
Abstract
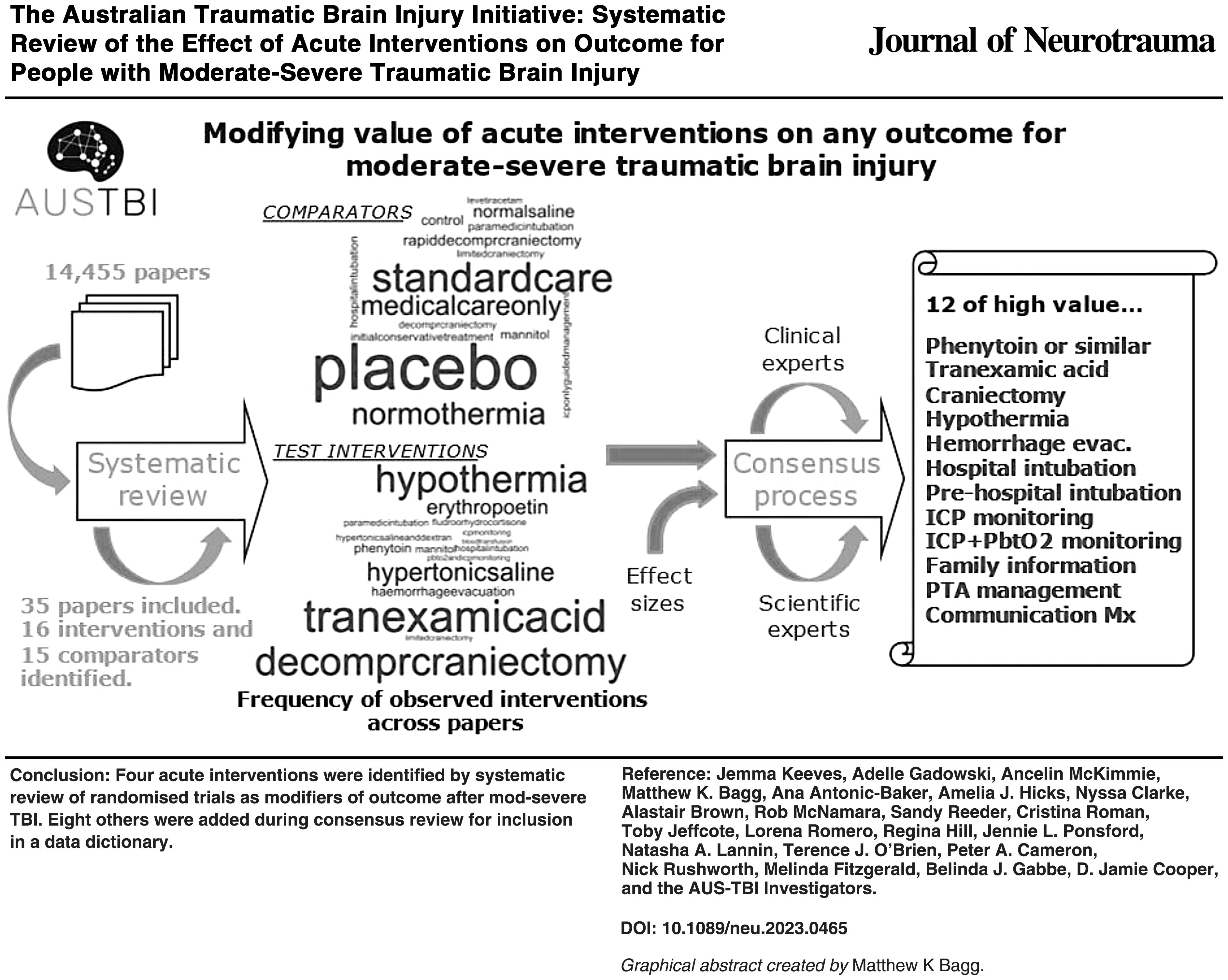
The Australian Traumatic Brain Injury Initiative (AUS-TBI) is developing a data resource to enable improved outcome prediction for people with moderate-severe TBI (msTBI) across Australia. Fundamental to this resource is the collaboratively designed data dictionary. This systematic review and consultation aimed to identify acute interventions with potential to modify clinical outcomes for people after msTBI, for inclusion in a data dictionary. Standardized searches were implemented across bibliographic databases from inception through April 2022. English-language reports of randomized controlled trials (RCTs) evaluating any association between any acute intervention and clinical outcome in at least 100 patients with msTBI, were included. A predefined algorithm was used to assign a value to each observed association. Consultation with AUS-TBI clinicians and researchers formed the consensus process for interventions to be included in a single data dictionary. Searches retrieved 14,455 records, of which 124 full-length RCTs were screened, with 35 studies included. These studies evaluated 26 unique acute interventions across 21 unique clinical outcomes. Only 4 interventions were considered to have medium modifying value for any outcome from the review, with an additional 8 interventions agreed upon through the consensus process. The interventions with medium value were tranexamic acid and phenytoin, which had a positive effect on an outcome; and decompressive craniectomy surgery and hypothermia, which negatively affected outcomes. From the systematic review and consensus process, 12 interventions were identified as potential modifiers to be included in the AUS-TBI national data resource.
Keywords
Introduction
Traumatic brain injury (TBI) is a common cause of morbidity and mortality in both high- and low-income countries. 1 Despite decades of research, less than 50% of patients with severe TBI are fully independent 6 months after injury, resulting in significant health care and socioeconomic burden globally.2–4 Due to the various causes and severities of TBI, acute management can be challenging and heterogeneous, particularly if an individual also has other complex injuries. Prognostic models and algorithms derived from multiple, large observational data sets have been developed for moderate-severe TBI (msTBI) to guide clinical decision-making; however, they are not sufficiently accurate for clinical use at an individual patient level. 5
Acute phase medical and surgical management of msTBI aims to minimize secondary brain injury and to improve individual patient outcomes. 6 Common pre-hospital and in-hospital interventions and surgical procedures include airway management, such as intubation; mechanical ventilation; sedation; intracranial pressure (ICP) monitoring; hypertonic infusions (mannitol/hypertonic saline); hypothermia; and neurosurgery, including extra-ventricular drain insertion, hematoma evacuation, and decompressive craniectomy. Other pharmacological interventions include anticonvulsants as prophylaxis of post-traumatic seizures, and tranexamic acid to reduce bleeding after traumatic hemorrhage. Despite these interventions being widely used in clinical practice and often reported in TBI research, efficacy varies, and there is little synthesized evidence to determine which interventions have most modified outcomes in people with msTBI. The aims of this systematic review were to synthesize the evidence describing acute interventions as evaluated by included trials, and to rank the likelihood that interventions had modified clinical outcomes.
The Australian Traumatic Brain Injury (AUS-TBI) Initiative seeks to improve prediction, health care, and outcomes for people with msTBI. 7 A key output is the data dictionary, compiled through consensus processes across six study areas: (1) demographic, injury event, and social characteristics, (2) pre-existing health conditions, (3) the clinical experience, (4) biological mechanisms, (5) acute interventions, and (6) longer-term outcomes.8,9 Further to the systematic review, this article reports the subsequent consensus processes that occurred in the interventions study area. Accompanying articles in this series report the activities in the other five study areas, with a summative report of the data dictionary in the final article.
Methods
This systematic review was prospectively registered on PROSPERO (CRD42022298596). The study is reported herein with respect to the 2020 PRISMA statement. 10
Objectives
The objectives of the systematic review were:
To identify published, high-quality, randomized controlled trials (RCTs) of acute medical and surgical interventions for patients with msTBI. To identify the acute interventions evaluated in studies within the record set. To assign judgements for interventions likely (high/medium/low) to have modified any patient outcome either positively or negatively.
Outcomes
The primary outcome of the systematic review is the set of unique acute interventions that have been shown to positively or negatively affect patient outcome. Secondary outcomes are the set of unique clinical outcomes, and the set of unique studies.
Sampling
Standardized, piloted, search strategies were used to search Central, CINAHL, Embase, Emcare, Medline, Scopus, SportDiscus, and Web of Science from inception to April 2022. Full details of the standardized methodology followed for this review are described by Gabbe and colleagues 11 unless otherwise stated. Briefly, two independent team members screened the title and abstract of each record, resolving any disagreements through discussion and consultation with a third independent team member if required. Full-length texts were also screened in duplicate to confirm inclusion for data extraction.
