
Abstract
Abstract
Antibiotics are often recommended as treatment for patients with chronic obstructive pulmonary disease (COPD) exacerbations. However, not all COPD exacerbations are caused by bacterial infections and there is consequently considerable misuse and overuse of antibiotics among patients with COPD. This poses a severe burden on healthcare resources such as increased risk of developing antibiotic resistance. The biomarker procalcitonin (PCT) displays specificity to distinguish bacterial inflammations from nonbacterial inflammations and may therefore help to rationalize antibiotic prescriptions. We report in this study, a three-country comparison of the health and economic consequences of a PCT biomarker-guided prescription and clinical decision-making strategy compared to current practice in hospitalized patients with COPD exacerbations. A decision tree was developed, comparing the expected costs and effects of the PCT algorithm to current practice in the Netherlands, Germany, and the United Kingdom. The time horizon of the model captured the length of hospital stay and a societal perspective was also adopted. The primary health outcome was the duration of antibiotic therapy. The incremental cost-effectiveness ratio was defined as the incremental costs per antibiotic day avoided. The incremental cost savings per day on antibiotic therapy avoided were (in Euros) €90 in the Netherlands, €125 in Germany, and €52 in the United Kingdom. Probabilistic sensitivity analyses showed that in the majority of simulations, the PCT biomarker strategy was superior to current practice (the Netherlands: 58%, Germany: 58%, and the United Kingdom: 57%). In conclusion, the PCT biomarker algorithm to optimize antibiotic prescriptions in COPD is likely to be cost-effective compared to current practice. Both the percentage of patients who start with antibiotic treatment as well as the duration of antibiotic therapy are reduced with the PCT decision algorithm, leading to a decrease in total costs per patient. Economic analysis based on real-life data is recommended for further research. Biomarker-driven prescription algorithms are important instruments for personalized medicine in COPD. This also attests to the emerging convergence of biomarker innovations and the broader field of Health Technology Assessment (HTA).
Introduction
C
Antibiotics are essential for treating infections, yet overuse and misuse contribute to the development of antibiotic resistance (European Centre for Disease Prevention and Control, 2017; Wenzel and Edmond, 2000) and pose an increasing burden on healthcare resources. This necessitates research on interventions that enhance the appropriate use of antibiotics. One option for doing so is measuring the biomarker procalcitonin (PCT). PCT has good specificity to distinguish bacterial from nonbacterial inflammations and could therefore help prevent unnecessary antibiotic prescriptions and/or reduce the duration of antibiotic therapy (Simon et al., 2004).
Several studies have been performed in hospitalized COPD patients with acute exacerbations, investigating the influence of a PCT strategy on the percentage of patients in whom antibiotic therapy is initiated and the duration of antibiotic use (Christ-Crain et al., 2004; Kristoffersen et al., 2009; Schuetz et al., 2009; Stolz et al., 2007). A systematic review showed that PCT-guided antibiotic therapy can significantly reduce the number of initial antibiotic prescriptions without increasing the incidence of adverse events (Tokman et al., 2011). PCT-guided antibiotic therapy may also lead to a shorter duration of antibiotic therapy (Tokman et al., 2011), but further research need to confirm these results.
Despite these favorable findings, the upfront costs of PCT testing remain a barrier for hospitals to adopt this test. A detailed analysis of the extent to which PCT testing impacts overall hospital costs is essential to gain insights to its value-based procurement. This model-based cost-effectiveness analysis therefore estimates, from a Dutch, German, and United Kingdom perspective, the expected health and economic outcomes of a PCT strategy on antibiotic prescription rate and duration of antibiotic therapy in patients hospitalized with COPD exacerbations.
Materials and Methods
A health economic model was constructed to compare the health economic consequences of a “PCT strategy” to guide the initiation and duration of antibiotic therapy versus current practice in hospitalized patients with COPD exacerbations (Fig. 1). The PCT algorithm provides guidance on initiation and/or duration of antibiotic therapy, based on the concentration of PCT in a patient's blood: at a PCT concentration below <0.1 μg/L, antibiotic therapy is strongly discouraged; at a PCT concentration between 0.1 and 0.25 μg/L, it is discouraged; at a PCT concentration between 0.25 and 0.5 μg/L, it is recommended; and antibiotic therapy is strongly recommended at a PCT value >0.5 μg/L.

