; Jodie K. Williams, National Critical Care and Trauma Response Centre, Royal Darwin Hospital, Darwin, Northern Territory, Australia; Roslind Witham, AUS-TBI Lived Experience Advisory Group; David K. Wright, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Louise York, Australian Institute of Health and Welfare, Canberra, Australian Capital Territory, Australia; Jesse T. Young, Centre for Health Equity, Melbourne School of Population and Global Health, The University of Melbourne, Melbourne, Victoria, Australia; Centre for Adolescent Health, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; School of Population and Global Health, University of Western Australia, Perth, Western Australia, Australia; National Drug Research Institute, Curtin University, Perth, Western Australia, Australia; Heidi Zeeman, The Hopkins Centre, Griffith University, Brisbane, Queensland, Australia.
Footnotes
Author Disclosure Statement
MKB has received personal fees for travel or consulting from Chiropractor's Association of Australia, Memorial University of Newfoundland, Life Ready Health Group, and Active Linc Pty. Ltd. MKB has received research funding from the Australian National Health and Medical Research Council, MRFF, and Research Training Program schemes, University of New South Wales, and Neuroscience Research Australia. DJC occasionally consults to Pressura Neuro, all funds to Monash University. MF is the CEO of the charitable organization Connectivity-Traumatic Brain Injury Australia.
Funding Information
This work is funded by the Australian Government's Medical Research Future Fund (MRFF), ID2008223. The funder had no role in study design, data collection and analysis, data interpretation and manuscript writing, or the decision to submit the article for publication.
Authors' Contributions
Melinda Fitzgerald: conceptualization, funding acquisition, methodology, project administration, supervision, writing—review and editing; Jennie L. Ponsford: conceptualization, funding acquisition, methodology, writing—review and editing; Regina Hill: conceptualization, methodology, writing—review and editing; Nick Rushworth: conceptualization, funding acquisition, methodology, writing—review and editing; Elizabeth Kendall: conceptualization, funding acquisition, methodology, writing—review and editing; Elizabeth Armstrong: conceptualization, funding acquisition, methodology, writing—review and editing; John Gilroy: conceptualization, funding acquisition, methodology, writing—review and editing; Jonathon Bullen: conceptualization, funding acquisition, methodology, writing—review and editing; Jemma Keeves: methodology, project administration, resources, data curation, formal analysis, writing—review and editing; Matthew K. Bagg: methodology, project administration, writing—review and editing; Sarah C. Hellewell: methodology, funding acquisition, writing—review and editing; Natasha A. Lannin: conceptualization, funding acquisition, methodology, writing—review and editing; Terence J. O'Brien: conceptualization, funding acquisition, methodology, writing—review and editing; Peter A. Cameron: conceptualization, funding acquisition, methodology, writing—review and editing; D. Jamie Cooper: conceptualization, funding acquisition, methodology, writing—review and editing; Belinda J. Gabbe: conceptualization, funding acquisition, methodology, writing—review and editing; AUS-TBI Investigators: conceptualization, writing—review and editing.