Specific to this systematic review, initial database searching was conducted identifying all studies that were published in English-language reports evaluating relationships between acute interventions and clinical outcomes in at least 100 people with msTBI. We considered that trials with fewer than 100 participants could not have findings sufficiently rigorous to guide clinical practice or prognostic decision-making in the management of msTBI. 12 Following the title and abstract screening, to limit the review to high-quality trials likely to influence clinical practice, study designs other than RCTs were excluded. The acute interventions of interest to this study were any medication administered, or procedure performed, during the acute care phase. The acute care phase included the pre-hospital and acute inpatient settings (emergency department, intensive care unit, and ward). Extensive consultation with clinical experts in pharmacology occurred when developing the literature searches to refine and prioritize the medications relevant to trauma and TBI management. Clinical outcomes were considered broadly as any dependent variable reflective of the clinical features or lived experience of TBI. msTBI was defined as the medically confirmed presence of at least one of: (1) initial or lowest Glasgow Coma Scale (GCS) score less than 13, (2) post-traumatic amnesia duration greater than 24 h, or (3) abnormal findings on computed tomography (CT) imaging of the head. This operational definition may include the complicated-mild injury type.
As outlined by Gabbe and colleagues, 11 studies sampling participants without TBI or with mild, non-complicated TBI were only included if the data on participants with msTBI were reported separately from other participants, or if greater than 80% of the baseline sample were people with msTBI. Studies without clearly reported medical confirmation of msTBI were included on the expert clinical area judgement of the review team that medical confirmation would have necessarily occurred in the study context. There were no restrictions on demographic characteristics of individuals or injury circumstances.
Data extraction
The coordinating team members and AUS-TBI Steering Committee co-designed the data items (variables) for extraction from included study reports. Standardized data sheets were built in Google Sheets (GSuite, Monash University), piloted, then adapted to the requirements of this review. Detailed data extraction methods are described in the second article of this series by Gabbe and colleagues. 11 Briefly, the data items captured information on study characteristics, measured outcomes, studied interventions (in this review, acute medical or surgical interventions), measured comparator variables (only applicable for this review), measured baseline sample size, subgroups, covariate adjustment, and reported measures of effects. Study authors were not contacted to request missing data or to clarify uncertain data for this iteration of the review.
For each record, data were extracted by a single team member. Trials were excluded at the abstract stage if all results were negative. Expert judgement of the team member was used to identify only acute intervention:outcome associations meeting the aforementioned criteria. In this review, these was all associations between an acute intervention and any clinical outcome (primary or secondary) evaluated in each study. The standardized data sheets included additional data items that summarized or structured the information in the extracted data items. These were filled during the extraction process. Upon completion, the team member used a predefined decision algorithm (Sidebar 1) to guide assigning a judgement of effect size for each observed intervention:outcome association. The algorithm for modifying judgements was developed by authors MF and MKB, using their methodological and content area expertise. The judgement algorithm for this systematic review differed slightly from the other reviews in the series due to the different criteria for included studies, in particular, all studies were RCTs with a sample size greater than 100 participants. The strength of the modifying relationship was based on the extractor's statistical knowledge. Any uncertainties about modifying relationships were discussed with the study area lead.

Data management
Completed data sheets were locked to editing, mirrored to static versions on OneDrive (Microsoft 365), and read to R (version 4.3.1). Data were inspected for implausible and missing values, cleaned, then summarized, using the tidyverse. 13 Implausible values were replaced in the R object (i.e., operating data set), with recourse to the study report as required. The extent of missing values was calculated for each variable. Observations coded relevant to other study area reviews were parsed to the appropriate data set object. Categorical variables were summarized using the frequency of observations on each level. Variables that captured semi-structured text were coerced to factors (the categorical structure in R) and unique levels were identified through homogenization by the review team. Original free text was preserved. The subsequently “cleaned” data set was written out to .csv, with values locked to editing, and then sent to the independent external facilitator of the AUS-TBI consensus meetings. Word clouds were used to display the observed frequency of unique predictor interventions, comparators, and outcomes in all the included trials.
AUS-TBI consensus process
AUS-TBI integrates multiple stakeholders. The contributions of (1) clinicians and researchers, (2) people with lived experience, and (3) people identifying as Aboriginal or Torres Strait Islander were sought at distinct stages of development of the data dictionary. In this “Interventions” study area, clinicians and researchers were consulted following the systematic review to refine the list of observed interventions toward an up-to-date and feasible list of prospective items for the data dictionary. Approximately 20 clinician and researcher AUS-TBI members self-nominated to participate in this Interventions study area consensus process.
The consensus process was organized by two members of the AUS-TBI Initiative Steering Committee (MF, DJC). Consultation occurred in a real-time virtual meeting, facilitated by an external consultant. Participants were sent the results of the systematic review prior to attending the meeting. Participant input was collected using structured questioning, open discussion, and voting with the final score being the average of indices scored by attendees. Specific details of the consensus process and scoring system used are described in the second article of this series by Gabbe and colleagues. Following the meeting, the consultant cleaned the results and circulated them to participants for additional feedback and confirmation.
Differences between protocol and this iteration of the review
The protocol stated that all study types would be included in this review; however, after database searching, only RCTs were included to limit consideration to high-quality evidence that might influence practice. Also, the Joanna Briggs Institute data extraction tools were not used in this review. In practice, a bespoke extraction tool was developed by the AUS-TBI Initiative Steering Committee for this review (and for others in the series) to enable applicability and standardization across the six review articles prepared by AUS-TBI. Although all studies were RCTs, detailed methodological assessments of study quality were not included in this review due to the time frames required to be met for the consensus meetings and project completion. Additionally, as the purpose of this review was not to identify a “correct” modifying relationship but to describe the existing literature in sufficient detail in preparation for people to make an informed decision about modifiers in the consensus meeting, a full risk of bias assessment was not indicated.
Results
Results of the systematic review
The searches identified 14,455 records, including 5730 duplicates. The title and abstract of 8725 records were screened and 8601 were excluded. At the title and abstract screening phase, the research team changed the review methodology to only include RCTs. The full-length texts of 124 records were successfully obtained and reviewed, of which 88 records were excluded, yielding 35 RCTs included in this review (Fig. 1). Industry-sponsored drug trials were also excluded, as none reported benefit and none of the studied drugs are in current clinical practice. 14
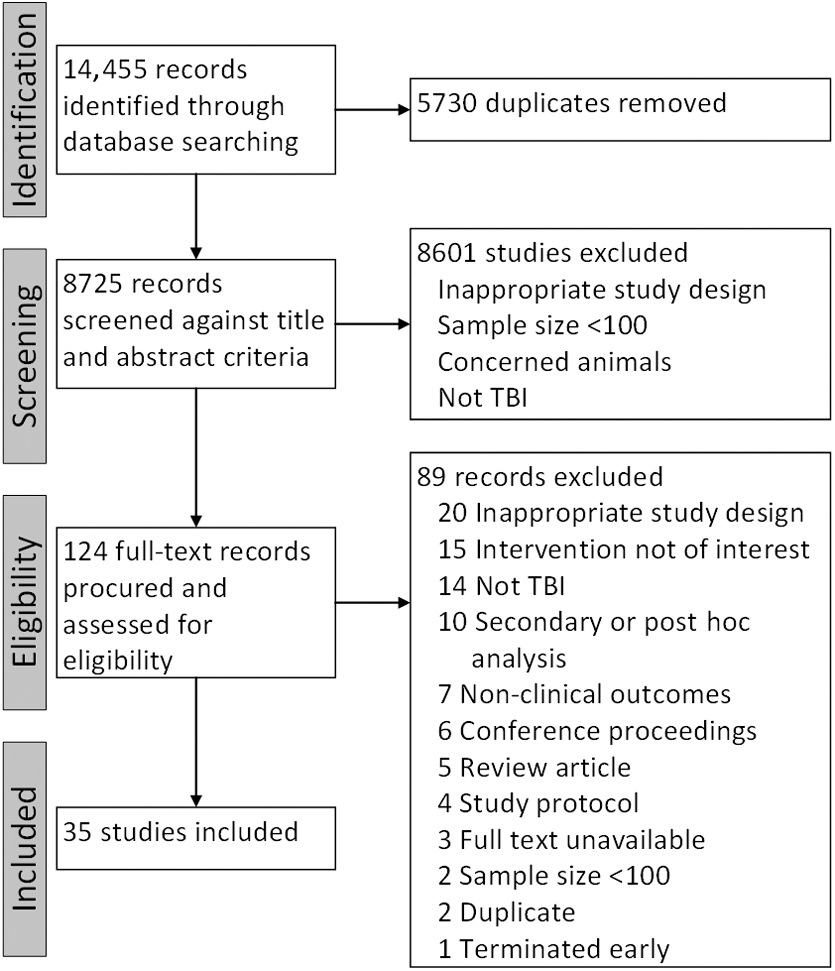
PRISMA diagram of included studies. TBI, traumatic brain injury.
