
Abstract
Abstract
Recent advances in multi-omics approaches encompassing genomics, transcriptomics, proteomics, and metabolomics offer hitherto unprecedented insights on common complex human diseases. A unique angle pertinent for both diagnostic and therapeutic sciences involves rethinking clinically distinct diseases with a view to their shared molecular targets, interactomes, and pathophysiologies. Reflecting at a scale of disease-to-disease associations might help clinicians, public health practitioners, drug and biotechnology developers, and associated knowledge industries in the current era. This review article examines the hypothesis that “Intersecting Molecular Pathways Permit Interventions on Multiple Clinical Endpoints”, thus uniquely bringing together Crohn's disease and periodontitis. Furthermore, we propose a novel connector molecular target between these two ostensibly distinct diseases at a clinical level, human beta defensin (hBD)-2, and suggest pathways by which hBD-2 can conceivably connect Crohn's disease and periodontitis by virtue of regulating the innate-immune response. We conclude by emphasizing different approaches where hBD-2 can be employed as a diagnostic and therapeutic tool to improve the quality of life of susceptible individuals and minimize the economic costs of these two major global public health problems. The strategy presented here also presents potentials for targeting of multiple diseases through a unique “nodal molecular target” that “speaks to” multiple clinical endpoints.
Introduction
I
Reflecting at a scale of disease-to-disease associations might help clinicians, public health practitioners, drug and biotechnology developers, and associated knowledge industries in the current era. This review article examines the integrative biology concept presented below, thus uniquely bringing together Crohn's disease and periodontitis.
Concept
“Intersecting Molecular Pathways Permit Interventions on Multiple Clinical Endpoints”
The current moves to conceptualize common complex diseases as syndromes with a shared clinical typology, comprised of multiple molecular pathways, have important corollaries. This means that at certain molecular intersection points it might be possible to intervene on more than one disease or several subtypes of an apparently homogenous disease-syndrome. Defining common risk groups for wide-spread diseases, exploring their underlying shared risk factors, and constructing cost-effective preventive measures for those public health problems will minimize the psychological and economic impacts of these diseases on individuals, and eventually, on public.
This mini-review applies the above hypothesis to the case of Crohn's disease and periodontitis through human beta defensin (hBD)-2. Ulcerative colitis (UC), which is another form of inflammatory bowel disease, will not be included into this review because genetic expression profiles, including that of hBD-2, are different in Crohn's disease and UC (Fellermann et al., 2006).
Connecting the Dots with Beta Defensin-2
Crohn's disease and UC are two forms of inflammatory bowel disease (IBD). Both diseases are characterized by a chronic dysregulation of mucosal immune response of the gastrointestinal tract and share similarities in their pathophysiology. While Crohn's disease can affect any part of the gastrointestinal tract, UC is restricted to colon and rectum (Ananthakrishnan, 2015). In Europe, the incidence of Crohn's disease is between 0.3–12.7 per 100,000 persons (Ananthakrishnan, 2015), and it creates an economic burden of 2.1–16.7 billion euros (Floyd et al., 2015). Traditionally, the incidence of IBD has been highest in developed continents, such as in North America and Europe. Nevertheless, with the constant westernization of the life styles of emerging populations, for example, in Asian nations, the incidence of IBD is increasing throughout the world.
Periodontitis, on the other hand, is an infection-induced inflammatory disease of the tooth-supporting tissues. It usually demonstrates a chronic, asymptomatic, and episodic character. It differs from gingivitis, the inflammation of gingiva, in that periodontitis is accompanied with degradation of hard tissues, the alveolar bone. At individual level, it causes tooth loss and, consequently, defects in speech and nutrition, and thereby reduces the quality of life. At the public level, it is an escalating burden to the healthcare economy (Chapple, 2014). Among the global adult population, the prevalence of advanced periodontitis ranges from 5%–15% (Dye, 2012).