Decision tree structure.
By means of simulation, the health outcomes and costs accrued in a hypothetical population of patients treated according to the PCT algorithm to guide antibiotic therapy is compared to a population of patients treated in accordance with currently used guidelines (Woodhead et al., 2011). These guidelines recommend antibiotics in patients with COPD exacerbations who have: (1) sputum purulence, increased dyspnea and/or sputum volume, and (2) a severe exacerbation that requires invasive or noninvasive mechanical ventilation. Antibiotics are not recommended in patients without sputum purulence and in patients with only one or less of the previously mentioned symptoms (Woodhead et al., 2011).
The model captured data on costs and effects for patient populations for the Netherlands, Germany, and the United Kingdom (Table 1). For each country, results were calculated from a societal perspective. The time horizon of the model covered the duration of a patient's hospital stay. The primary effectiveness measure was the average duration of antibiotic therapy per patient in the PCT strategy versus current practice. Costs included are total direct hospital costs and patients' productivity losses during hospital stay. Incremental costs of PCT and current practice strategy were divided by the incremental number of antibiotic days avoided per strategy, giving an incremental cost-effectiveness ratio (ICER) expressed as the incremental cost per antibiotic day avoided.
COPD, chronic obstructive pulmonary disease.
Literature review
A systematic literature review was performed to determine to what extent a PCT algorithm affects antibiotic prescription rates, duration of antibiotic therapy, intensive care unit (ICU) length of stay, total duration of hospital stay, number of days on mechanical ventilation, and number of blood cultures and other laboratory analyses performed.
PubMed was searched from the year 2000 onward for relevant articles that reported outcomes on at least one of those parameters. The following combinations of terms were searched in all fields: (strategy OR guide OR guided OR based) AND (COPD OR COPD exacerbations OR AECOPD OR Lower Respiratory Tract Infections OR LRTI) AND (PCT or procalcitonin) AND (antibiotic OR antibiotics). The search was limited to articles published in English, Dutch, or German, and restricted to randomized controlled trials (RCTs), meta-analyses, and systematic reviews. Only articles that reported on (1) an adult patient population, (2) hospitalized COPD or LRTI patients, and (3) the effect of a PCT algorithm on antibiotic prescription rate and/or the duration of antibiotic therapy, were included.
Relevant articles were initially selected based on title and abstract. After that, full texts were reviewed to assess whether articles met the inclusion criteria. The literature search was performed in January 2015.
Mean values and standard deviations (SDs) were obtained from each of the individual studies where possible. In case no mean and SD were reported, estimates of mean and SD were calculated according to Hozo et al. (2005). Subsequently, weighted mean differences were calculated using Review Manager version 5.1, combining the studies' sample sizes with the mean and SD of each parameter, using a random-effects model (Higgins et al., 2011).
Resource use
Country-specific data were used to determine the average number of hospitalization days of a patient and the percentage of patients who are prescribed antibiotics in current practice. Parameter input values for the PCT strategy were calculated by adjusting current practice values with the percentage change that was found in the systematic literature review.
Length of ICU stay, percentage of patients with COPD exacerbations admitted to the ICU, and number of days on antibiotic therapy were based on the systematic literature review. The percentage of patients receiving mechanical ventilation was obtained from Lindenauer et al. (2015) and considered equal in both strategies. The percentage of patients in whom a blood culture is taken was based on the prospective, cluster-randomized, controlled single-blinded analysis that compared the effect of using a PCT strategy to current practice (Christ-Crain et al., 2004). There are two blood cultures taken per patient, which is considered adequate to gain valid results (Weinstein et al., 1983). The number of PCT tests done per patient with COPD exacerbation was based on Cleves et al. (2010).
As no country-specific data were available for these parameters, their input values were considered equal across countries and sensitivity analyses were performed to determine the potential impact of this assumption on the model outcomes for each country. Table 2 shows all resource use inputs for the model.
ICU, intensive care unit; PCT, Procalcitonin.