This review included 35 unique studies, published across the period 1990 to 2020. The 34 raw modifier interventions were homogenized into 16 “modifiers” (e.g., “erythropoietin,” “Erythropoietin,” and “Erythropoiten” were homogenized as “erythropoietin”; Fig. 2) and 24 raw “comparator” interventions homogenized into 15 comparators (for example, “Standard care alone” and “Standard care” were homogenized to “standard care”). These two groups were further consolidated, leaving 26 unique modifier interventions, inclusive of both groups classified as “control” or “placebo.” Of 85 raw outcomes, there were 21 unique outcomes identified (Fig. 3). In summary, 148 observations on associations between these 26 modifier interventions and 21 outcomes were identified. To assess the extent to which each intervention modified an outcome, high, medium, low, or null values were assigned, based upon the rules outlined (see Sidebar 1). Interventions were considered worthy of inclusion in the group of common data elements if they were of at least of medium modifier value, in at least one study. The full list of included studies and the associations evaluated are described in Table 1.
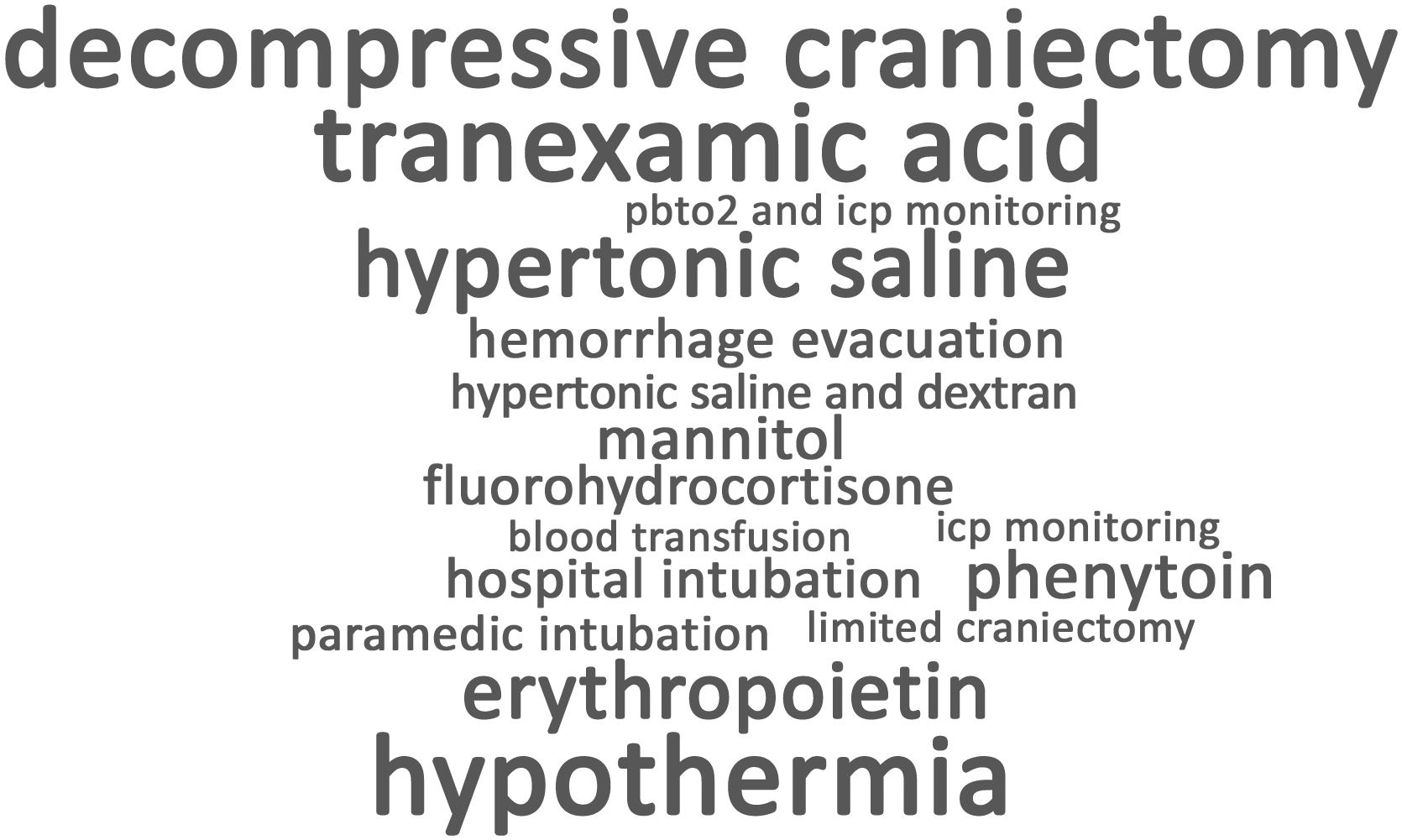
Word cloud for modifier interventions. This figure is a graphical representation of the number of studies testing each intervention identified in the review. Larger words reflect modifiers that appeared more frequently in the dataset.

Word cloud for outcomes. This figure gives greater prominence (larger words) to outcomes that were more frequently used in the included trials. gose, Glasgow Outcome Score-Extended; cva, cerebral vascular accident; gcs, Glasgow Coma Scale; katzindex, Katz Index of Independence in Activities of Daily Living
Summary of Included Studies and Associations Evaluated Between Acute Interventions and Outcomes for People With Moderate-Severe TBI
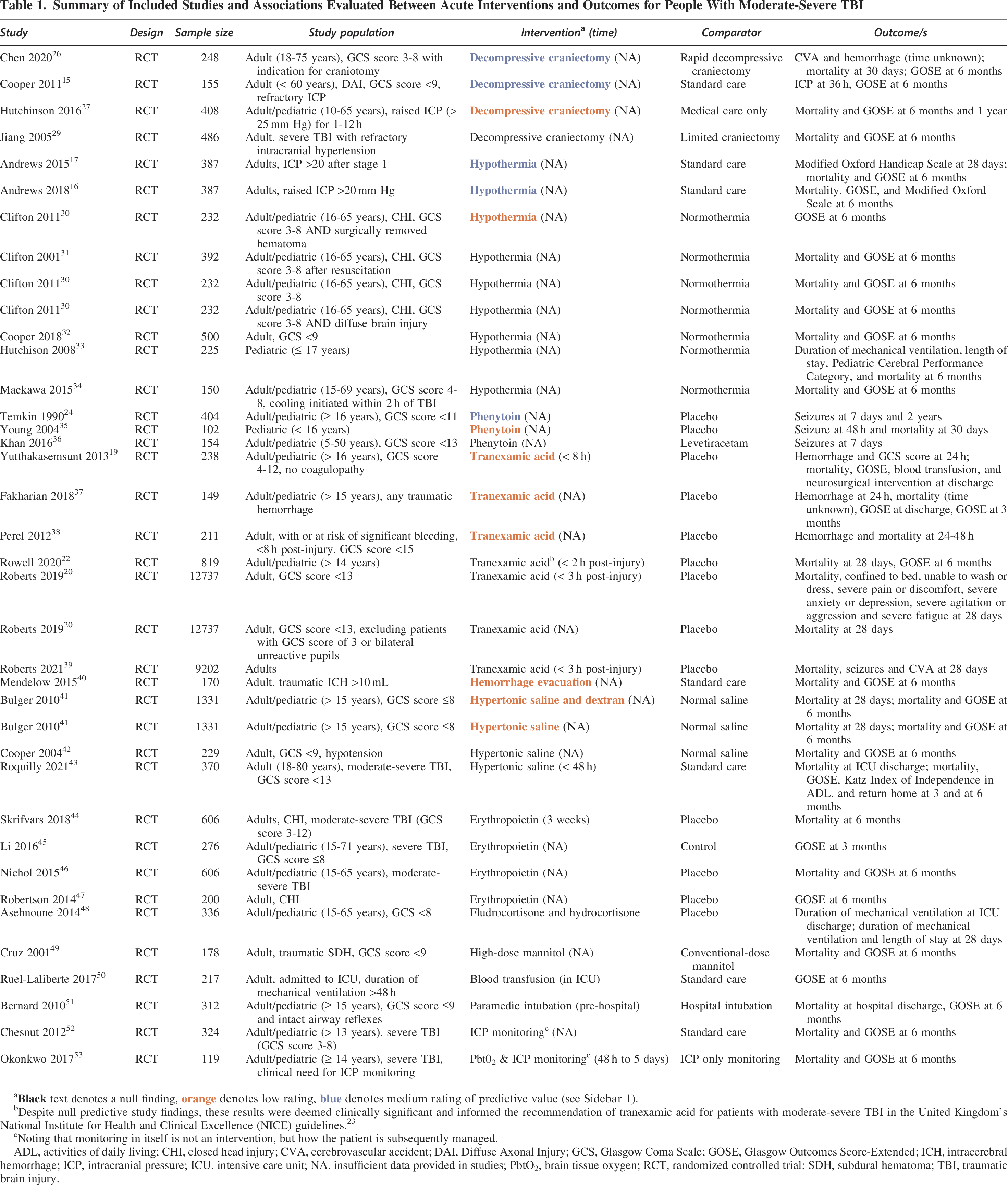
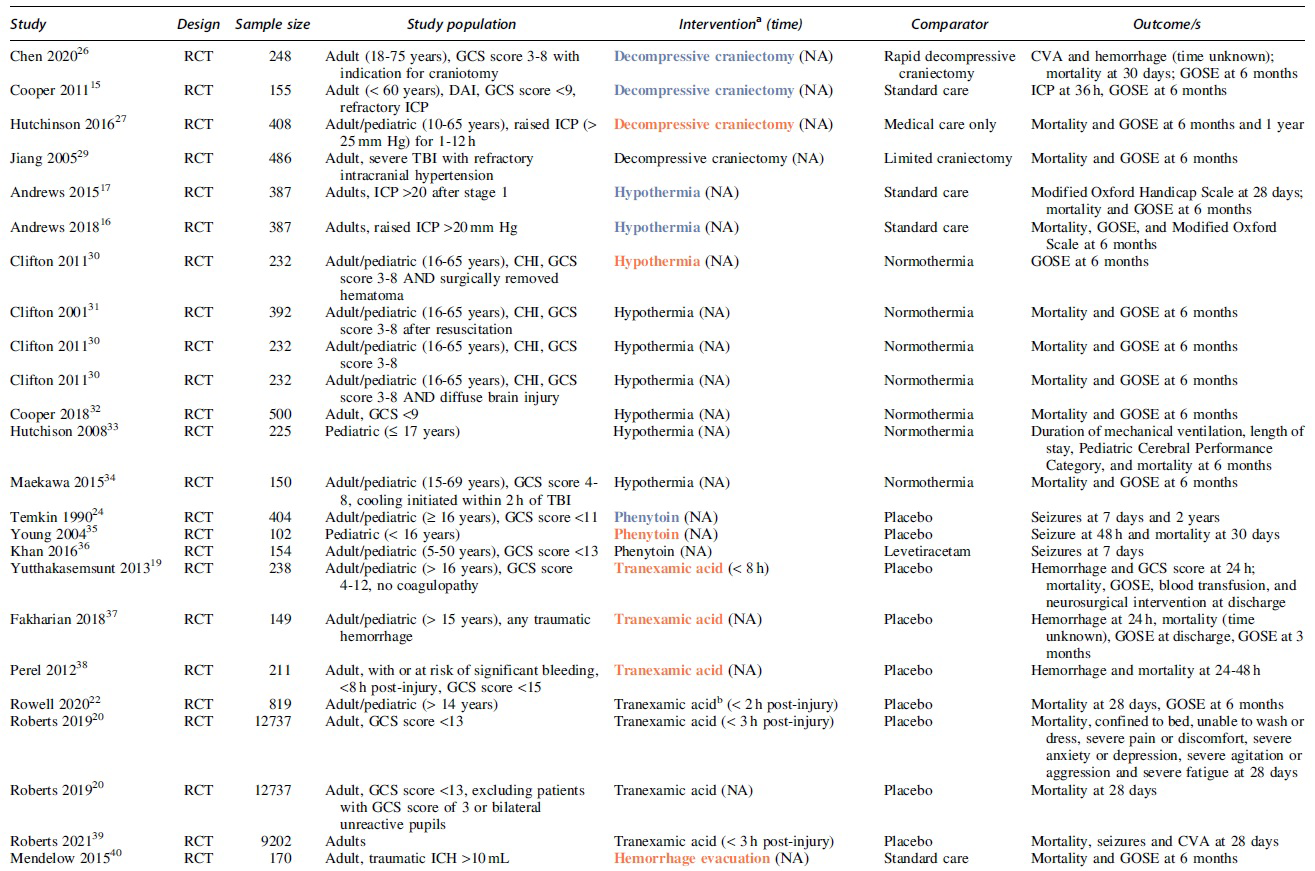
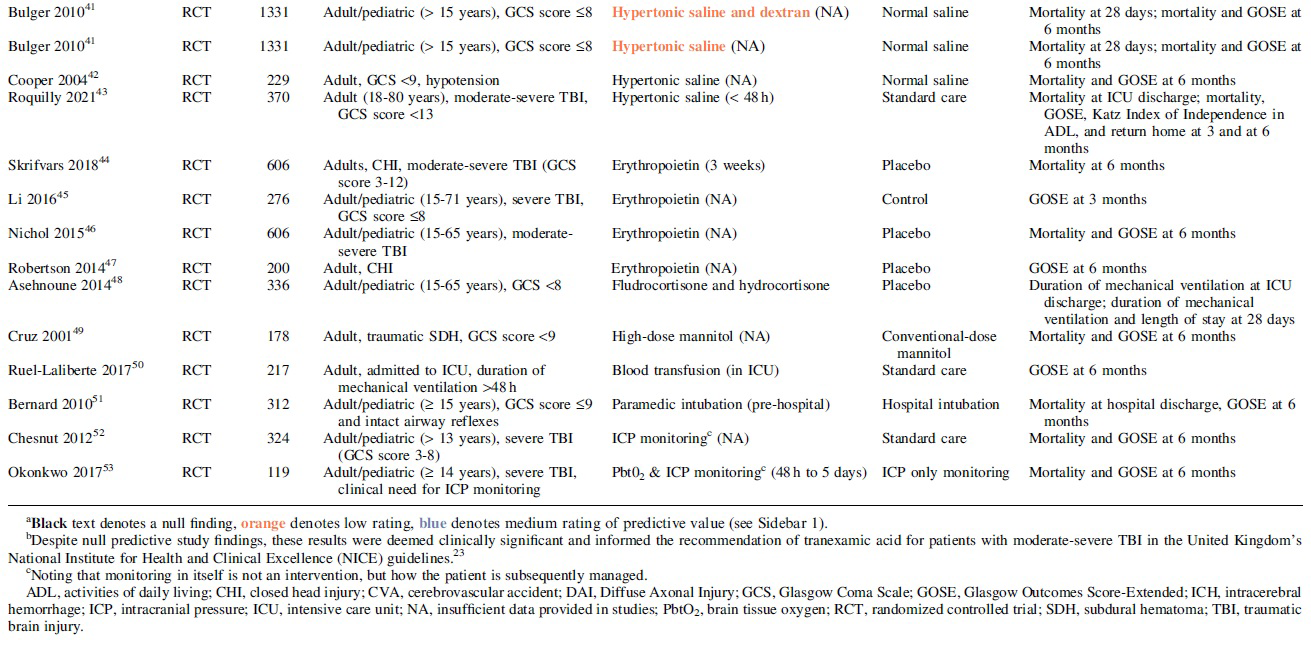