Several lines of evidence and rationales connect Crohn's disease and periodontitis. If we can connect these two distinct diseases through a common genetic background, this may mean that individuals who develop Crohn's disease can be in risk of developing periodontitis as well. With that knowledge, it can be possible to develop health policies to invest in preventive treatment of risk groups, rather than treating disease in larger populations. Therefore, below, we will define the prevalence of periodontal diseases in individuals with periodontal disease, describe the similarities in the pathogenesis of Crohn's disease and periodontitis, connect these two distinct diseases with hBD-2, and finally suggest applicable approaches to support healthcare economy.
Periodontal Diseases in Individuals with Crohn's Disease
While the prevalence of oral findings in subjects with Crohn's disease is relatively high, reports on a putative association specifically between periodontal diseases and Crohn's disease are limited (Katsanos et al., 2015). One plausible reason for the lack of reports in this literature domain is that the association studies were performed hitherto on subjects with both Crohn's disease and UC, under a common diagnosis of IBDs. The first report on the oral findings of a subject with Crohn's disease dates back to 1969 (Dudeney, 1969). Most common oral symptoms of Crohn's disease include apthous-ulcerative lesions, nonspecific swellings, and cobblestone architecture of the oral mucosa (Scheper and Brand, 2002; Harty et al., 2005). Moreover, the caries prevalence was found to be higher in subjects with Crohn's disease than in healthy controls (Brito et al., 2008).
The clinical findings of Crohn's disease were not limited to mucosal changes and caries, but it was also observed that Crohn's disease can accompany with symptoms of periodontal diseases (Brito et al., 2008; Flemmig et al., 1991; Grössner et al., 2006; Stein et al., 2010; Vavricka et al., 2013). A case of a young male with Crohn's disease suffering from rapidly progressive periodontitis was the first to mention a relation between these two different disease entities (Lamster et al., 1978).
Later, a greater gingival inflammation, but less periodontal tissue destruction, was demonstrated on 10 subjects with IBD (6 subjects with Crohn's disease and 4 with UC), in comparison to a group of age- and sex-matched systemically healthy periodontitis patients (Van Dyke et al., 1986). Interestingly, in the same study, the authors presented a defect in neutrophil chemotaxis and an increased prevalence of motile gram-negative species of the genus Wolinella (currently Camphylobacter) in periodontal pockets (Van Dyke et al., 1986).
In a larger study population with 107 IBD patients (46 Crohn's disease and 61 UC patients), it was demonstrated that periodontal disease in IBD subjects was more generalized but less severe when compared to a general population in the USA (Flemmig et al., 1991). In a successive case-control study in 121 subjects, including 62 IBD patients, a slightly higher prevalence of clinical attachment loss was observed in the IBD group, in comparison to systemically healthy controls (Grössner et al., 2006). While the probing pocket depth scores in Crohn's disease patients showed similarities as reported before (Flemmig et al., 1991), clinical signs of inflammation in the IBD group were not significantly different from the controls (Grössner et al., 2006).
A study by Brito et al. (2008) compared the periodontal health status of 179 IBD patients (99 Crohn's disease and 80 UC patients) to 74 systemically healthy subjects. After adjustment for race, gender, smoking habit, age, and dental plaque, Crohn's disease patients were found to have significantly deeper probing pocket depths than controls. Furthermore, among nonsmokers, Crohn's disease patients showed significantly fewer sites with plaque but deeper pocket depths compared to controls. The prevalence of periodontitis was significantly higher in the patient groups than in their controls (Brito et al., 2008).
It is noteworthy that in certain studies (Flemmig et al., 1991; Grössner et al., 2006) probing pocket depth and clinical attachment level scores were measured either in two sites (Flemmig et al., 1991) or four sites (Grössner et al., 2006) of only two quadrants. It is well proven that partial-mouth designs underestimate the severity of periodontitis (Thomson and Williams, 2002). When measuring the periodontal parameters from six sites of all teeth, Stein et al. (2010) demonstrated greater probing pocket depths and a higher prevalence of periodontitis in Crohn's disease patients, than in previous studies mentioned above. The severity of periodontitis, however, was shown to be similar in all studies (Brito et al., 2008; Flemmig et al., 1991; Grössner et al., 2006; Stein et al., 2010).