Unit costs
The model considers costs of hospital stay, diagnostic tests (including, among others, PCT and blood cultures), treatments (including antibiotic therapy and mechanical ventilation), and productivity losses (Table 3) (Department of Health, 2012; Dorschner, 2006; Hakkaart-van Roijen et al., 2011; Martin et al., 2008; Muller et al., 2010; Nederlandse Zorgautoriteit, 2014; van Nieuwkoop et al., 2010). Costs per hospital day, mechanical ventilation costs, and productivity losses were all country specific. Costs of PCT tests and antibiotic therapy were assumed equal across countries. There is currently no fixed price for the PCT assay; therefore, these costs were based on interviews with clinical chemists and intensivists. Costs per day of antibiotic therapy were based on an economic evaluation of PCT-guided antibiotic therapy in acute respiratory infections (ARIs) in the US ($9.10 for the initial day of antibiotic therapy and $14.67 per day follow-up antibiotics) (Schuetz et al., 2015). A conversion rate of $1.00 is €0.72 was used (Wisselkoers, 2016).
Overview of cost parameters used in the model. For each cost parameter, its value in the Netherlands, Germany, and in the United Kingdom is indicated, with its associated reference. Expert opinions were obtained through interviews with intensivists (n = 2) and clinical chemists (n = 5).
All costs were converted to 2014 Euros. The time horizon of the model encompasses the duration of the patient's hospital stay. As this is shorter than one year, discounting future effects and costs was not necessary.
Assumptions
Mechanical ventilation takes place in the ICU only. The duration of mechanical ventilation is therefore set to be equal to the number of days a COPD patient with an exacerbation is admitted to the ICU. Furthermore, it is assumed that laboratory tests are ordered once daily during a patient's hospital stay.
Sensitivity analyses
Probabilistic sensitivity analysis was performed to assess the joint decision uncertainty stemming from uncertainty in parameter input values. Parameter distributions were defined using the method-of-moments approach, based on the parameter mean and standard error. Beta distributions were assigned to the probability parameters and Gamma distributions to the resource use parameters (Briggs and Claxton, 2006). Ten thousand random draws from all parameter distributions, simultaneously, give a scatterplot of cost-effectiveness estimates spread around the mean. Cost-effectiveness acceptability curves (CEACs) show the proportion of simulated outcomes that fall below a given willingness-to-pay threshold for one antibiotic day avoided.
One-way sensitivity analyses were performed to identify the parameters that, when changed, affected the outcome of the model the most. The base case value of each input parameter was varied over a range of alternative values starting 1 SD below to 1 SD above the mean. Parameters for which no measure of variance was reported in the literature were varied ±25% of their mean value.
Role of the funding source
The study sponsor had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Results
Literature search
The search strategy initially resulted in 18 unique articles. Five articles were subsequently excluded because these did not focus on adult hospitalized COPD patients and two articles were excluded because their main focus was on developing a clinical algorithm to determine antibiotic use (Albrich et al., 2011; Baer et al., 2013; Berg and Lindhardt, 2012; Briel et al., 2005, 2008; Schuetz et al., 2011; Tang et al., 2013). The 11 remaining articles included 5 RCTs, 4 systematic reviews (all meta-analyses), 1 model-based economic evaluation, and 1 addendum to an RCT. Reviewing the reference lists of these articles led to the inclusion of 1 additional systematic review, resulting in a final set of 12 studies (Tokman et al., 2011).
All included RCTs applied a similar PCT strategy, where prescription of antibiotic therapy is strongly discouraged at a PCT value <0.1 μg/L; discouraged at a PCT value of 0.1–0.25 μg/L; recommended at a PCT value of 0.25–0.5 μg/L; and strongly recommended at a PCT value >0.5 μg/L.
Effectiveness
A statistically significant reduction in the primary effectiveness parameter of 1.58 antibiotic days (95% confidence interval [CI] −2.29 to −0.88) was found for the PCT strategy versus current practice (Christ-Crain et al., 2004; Kristoffersen et al., 2009; Schuetz et al., 2012). In addition, a relative reduction of 33% in the antibiotic prescription rate in the PCT group was found (Christ-Crain et al., 2004; Kristoffersen et al., 2009; Schuetz et al., 2009; Stolz et al., 2007). In current practice, country-specific estimates of the percentage of COPD patients hospitalized with an exacerbation that are prescribed antibiotics are 39% in Germany, 53% in the Netherlands, and 81% in the United Kingdom (Bont et al., 2009; Buckingham et al., 2008; Nowak et al., 2004).