Decompressive craniectomy 15 and hypothermia16,17 were judged to be of medium modifier value, with the intervention groups in both cases being associated with poorer functional outcome (Glasgow Outcome Scale-Extended [GOS-E]) at 6 months following injury. Earlier decompressive craniectomy in patients with diffuse TBI unexpectedly decreased favorable (independent) outcomes at 6 months and in patients with extra-axial mass lesions it was found recently to be of no benefit. 18 Controversially, delayed decompressive craniectomy in patients with diffuse and mass-lesion TBI, saved lives while increasing severe disability at 6 months, and both severe and moderate disability at 12 months. The patients with decompressive craniectomy also tended to improve more over 48 months than those receiving usual medical care.
Tranexamic acid (TXA) was judged to be of medium modifier value for neurosurgical interventions, with people managed with TXA less likely to require neurosurgical intervention. 19 The CRASH-3 trial in patients predominantly from low-income countries found that TXA decreased mortality in patients with mild-to-moderate TBI, but not in those with severe TBI.20,21 Then in a subgroup of patients with msTBI without hypotension receiving bolus TXA dosing only, a Phase 2 trial found possible benefit. 22 There were also increased seizures, but nevertheless this trial informed the U.K. Clinical Guidelines recommendation to consider TXA administration for patients with a GCS score <13 without evidence of extracranial bleeding, as it was believed by the panel that despite the uncertain clinical trial evidence, there may be benefit in reducing all-cause mortality and mortality from TBI (full rationale can be found in the guidelines). 23 It was then recommended in these guidelines that TXA be given within 2 h of injury and before imaging with a 2-g IV bolus injection for people age 16 years and older, or by weight in those under age 16.
The fourth intervention of medium modifier value reported in this review was phenytoin, which was associated with fewer early post-traumatic seizures. 24 All other interventions reported in the included studies, listed in the word cloud (Fig. 2), were of null or low predictive value, or there were insufficient data available to make a judgement (Table 1).