Habashneh et al. (2012) investigated the association between the prevalence, severity, and extent of periodontitis among patients with UC (n=101) or Crohn's disease (n=59) and their systemically healthy controls (n=100). All periodontal parameters (plaque index, gingival index, probing pocket depth, clinical attachment level, and gingival recession) were elevated in subjects with Crohn's disease. Moreover, the prevalence of periodontitis was higher in the age group of 18–45 year controls. The high prevalence of periodontitis in young adults is surprising, since initiation and progression of periodontitis is highly related with age and the prevalence of periodontitis is relatively low in young adults (<35 years-of-age) (Kassebaum et al., 2014).
In a prospective study by Vavricka et al. (2010), including 113 patients with IBD (69 Crohn's disease and 44 UC) and 113 healthy volunteers, higher gingivitis and periodontitis parameters were found in patients with IBD compared to the healthy control group. In the Crohn's disease group, gingival inflammation was significantly more pronounced than in the control group. In a recent study, where the occurrence and progression of periodontal disease was examined in SAMP mice that develop spontaneously Crohn's disease-like ileitis, it was demonstrated that the severity of periodontitis strongly correlates to the severity of ileitis (Pietropaoli et al., 2014).
In summary, there is substantial evidence that subjects with Crohn's disease, often at relatively young age, are prone to develop periodontitis, especially its severe forms.
Similarities in Pathogenesis of Crohn's Disease and Periodontitis
Both Crohn's disease and periodontitis are common multifactorial and complex diseases, which seem to share similarities in their etiology and pathogenesis. Aberrations in the sensitively controlled cytokine network against pathosymbionts are supposed to be one important aspect in the pathology of periodontitis and Crohn's disease, potentially linking these diseases (Bouma and Stober, 2003; Kornman, 2008; Schulz et al., 2014). Environmental (e.g., smoking) and genetic (e.g., NOD2/CARD15) factors are also known as regulators of their etiologies (Indriolo et al., 2011). Three defects in the innate-immune response are the most recognized connectors of Crohn's disease and periodontitis, and these will be discussed in detail below (Fig. 1).