Compared to current practice, the PCT strategy was found to reduce the duration of total hospital stay with an average 2.9% (Christ-Crain et al., 2004; Kristoffersen et al., 2009; Schuetz et al., 2012; Stolz et al., 2007). Of this 2.9%, a reduction of 0.4 days (−10.8%) was attributable to the ICU stay (Stolz et al., 2007). Country-specific baseline data regarding the duration of hospital stay in current care were 6.0 days for the United Kingdom, 6.9 days for the Netherlands, and 12.0 days for Germany.
Furthermore, the literature review showed that of patients with COPD exacerbations, on average 6 · 3% are admitted to the ICU, and no significant difference herein between the PCT strategy and current practice was reported (Tokman et al., 2011). None of the three included studies that reported mortality rates (Christ-Crain et al., 2004; Schuetz et al., 2009, 2012) found a statistically significant difference between the PCT strategy versus current practice.
Cost-effectiveness
In all three countries, direct hospital costs and productivity losses are expected to decrease when a PCT-guided strategy is followed. Country-specific cost changes are shown in Tables 4–6.
The costs per patient with COPD exacerbations admitted to the hospital, split for each aspect of the treatment. Overall costs are shown per patient base and for the estimated yearly number of patients with COPD exacerbations admitted to the hospital in the Netherlands (n = 43,348). Numbers may not add up due to rounding.
The costs per patient with COPD exacerbations admitted to the hospital, split for each aspect of the treatment. Overall costs are shown on per patient base and for the estimated yearly number of patients with COPD exacerbations admitted to the hospital in Germany (n = 270,000). Numbers may not add up due to rounding.
The costs per patient with COPD exacerbations admitted to the hospital, split for each aspect of the treatment. Overall costs are shown on per patient base and for the estimated yearly number of patients with COPD exacerbations admitted to the hospital in the United Kingdom (n = 105,600). Numbers may not add up due to rounding.
The Netherlands
In the Netherlands, the PCT strategy leads to a reduction in expected total costs per patient from €6221 to €6078, indicating a decrease of €144 per patient (95% CI €−1290 to €1021). Combined with the reduction of 1.58 (95% CI: 0.06–3.17) in days that antibiotics are being administered (AB days), this leads to an incremental cost saving of €90 per AB day avoided. The reduction of 1.58 AB days ensures a reduction in the costs of antibiotic treatment, from €33 in current practice to €16 in the PCT strategy. Total laboratory costs increase with the PCT strategy from €184 to €253, which is due to the costs of PCT testing (€15 per test). Furthermore, the PCT strategy is expected to decrease productivity losses from €1817 to €1765, due to shorter total hospital stay.
Germany
In Germany, the total costs per patient are reduced from €8288 in current practice to €8091 with the PCT strategy, which is a reduction of €198 (95% CI: €−1805 to €1407) per patient. Cost savings are mainly attributable to a reduction in hospital costs of €154, from €4699 to €4545. Costs of antibiotic therapy are reduced from €24 in current practice to €12 in the PCT strategy. Laboratory costs increase with €58 (from €555 to €613). Productivity losses decreased with the PCT strategy because of shorter hospital stay, from €3010 to €2920. The cost reduction of €198 divided by the reduction of 1.58 (95% CI 0.08–3.14) in the number of antibiotic days gives an incremental cost saving of €125 per day on antibiotic therapy avoided per patient.
United Kingdom
In the United Kingdom, a total cost reduction of €81 (95% CI €−830 to €691) per patient is achieved by following the PCT strategy compared to current practice (from €4226 without PCT to €4144 with PCT). There is a reduction in the number of days on antibiotic therapy (−1.57, 95% CI: 0.05–3.12). Therefore, the incremental savings per day of antibiotic therapy avoided are €52 per patient. Cost savings are mainly attributable to the reduction in direct hospital costs (€100). Costs of laboratory tests increase in the PCT strategy compared to current practice, from €310 to €375. Productivity losses decrease in the PCT strategy due to the reduced duration of hospital stay, from €1003 to €972.