Results of the consensus meeting
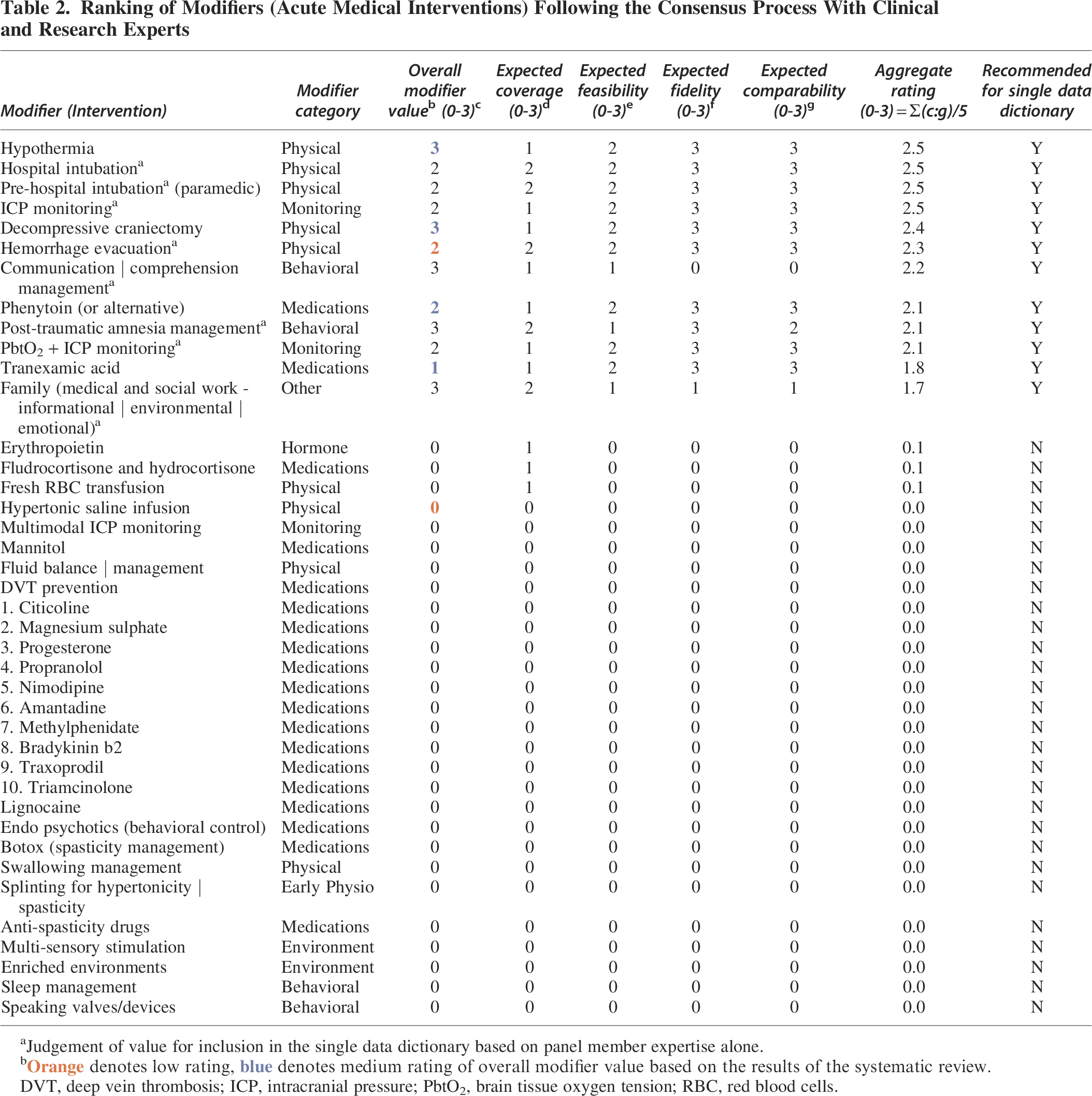
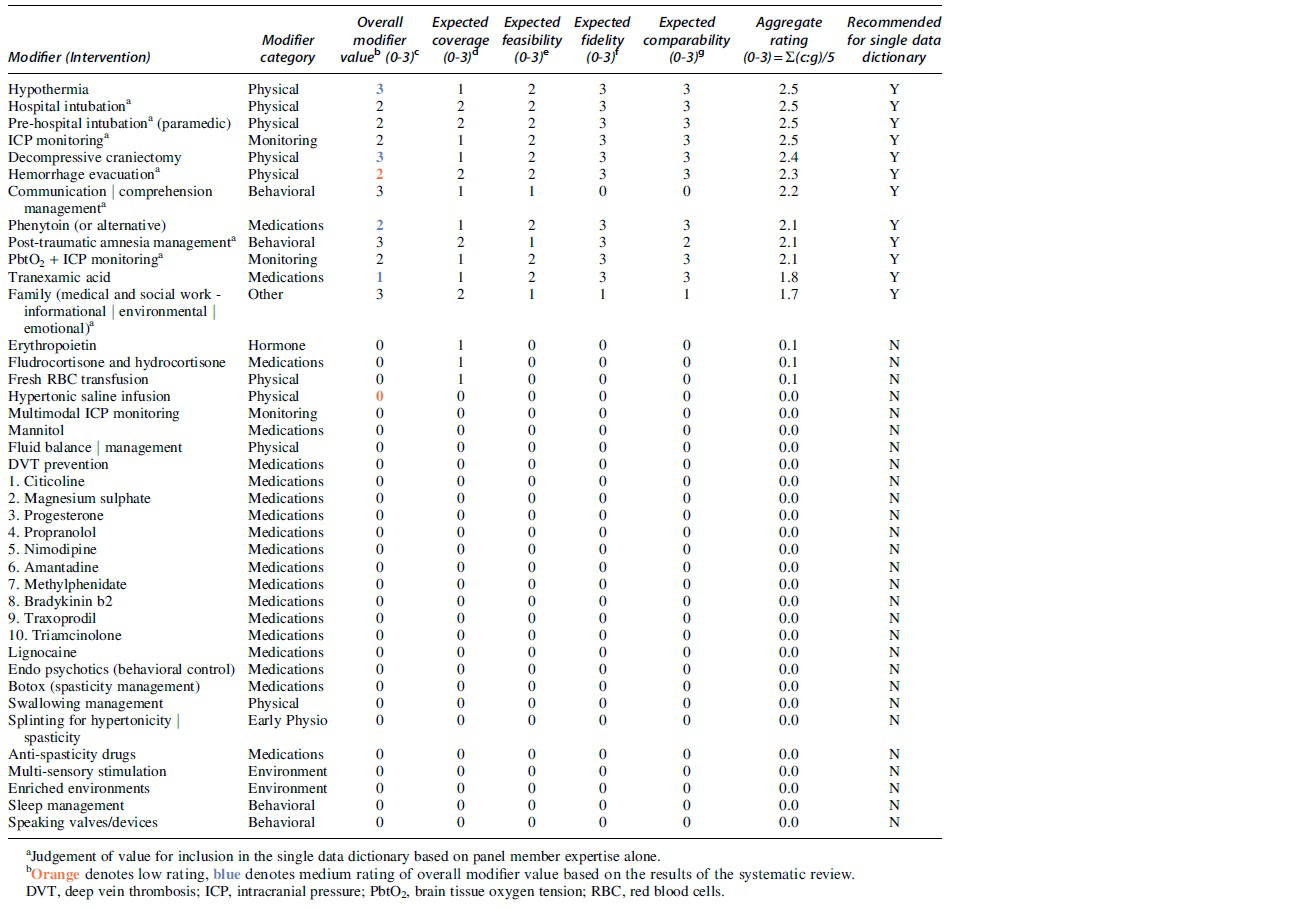
A list of potential interventions identified by the systematic review, including the ratings assigned to each modifier, was provided to the consensus group for consideration. The consensus meeting was convened in June 2022. Evidence from the systematic review, and the expected coverage, feasibility, and fidelity of data collection in the Australian context, were considered at the meeting. The aggregate rating scores for each modifier, as agreed by the panel, are shown in Table 2. The four interventions that were rated to be of medium modifier value from the systematic review also received a medium aggregate score in the consensus group meeting. An additional eight interventions were considered by the consensus group as potential modifiers worthy of inclusion in the single data dictionary (hospital intubation, pre-hospital (paramedic) intubation, ICP monitoring, brain tissue oxygen tension (PbtO2) + ICP monitoring, hemorrhagic evacuation, post-traumatic amnesia management, communication management, and information provided to family members). Contributions from Aboriginal and Torres Strait Islander people and people with lived experience of TBI were sought. 9
Ranking of Modifiers (Acute Medical Interventions) Following the Consensus Process With Clinical and Research Experts
Discussion
Thirty-five high-quality RCTs of acute medical interventions were identified by this review, but only four of these interventions were assessed to be of medium modifier value for any outcome in patients with msTBI, whereas no included trials of interventions were judged to be of high modifier value. Most of these trials found null or low modifier value associations between interventions and outcome. The interventions that could be considered for inclusion in a future national data resource were TXA and phenytoin, which had a positive effect on an outcome; and decompressive craniectomy surgery and hypothermia, which negatively affected outcomes. The utility of these interventions for inclusion in future predictive models for outcomes in patients with TBI could then be determined.