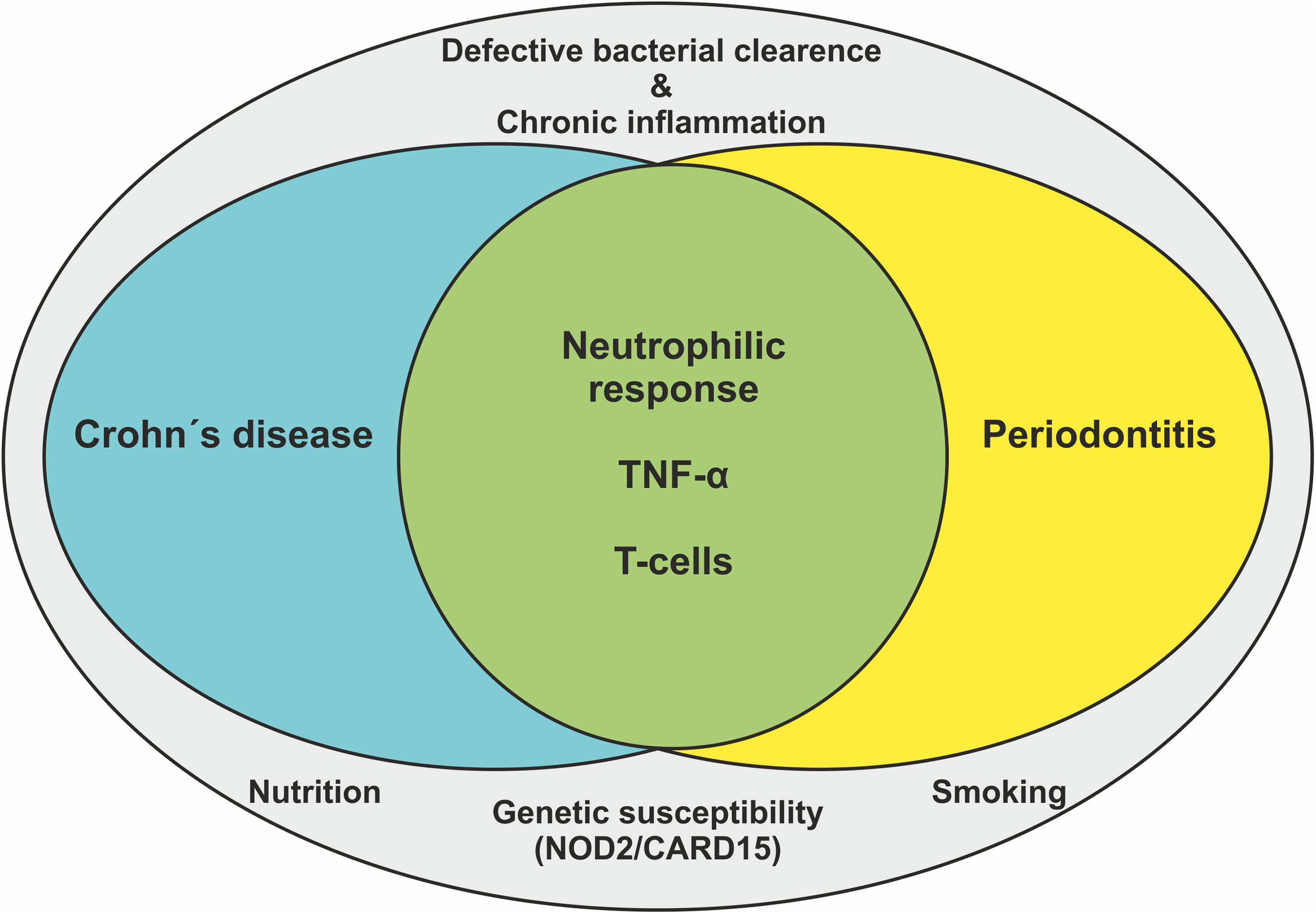
Crohn's disease and periodontitis are proposed to share common environmental, systemic, and genetic factors, and disturbances in innate immune response parameters (neutrophilic chemotaxis, tumor necrosis factor (TNF)-α expression, and T-cell functions).
First, a defect in neutrophil chemotaxis was connected to the pathogenesis of Crohn's disease and periodontitis, which was a case report of a 28-year-old white male with Crohn's disease (Lamster et al., 1978). This patient suffered from painful bleeding gums, and radiographic evaluation demonstrated rapidly progressive alveolar bone loss. Serum analyzes of the patient revealed altered neutrophil functions, which is considered significant in certain forms of periodontal disease (Roberts et al., 2015), as well as in Crohn's disease (Koldkjaer et al., 1977). Later on, the same group of researchers confirmed their initial findings by demonstrating that neutrophils of IBD patients have 45% less activity than those of systematically healthy controls (Lamster et al., 1982). Moreover, a serum-mediated defect in the neutrophil chemotaxis was also presented (Van Dyke et al., 1986).
Second, the impairment in tumor necrosis factor (TNF)-α secretion is another factor that may link periodontitis and Crohn's disease. TNF-α is a potent proinflammatory cytokine, which is released mainly by T-cells at sites of inflammation (Garlet, 2010). Elevated levels of TNF-α have been observed in serum of patients with Crohn's disease (Szczeklik et al., 2012). In a recent study by Schulz et al. (2014), investigating the impact of TNF-α polymorphisms on periodontal markers in 142 patients with Crohn's disease, oral soft tissue lesions were significantly more common in A allele carriers of rs361525 than G carriers. They suggested that the TNF-α A allele of rs361525 representing a significant risk factor for oral inflammatory alterations (Schulz et al., 2014). These data from above-mentioned studies present a TNF-α mediated connection between Crohn's disease and periodontitis.