Decision uncertainty
The majority of random model draws from the predefined parameter distributions indicated that the PCT strategy is superior to current practice in each evaluated country, which means that it is expected to reduce the total per patient costs and the duration of antibiotic therapy. For the Netherlands, 58% (5835/10,000 simulations) of model draws fall in the south-east quadrant of the cost-effectiveness plot (see Supplementary Fig. S1); for Germany, this is 58% (5837 of 10,000; Supplementary Fig. S2); and for the United Kingdom, this is 57% (5730/10,000 simulations; Supplementary Fig. S3).
The CEACs (Figs. 2–4) show that at a willingness-to-pay threshold of €0 for 1 day of antibiotic treatment avoided, the probability of the PCT-guided strategy is ∼60% in all three countries. This probability reaches 80% at willingness to pay thresholds of €250 in the Netherlands (Fig. 2), €350 in Germany (Fig. 3), and €200 in the United Kingdom (Fig. 4). At a WTP threshold of €2000 per AB day avoided, the probability approaches 100%.
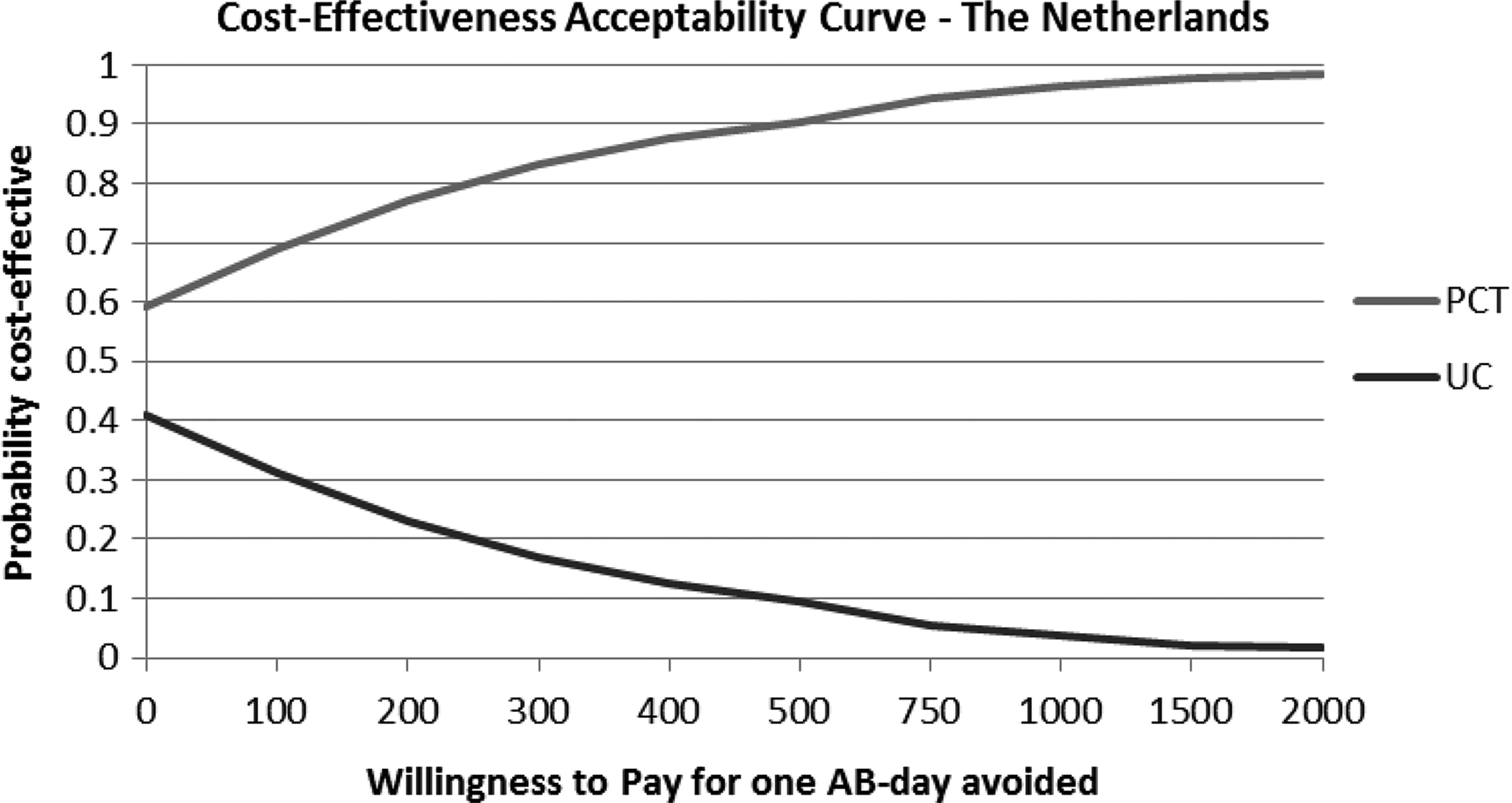
Cost-effectiveness acceptability curve for the Netherlands.