Increased ICP can result in impaired cerebral blood flow and cause secondary ischemic injuries. 25 Decompressive craniectomy is a neurosurgical intervention that involves the temporary removal of a portion of the skull, to relieve ICP and prevent secondary neurological damage following TBI. The use of decompressive craniectomy to reduce ICP following TBI is controversial and has been widely debated. 6 Some trials suggest that decompressive craniectomy may reduce mortality rates for some patients with severe TBI and late-stage refractory intracranial hypertension26,27 with the reduction in mortality sustained at 24 months. 28 In two key RCTs, which tested decompressive craniectomy and outcomes (DECRA 15 and RESCUEicp 27 ), patients with severe TBI who received earlier or later (respectively) decompressive craniectomy had shorter lengths of intensive care unit (ICU) stay, indicating faster reversal of ICU sedation and ICU discharge. However, they also had more vegetative and severe disability outcomes at 6 months. Although not statistically significant, the data trended toward similar findings at 12 months 54 and 24 months. 28 One trial defined “favorable” outcome as including severe disability, and reported an increase in this at 12 months after injury. 27 Notably, in the RESCUEicp trial, functional outcome (GOS-E) for the majority of patients in both the decompressive craniectomy and medical groups remained unchanged over the 6- to 24-month follow-up period. 28
Guidelines for the management of severe TBI have also highlighted that the type of decompressive craniectomy performed may be important in predicting outcomes, and this presents a critical knowledge gap in the management of severe TBI. 6 In clinical practice, choosing to perform a decompressive craniectomy is an urgent and complex decision where risks and benefits must be evaluated on a case-by-case basis to determine whether the life potentially saved by surgical ICP control is likely to have a quality acceptable to the patient, and to outweigh potential adverse impacts of two surgeries—the initial decompressive craniectomy and the required future cranioplasty. These results highlight the importance of future studies examining the effects of all potential interventions on the range of long-term health outcomes.
Hypothermia evaluations provided good-quality evidence that hypothermia is a modifier with negative outcome following msTBI.16,31,32 Hypothermia works to lower an individual's body temperature to reduce cerebral metabolism, decrease ICP, and perhaps, improve outcomes. Although a recent systematic review of therapeutic hypothermia for TBI management found that it was associated with a reduction in mortality and improved functional outcomes, most included trials were of low quality, with small study numbers and poor explanation of allocation concealment and randomization methods. 55 In comparison, the studies of therapeutic hypothermia with medium modifier value included in this review favored standard medical care, with hypothermia leading to unchanged or poorer functional outcomes (GOS-E).15,16 The use of hypothermia carries risk, with patients also having bradycardia, increased pneumonia, 55 and fluid overload leading to paradoxically increased ICP after hypothermia withdrawal. Further randomized trials of hypothermia in msTBI are very unlikely to be supported.
TXA is a pharmacological agent that reduces bleeding by inhibiting the enzymatic breakdown of fibrin blood clots (fibrinolysis). Intracranial bleeding is common following TBI and can result in increased ICP and worse outcomes following TBI. 56 When administered early following injury, TXA decreases bleeding-related deaths in patients with TBI with major extracranial bleeding.21,38 Further work by Gayet-Ageron and colleagues found that early TXA for people with acute, severe hemorrhage had a survival benefit that was reduced by 10% for every 15 min of treatment delay until 3 h, after which there was no benefit. 57 Specific to TBI, the CRASH-3 trial, a large RCT, found that very early TXA (within 3 h) reduced the risk of head-injury-related death within 28 days. 20 This benefit was in patients with mild-to-moderate TBI, but not in those with severe TBI. 20 CRASH-3 did not measure long-term outcomes, and it also included many patients from low- to middle-income countries where pre-hospital care is usually limited, so the findings may have less relevance for patients from high-income countries. 20
Perhaps surprisingly, the negative three-arm Phase 2 trial of TXA in msTBI, which found increased seizures, 22 did not slow clinical recommendations in the United Kingdom. 23 Most recently, and perhaps of greatest relevance to patients in high-income countries, the 2023 Australia and New Zealand PATCH trial randomized 1310 trauma patients at high risk of acute coagulopathy, and then measured functional outcomes at 6 months. 58 TXA decreased mortality at 28 days but not 6 months, whereas at the same time TXA increased severe disability outcomes, with findings that were concordant in patients with msTBI. 58 Thus, the ongoing TXA controversy now pivots on the desirability of severe disability as an outcome after TBI. Our future national data resource for msTBI will therefore include longer-term functional outcomes at 6, 12, and 24 months.
Phenytoin is an anticonvulsant, commonly used in acute TBI management for prophylaxis of post-traumatic seizures.6,59 After a brain injury, seizures can exacerbate neurological damage and increase the risk of mortality. 60 Seizure activity following msTBI may be experienced by up to 21% of patients in the first week after an msTBI. 61 Phenytoin is effective in preventing seizures; however, it has limited modifier value for patients' clinical outcomes.35,61,62 A major concern with phenytoin as a therapy is the list of side-effects and drug interactions associated with its use, 63 but most of these are not relevant for short-term post-injury usage. The 1990 trial by Temkin and colleagues formed the basis of clinical recommendations regarding the use of phenytoin, or similar anticonvulsants, in the management of severe TBI to minimize the risk of post-traumatic seizures. 24 Despite the beneficial effects of anticonvulsant drugs for early post-traumatic seizures, early prophylactic seizure treatments do not appear to decrease the risk of post-traumatic epilepsy or mortality. Short-term prophylaxis as is universally used post severe TBI is generally considered safe, 6 but longer-term use may adversely affect functional outcomes.61,62,64,65
Strengths and limitations
To our knowledge, this is the first systematic review assessing the effect, for better or worse, of acute medical and surgical interventions on clinical outcomes in people with msTBI. Strengths of this review include the thorough search strategy that included eight comprehensive literature databases from their inception, screening articles with at least two independent reviewers to ensure consistency, and a rigorous data extraction process with assignment of modifier judgements. The large collaborative effort between clinical experts (including but not limited to intensivists, emergency physicians, and pharmacists), scientific experts, and people with lived experience of brain injury in the design, implementation, and findings of this review and consultation through the consensus process is an additional strength.
There are several limitations of this study. Given the heterogeneity of available publications across a wide range of intervention and control variables, different outcome measures and various time-points of follow-up, a meta-analysis could not be completed. Similarly, it was not possible to compare modifying associations between different interventions and outcomes, beyond a simple judgement algorithm (high, medium, low, null) as described (see Sidebar 1). In some studies, certain individual interventions were used as modifiers for several different outcomes in a single study, rather than across several studies. Our results describing the frequency with which an intervention (modifier or comparator) was reported are biased because some trials reported more than one intervention. This was necessary to ensure that all potential modifying associations were included and judged on an individual level. No methodological assessment of each included RCT (beyond randomization and sample size greater than 100 patients) was able to be undertaken. Finally, the consensus meeting for this article consisted predominantly of rehabilitation specialists, with fewer acute care physicians. Because rehabilitation-phase interventions were out of scope for the systematic review, these were added by the consensus meeting.
Conclusions
High-quality trials of medical and surgical interventions for the acute management of msTBI report varying degrees of clinical effectiveness and varying potential value as outcome modifiers. Four medical and surgical interventions were judged to be the strongest modifiers of a clinical outcome following msTBI: TXA and phenytoin, which had a positive effect on an outcome; and decompressive craniectomy surgery and hypothermia, which negatively affected outcomes. From the results of the expert consultation process and systematic review, 12 acute medical interventions were identified for inclusion as outcome modifiers in a single data dictionary of msTBI for a future national data resource. The AUS-TBI data resource will support development of improved algorithms for outcome prediction after msTBI, with the aim of assisting clinical decision-making at key time-points in the acute care of individual patients with TBI. Further research using contemporary, large data sets is required to determine whether including data on use of these interventions can increase the accuracy of predictive algorithms for outcome in patients with msTBI.
Transparency, Rigor, and Reproducibility Summary
This study was conducted following a planned protocol. Deviations from the protocol have been clearly reported herein. The meta data and search strategies and the data set are available in Supplementary Appendixes S1 and S2, respectively. Annotated R scripts are available on request, subject to written agreement. Further information is available at the discretion of the corresponding author.