A third connection between Crohn's disease and periodontitis was built via T-cell functions. A case of a 60-year-old woman with diagnoses of Crohn's disease and severe generalized periodontitis with several periodontal abscesses was the first to give a role on T-cell functions to connect these two distinct diseases (Engel et al., 1988). Numerous medical reports had reported lymphocyte and leukotriene B4 (LTB4) abnormalities in Crohn's disease patients, therefore, lymphocyte subset profiles, B cell function, and LTB4 synthetic activity of PMNs were analyzed in the patient, and the data were compared to these available from two systemically and periodontally healthy control subjects. The B cell profile of the patient exhibited a paucity of brightly stained cells, and the T cell profile contained a large distinct subpopulation of dull-staining cells. While B cell growth factor proved to be normal in the patient, its responsiveness to anti-IGM was approximately one-half of that of the controls. Instead, a normal range of lymphocyte concentrations was observed in the patient. It was also stated that total counts of B and T cells per μL of blood did not significantly differ between the patient and the controls (Engel et al., 1988).
Atypical T helper 1 (Th1) response, with an overproduction of interferon (IFN)-γ, is characteristic for Crohn's disease. IFN-γ can activate macrophages to release inflammatory cytokines, including TNF-α, interleukin (IL)-1β, and IL-6, which, at the end, leads to a chronic inflammatory condition (Monteleone et al., 2002). In periodontitis, increased levels of IFN-γ, IL-2, IL-10, IL-17A, and TNF-α had been observed in several studies, demonstrating the participation of Th1/Th2/Th17 cell cytokines in the disease pathogenesis (Gaffen and Hajishengallis 2008; Souto et al., 2014). Therefore, the intensive hyperactive T-cell theory is perhaps seen as one most widely accepted connection between Crohn's disease and periodontitis (Indriolo et al., 2011).
Human Beta-Defensin-2: A Pivotal Intersection in the Molecular Nexus
During the last decade, variations in genome copy numbers of hBD-2 were associated with periodontitis (Jaradat et al., 2013) and Crohn's disease (Bentley et al., 2010; Fellermann et al., 2006). The hBDs are a group of cationic antimicrobial peptides, which are secreted by epithelial cells. In the oral cavity and gastrointestinal tract, they form a major part of the innate immune response against continuous bacterial insult. Their main role is to act as antimicrobial peptides by causing pores on the bacterial membrane and stimulating bacterial lysis. Furthermore, they act as regulators of the immune response, for example, by being chemotactic to T cells. In in vitro experiments, hBD-2 has shown to enhance the secretion and the mRNA expression of IFN-γ, TNF-α, IL-1β, -6, -10, and -22 of CD3/28-stimulated T cells (Kanda et al., 2011).
Moreover, hBD-2 contributes to the recruitment and migration of Th17 cells in inflamed endothelium (Ghannam et al., 2011). It is possible to hypothesize that an impaired hBD-2 response is a functional interactome in the pathogeneses of Crohn's disease and periodontitis, since hBD2 takes part in both T-cell functions and cytokine networks, which are known to connect these two distinct diseases. A bioinformatics analysis to demonstrate the association between hBDs and the T cell signaling pathway and cytokine networking is given in Figure 2 and Table 1.

Protein–protein interaction network between beta-defensins and T cell receptor signaling pathway-related proteins (KEEG Pathway Database; http://www.genome.jp/kegg/pathway.html; map04660), developed by using the STRING 9.1 database resource search tool (http://string-db.org/) under a confidence score of 0.400. Proteins belonging to the interaction network between hBDs and T-cell receptor signaling pathway-related proteins are given in Table 1.