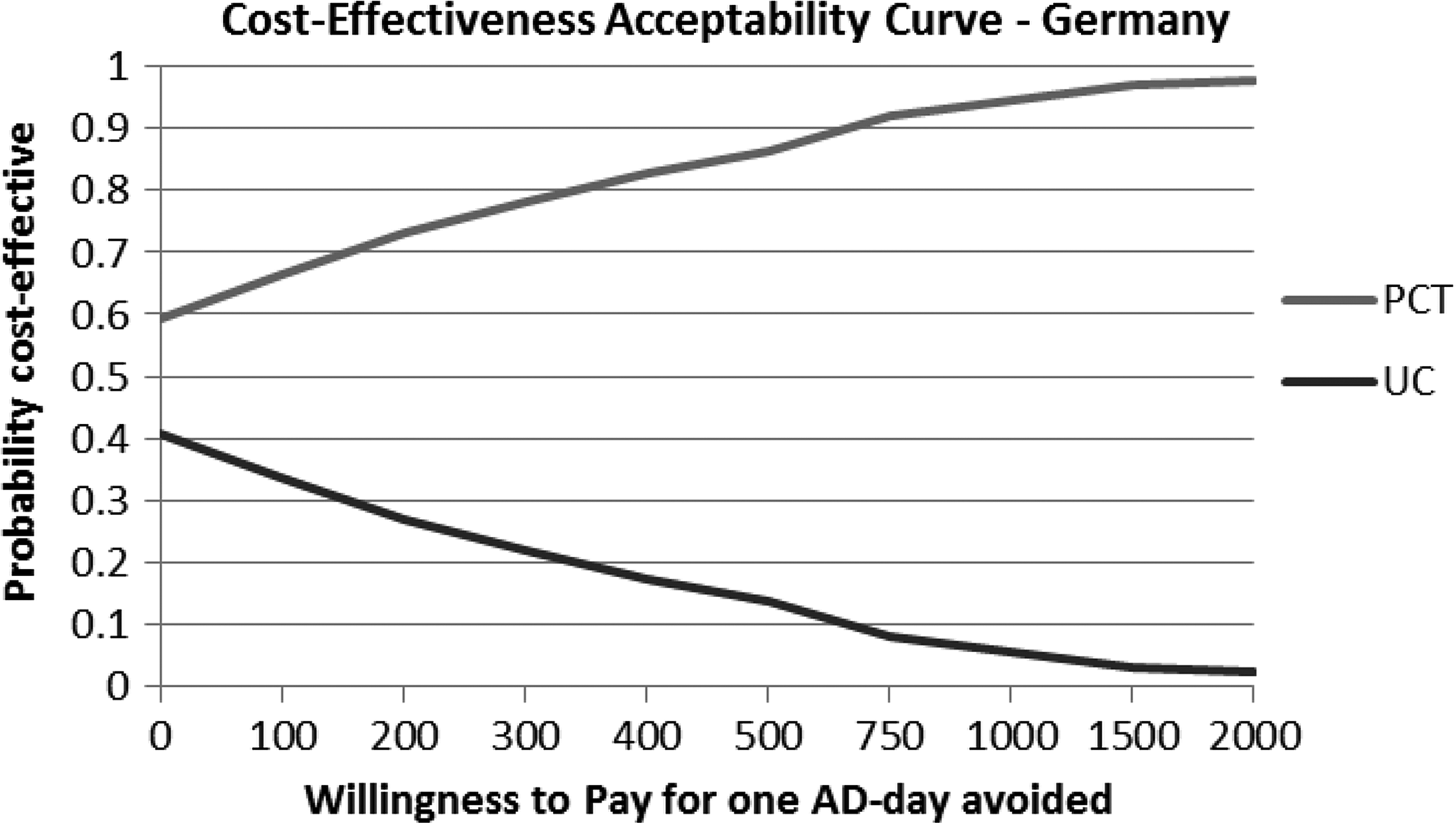
Cost-effectiveness acceptability curve for Germany.