AUS-TBI Initiative Investigators
Tara Alexander, Australasian Rehabilitation Outcomes Centre & Australian Health Services Research Institute, Faculty of Business and Law, University of Wollongong, Wollongong, New South Wales, Australia; Vicki Anderson, Psychology Service, The Royal Children's Hospital, Melbourne, Victoria, Australia; Clinical Sciences Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Ana Antonic-Baker, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Elizabeth Armstrong, School of Medical and Health Sciences, Edith Cowan University, Perth, Western Australia, Australia; Franz E. Babl, Department of Emergency Medicine, The Royal Children's Hospital, Melbourne, Victoria, Australia; Departments of Paediatrics and Critical Care, University of Melbourne, Melbourne, Victoria, Australia; Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Matthew K. Bagg, Curtin Health Innovation Research Institute, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; School of Health Sciences, University of Notre Dame Australia, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Perth, Western Australia, Australia; Centre for Pain IMPACT, Neuroscience Research Australia, Sydney, New South Wales, Australia; Zsolt J. Balogh, Department of Traumatology, John Hunter Hospital and University of Newcastle, Newcastle, New South Wales Australia; Karen M Barlow, Acquired Brain Injury in Children Research Program, Queensland Children's Hospital, Brisbane, Queensland, Australia; Centre for Children's Health Research, University of Queensland, Brisbane, Queensland, Australia; Judith Bellapart, Department of Intensive Care Services, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Faculty of Medicine, University of Queensland, Brisbane, Queensland, Australia; Niranjan Bidargaddi, Flinders Digital Health Centre, College of Medicine & Public Health, Flinders University, Adelaide, South Australia, Australia; Erika Bosio, Centre for Clinical Research in Emergency Medicine, Harry Perkins Institute of Medical Research, Perth, Western Australia, Australia; School of Biomedical Science & School of Medicine, University of Western Australia, Perth, Western Australia, Australia; Peter Bragge, BehaviourWorks Australia, Monash Sustainable Development Institute, Monash University, Melbourne, Victoria, Australia; Michael Bynevelt, School of Surgery, The University of Western Australia, Perth, Western Australia, Australia; Neurological Intervention and Imaging Service of Western Australia, Sir Charles Gairdner Hospital, Perth, Western Australia, Australia; Karen Caeyenberghs, Cognitive Neuroscience Unit, School of Psychology, Deakin University, Geelong, Victoria, Australia; Peter A. Cameron, National Trauma Research Institute, Melbourne, Victoria, Australia; School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Emergency and Trauma Centre, The Alfred Hospital, Melbourne, Victoria, Australia; Jacquelin Capell, Australasian Rehabilitation Outcomes Centre & Australian Health Services Research Institute, Faculty of Business and Law, University of Wollongong, Wollongong, New South Wales, Australia; Kevin E.K. Chai, School of Population Health, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Curtin Institute for Computation, Curtin University, Perth, Western Australia, Australia; Lyndsey E. Collins-Praino, School of Biomedicine, University of Adelaide, Adelaide, South Australia, Australia; D.J. Jamie Cooper, Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Department of Intensive Care and Hyperbaric Medicine, The Alfred, Melbourne, Victoria, Australia; Gill Cowen, School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Louise M. Crowe, Clinical Sciences Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Victoria, Australia; Tim Cudmore, AUS-TBI Lived Experience Advisory Group; Jennifer Cullen, Synapse, Brisbane, Queensland, Australia; James Cook University, Townsville, Queensland, Australia; Menzies Health Institute Queensland, Griffith University, Brisbane, Queensland, Australia; Kate Curtis, Susan Wakil School of Nursing and Midwifery, Faculty of Medicine and Health, The University of Sydney, New South Wales, Australia; Illawarra Shoalhaven Local Health District, Wollongong, New South Wales, Australia; Illawarra Health and Medical Research Institute, Wollongong, New South Wales, Australia; George Institute for Global Health, Sydney, New South Wales, Australia; Anthony Delaney, Division of Critical Care, The George Institute for Global Health, Sydney, New South Wales, Australia; Malcolm Fisher Department of Intensive Care Medicine, Royal North Shore Hospital, Sydney, New South Wales, Australia; Northern Clinical School, Sydney Medical School, University of Sydney, Sydney, New South Wales, Australia; Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria Australia; Graeme Dibdin, AUS-TBI Lived Experience Advisory Group; Sandra Eades, Centre for Epidemiology and Biostatistics, Melbourne School of Population and Global Health, University of Melbourne, Melbourne, Victoria, Australia; School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Gary F. Egan, Monash Biomedical Imaging & School of Psychological Sciences, Monash University, Melbourne, Victoria, Australia; Daniel Y. Ellis, Department of Trauma, Royal Adelaide Hospital, Adelaide, South Australia, Australia; Statewide South Australian Trauma Service, South Australia, Australia; School of Public Health and Tropical Medicine, James Cook University, Queensland, Australia; Ari Ercole, Division of Anaesthesia, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Cambridge Centre for AI in Medicine, University of Cambridge, United Kingdom; Daniel M. Fatovich, Emergency Medicine, Royal Perth Hospital, University of Western Australia, Perth, Western Australia, Australia; Centre for Clinical Research in Emergency Medicine, Harry Perkins Institute of Medical Research, Perth, Western Australia, Australia; Murray J. Fisher, Susan Wakil School of Nursing and Midwifery, Faculty of Medicine and Health, University of Sydney, New South Wales, Australia; Royal Rehab, Ryde, Sydney, New South Wales, Australia; Mark Fitzgerald, National Trauma Research Institute, Melbourne, Victoria, Australia; Melinda Fitzgerald, Curtin Health Innovation Research Institute, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Perth, Western Australia, Australia; Jennifer Fleming, School of Health and Rehabilitation Sciences, The University of Queensland, Brisbane, Queensland, Australia; Roslyn Francis, Department of Health, Government of Western Australia, Perth, Western Australia, Australia; Belinda J. Gabbe, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Health Data Research UK, Swansea University Medical School, Swansea University, Singleton Park, United Kingdom; Adelle Gadowski, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; John Gilroy, Aboriginal and Torres Strait Islander Research, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Mitchell A. Hansen, Department of Neurosurgery, John Hunter Hospitals and University of Newcastle, Newcastle, New South Wales, Australia; James E. Harrison, College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia; Luke J. Haseler, Curtin Health Innovation Research Institute, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Leanne Hassett, Institute for Musculoskeletal Health & Sydney School of Health Sciences, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Sydney Local Health District, Sydney, New South Wales, Australia; Sarah C. Hellewell, Curtin Health Innovation Research Institute & School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Nedlands, Western Australia, Australia; Amelia J. Hicks, School of Psychological Sciences, Monash University, Melbourne, Victoria, Australia; Monash Epworth Rehabilitation Research Centre, Epworth Healthcare, Melbourne, Victoria, Australia; Brain Injury Research Center, Icahn School of Medicine at Mount Sinai, New York City, New York, United States of America; Andrew F. Hill, College of Science, Health and Engineering, La Trobe University, Melbourne, Victoria, Australia; Andrew J.A. Holland, The Children's Hospital at Westmead Clinical School, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Stephen Honeybul, Department of Neurosurgery, Sir Charles Gairdner Hospital, Perth, Western Australia, Australia; Department of Neurosurgery, Royal Perth Hospital, Perth, Western Australia, Australia; Rosalind L. Jeffree, Kenneth G. Jamieson Department of Neurosurgery, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Royal Brisbane Clinical School, School of Medicine, University of Queensland, Brisbane, Queensland, Australia; Chris Joyce, Intensive Care Unit, Princess Alexandra Hospital, Brisbane, Queensland, Australia; School of Medicine, University of Queensland, Brisbane, Queensland, Australia; Elizabeth Kendall, Menzies Health Institute Queensland, Griffith University, Brisbane, Queensland, Australia; Kate King, John Hunter Trauma Service, John Hunter Hospital, Newcastle, New South Wales, Australia; College of Health, Medicine and Wellbeing, University of Newcastle, Newcastle, New South Wales, Australia; Natasha A. Lannin, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Alfred Health, Melbourne, Victoria, Australia; Meng Law, Departments of Neuroscience and Radiology, Monash University, Melbourne, Victoria, Australia; Alfred Health, Melbourne, Victoria, Australia; Alzheimer's Disease Research Center & Department of Neurological Surgery, Keck School of Medicine, University of Southern California, Los Angeles, California, United States of America; Andrew I.R. Maas, Department of Neurosurgery, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Adam Mahoney, Trauma Service, Royal Hobart Hospital, Hobart, Tasmania, Australia; 2nd General Health Battalion, Australian Defence Force; Peter Makin, AUS-TBI Lived Experience Advisory Group; Peter Mayhew, AUS-TBI Lived Experience Advisory Group); Alison McDonald (AUS-TBI Lived Experience Advisory Group; Skye McDonald, School of Psychology, University of New South Wales, Sydney, New South Wales, Australia; Stuart J. McDonald, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Ancelin McKimmie, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Robert McNamara, Department of Intensive Care Medicine, Royal Perth Hospital, Perth, Western