While there is considerable information on the regulation of immune responses by hBD-2, the evidence on the associations between Crohn's disease and periodontitis and hBD-2 genomic (DEFB4) copy number variations is still sparse. A study on the associations of the occurrence and severity of chronic periodontitis and DEFB4 among study population of 227 subjects with Caucasian decent demonstrated that subjects carrying low DEFB4 copy numbers in serum have a 3-fold higher risk for developing severe periodontitis, in comparison to controls (Jaradat et al., 2013). However, in oral samples (saliva, gingival crevicular fluid, or gingival tissue) from subjects with periodontitis, both elevated and decreased levels of hBD-2 have been reported. Possible explanations on these controversies, such as degradation of hBDs by bacteria- or host-derived enzymes, were discussed in our recent review (Gursoy and Könönen, 2012).
The first study to seek an association between DEFB4 copy numbers and Crohn's disease of the colon demonstrated that individuals with the hBD-2 gene copy number of <4 were predisposed to colonic Crohn's disease via diminished mucosal hBD-2 mRNA expression (Fellermann et al., 2006). Their findings were challenged by Bentley et al. (2010), who showed that elevated gene copy numbers of DEFB4 increase the risk for developing Crohn's disease. Interestingly, at protein levels, hBD-2 was found to be the same in subjects with and without Crohn's disease; however, lipopolysaccharide-induced hBD-2 production is significantly elevated in biopsies from subjects with Crohn's disease when compared to these from healthy controls (Aldhous et al., 2009). The latter findings are of interest; according to previous studies, impaired hBD expression due to a mutation of NOD2 gene leads to an impaired intestinal barrier function, and thus Crohn's disease is developed (Wehkamp et al., 2002; 2005).
Do Subjects with Crohn's Disease have Impaired hBD-2 Response against Bacteria? A Decision Aid to Define the Risk of Developing Periodontitis
In humans, antimicrobial peptide hBD-2 acts as an antibacterial agent and immune-regulator in both health and disease. On one hand, as an antibacterial agent, its deficiency may be related to the increased tendency to develop chronic infectious diseases, such as periodontitis or Crohn's disease. On the other hand, since it is chemotactic for T-cells, its overexpression may be related to aggravated immune response, which is again a common scenario in both periodontitis and Crohn's disease.
We therefore propose that subjects with Crohn's disease could be screened for their hBD-2 responsiveness to early define the subjects at risk for developing periodontitis. This would be an easy procedure; for example, collecting saliva samples with DNA self-collection kits (Nunes et al., 2012), and later analyzing the gene copy number variants of DEFB4. Then subjects with low or high gene copy numbers can be defined and directed to more intense check-ups by their dentist. Alternatively, epithelial cells could be collected by buccal swabs and stimulated with bacterial lipopolysaccharides to follow their hBD-2 responses (Mathews et al., 1999). Again, hypo- or hyper-responsive individuals could be detected and directed to their dentists.
It is plausible that Crohn's disease and periodontitis have different genetic and environmental backgrounds other than hBD-2-related impairments. However, these two noninvasive and cost-effective methods can be useful in preventing the development and progression of periodontitis in high-risk individuals with Crohn's disease, which can help policy-makers in the field of public health to construct cost-effective preventive measures against periodontitis.
Conclusions
The information given in this review is directed to a diverse group of scientists and top executives of drug development and biotechnology industries and regulators interested in emerging intersections of systems medicine, oral health, novel molecular targets, and diagnostics. Executive take-home points are listed in Table 2. We believe that the identification of shared hBD-2-related pathogenic pathways of Crohn's disease and periodontitis will enable us to integrate diagnostic approaches, identify novel therapeutic targets, and define risk groups of these distinct diseases. With the aid of these preventive, diagnostic, and therapeutic approaches, it will be possible to minimize the economic costs of these two major global public health problems.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicting financial interests.