Australia, Australia; School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Shiv Meka, Department of Health, Government of Western Australia, Perth, Western Australia, Australia; David K. Menon, Division of Anaesthesia, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Wolfson Brain Imaging Centre, University of Cambridge, Cambridge, United Kingdom; Gary Mitchell, Emergency and Trauma Unit, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Royal Brisbane Clinical Unit, University of Queensland, Brisbane, Queensland, Australia; Jamieson Trauma Institute, Brisbane, Queensland, Australia; Queensland Rugby Union; Brisbane, Queensland, Australia; Rowena Mobbs, Brain & Mind Centre, University of Sydney, Sydney, New South Wales, Australia; Macquarie University, Sydney, New South Wales, Australia; Fatima A. Nasrallah, Queensland Brain Institute, University of Queensland, Brisbane, Queensland, Australia; Virginia F.J. Newcombe, PACE Section, Department of Medicine, Addenbrooke's Hospital, University of Cambridge, Cambridge, United Kingdom; Terence J. O'Brien, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; John H. Olver, Epworth Healthcare, Melbourne, Victoria, Australia; Department of Medicine, Monash University, Melbourne, Victoria, Australia; Gerard M. O'Reilly, National Trauma Research Institute, Melbourne, Victoria, Australia; Emergency and Trauma Centre, The Alfred Hospital, Melbourne, Victoria, Australia; School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Tamara Ownsworth, The Hopkins Centre, Menzies Health Institute Queensland, Griffith University, Brisbane, Queensland, Australia; School of Applied Psychology, Griffith University, Brisbane, Queensland, Australia; Paul M. Parizel, University of Antwerp, Edegem, Belgium; Department of Radiology, Royal Perth Hospital & University of Western Australia, Perth, Western Australia, Australia; West Australian National Imaging Facility Node, Perth, Western Australia, Australia; Michael Parr, Intensive Care Unit, Liverpool Hospital, University of New South Wales, Sydney, New South Wales, Australia; Intensive Care Unit, Macquarie University Hospital, Macquarie University, Sydney, New South Wales, Australia; Jennie L. Ponsford, School of Psychological Sciences, Monash University, Melbourne, Victoria, Australia; Monash Epworth Rehabilitation Research Centre, Epworth Healthcare, Melbourne, Victoria, Australia; Bruce Powell, AUS-TBI Lived Experience Advisory Group; Patricia Ratajczak, AUS-TBI Lived Experience Advisory Group; Michael C. Reade, Faculty of Medicine, University of Queensland, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Joint Health Command, Australian Defence Force, Canberra, Australian Capital Territory, Australia; Sandy Reeder, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Christopher Reid, School of Public Health, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Julia Robertson, AUS-TBI Lived Experience Advisory Group; Suzanne Robinson, School of Population Health, Faculty of Health Sciences, Curtin University, Perth Western Australia, Australia; Stephen E. Rose, The Australian e-Health Research Centre, Commonwealth Scientific and Industrial Research Organisation, Brisbane, Queensland, Australia; Jeffrey V. Rosenfeld, Department of Neurosurgery, The Alfred Hospital, Melbourne, Victoria, Australia; Department of Surgery, Monash University, Melbourne, Victoria, Australia; F. Edward Hébert School of Medicine, Uniformed Services University of The Health Sciences, Bethesda, Maryland, United States of America; Jason P. Ross, Molecular Diagnostic Solutions, Health and Biosecurity, Commonwealth Scientific and Industrial Research Organisation, Australia; Danette Rowse, AUS-TBI Lived Experience Advisory Group; Nick Rushworth, Brain Injury Australia, Sydney, New South Wales, Australia; Adam Scheinberg, Neurodevelopment and Rehabilitation Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Victoria, Australia; Bridgette D. Semple, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Alfred Health, Melbourne, Victoria, Australia; Department of Medicine, Royal Melbourne Hospital, The University of Melbourne, Melbourne, Victoria, Australia; Sandy R. Shultz, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Grahame K. Simpson, Brain Injury Rehabilitation Research Group, Ingham Institute for Applied Medical Research, Sydney, New South Wales, Australia; John Walsh Centre for Rehabilitation Research, Sydney School of Medicine, University of Sydney, Sydney, New South Wales, Australia; Warwick J. Teague, Trauma Service & Department of Paediatric Surgery, The Royal Children's Hospital, Melbourne, Victoria, Australia; Surgical Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Victoria, Australia; Leanne Togher, Speech Pathology, School of Health Sciences, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Andrew A. Udy, Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Department of Intensive Care and Hyperbaric Medicine, The Alfred Hospital, Melbourne, Victoria, Australia; Kirsten Vallmuur, Centre for Healthcare Transformation, Australian Centre for Health Services Innovation, Queensland University of Technology, Brisbane, Queensland, Australia; Jamieson Trauma Institute, Brisbane, Queensland, Australia; Dinesh Varma, Department of Radiology, The Alfred Hospital, Melbourne, Victoria, Australia; Department of Surgery, Monash University, Melbourne, Victoria, Australia; National Trauma Research Institute, Melbourne, Victoria, Australia; James Vickers, Wicking Dementia Research and Education Centre, College of Health and Medicine, University of Tasmania, Hobart, Tasmania, Australia; Janet Wagland, Brightwater Group, Perth, Western Australia, Australia; James Walsham, Intensive Care Unit, Princess Alexandra Hospital, Brisbane, Queensland, Australia; School of Medicine, University of Queensland, Brisbane, Queensland, Australia; Adam J. Wells, Department of Neurosurgery, Adelaide Hospital, Adelaide, South Australia, Australia; Department of Surgery, University of Adelaide, Adelaide, South Australia, Australia; Neurosurgical Research Foundation, Adelaide, South Australia, Australia; Luke Whiley, Health Futures Institute, Murdoch University, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Perth, Western Australia, Australia; Gavin Williams, Department of Physiotherapy, Epworth Healthcare, Melbourne, Victoria, Australia; Department of Physiotherapy, University of Melbourne, Melbourne, Victoria, Australia; Jodie K. Williams, National Critical Care and Trauma Response Centre, Royal Darwin Hospital, Darwin, Northern Territory, Australia; Roslind Witham, AUS-TBI Lived Experience Advisory Group; David K. Wright, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Louise York, Australian Institute of Health and Welfare, Canberra, Australian Capital Territory, Australia; Jesse T. Young, Centre for Health Equity, Melbourne School of Population and Global Health, The University of Melbourne, Melbourne, Victoria, Australia; Centre for Adolescent Health, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; School of Population and Global Health, University of Western Australia, Perth, Western Australia, Australia; National Drug Research Institute, Curtin University, Perth, Western Australia, Australia; Heidi Zeeman, The Hopkins Centre, Menzies Health Institute Queensland, Griffith University, Brisbane, Queensland, Australia.
Footnotes
Author Disclosure Statement
MKB has received personal fees for travel or consulting from Chiropractor's Association of Australia, Memorial University of Newfoundland, Life Ready Health Group and Active Linc Pty. Ltd. MKB has received research funding from the Australian National Health and Medical Research Council, Medical Research Future Fund, and Research Training Program, Australia (RTP) schemes, University of New South Wales, and Neuroscience Research Australia (NeuRA). DJC occasionally consults to Pressura Neuro P/L, all funds to Monash University. MF is the CEO of the charitable organization Connectivity-Traumatic Brain Injury Australia.
Funding Information
This work was funded by the Australian Government's Medical Research Future Fund, ID2008223. The funder had no role in study design, data collection and analysis, data interpretation, and manuscript writing, or the decision to submit the article for publication.
Authors' Contributions
Jemma Keeves: project administration, data curation, visualization, writing—original draft; Adelle Gadowski: methodology, project administration, resources, data curation, writing—review and editing; Ancelin McKimmie: methodology, project administration, resources, data curation, visualization, writing—review and editing; Matthew K. Bagg: methodology, project administration, resources, data curation, visualization, formal analysis; Cristina Roman: methodology, data curation; Ana Antonic-Baker: methodology, project administration, resources, data curation, visualization, writing—review and editing; Amelia J. Hicks: methodology, project administration, resources, data curation, visualization, writing—review and editing; Lorena Romero: methodology, data curation; Nyssa Clarke: data curation, writing—review and editing; Alastair Brown: data curation, writing—review and editing; Rob McNamara: data curation, writing—review and editing; Sandy Reeder: data curation, writing—review and editing; Toby Jeffcote: data curation, writing—review and editing; Jennie L. Ponsford: conceptualization, funding acquisition, methodology, writing—review and editing; Natasha A. Lannin: conceptualization, funding acquisition, methodology, writing—review and editing; Terence J. O'Brien: conceptualization, funding acquisition, methodology, writing—review and editing; Peter A. Cameron: conceptualization, funding acquisition, methodology, writing—review and editing; Nick Rushworth: conceptualization, funding acquisition, methodology, writing—review and editing; Melinda Fitzgerald: conceptualization, funding acquisition, methodology, project administration, writing—review and editing; Belinda J. Gabbe: conceptualization, funding acquisition, methodology, writing—review and editing; D. Jamie Cooper: conceptualization, funding acquisition, methodology, supervision, data curation, writing—original draft; AUS-mTBI Investigators: conceptualization, writing—review and editing.