Cost-effectiveness acceptability curve for the United Kingdom.
Sensitivity analysis
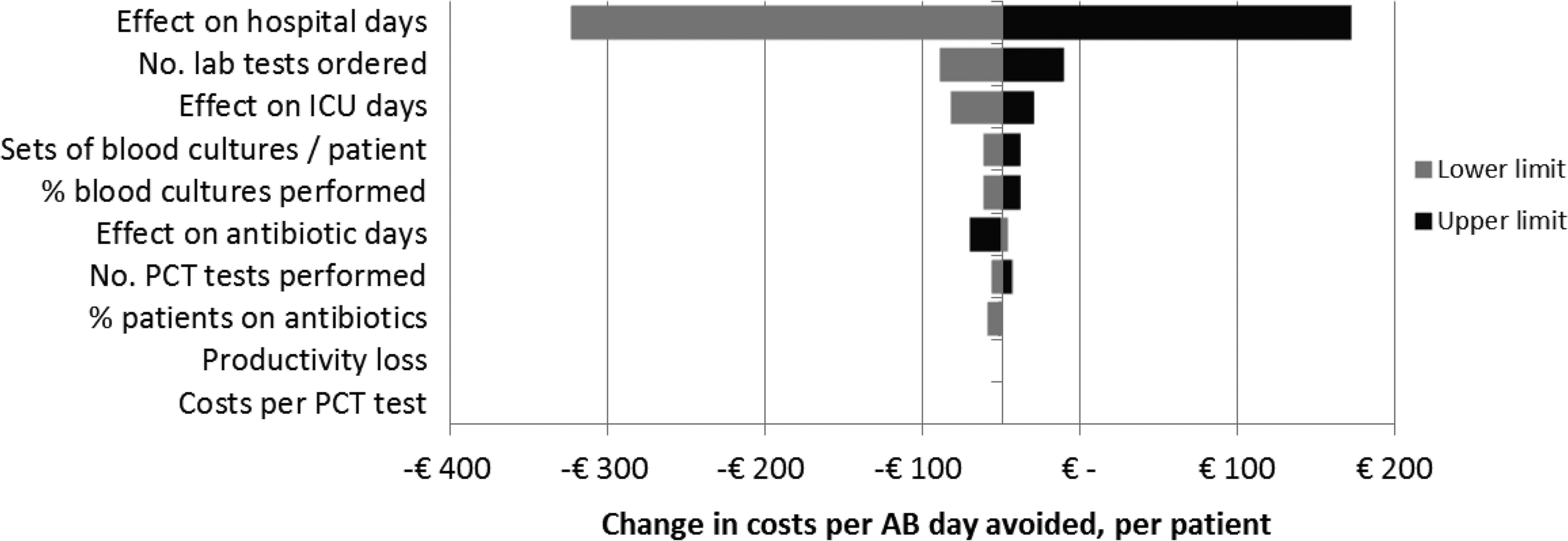
In all three countries, varying the number of general ward days over its prespecified range had the highest impact on incremental costs. When increased up to 25% from its baseline value, the PCT strategy became more costly than current practice, with incremental costs ranging from €48 (United Kingdom) to €59 (Germany) per patient. This translates to additional costs of €30, €37, and €38 per antibiotic day avoided in the United Kingdom, the Netherlands, and Germany, respectively. Furthermore, the number of ICU days had a relatively large impact on incremental costs in the Netherlands and the United Kingdom; the duration of antibiotic therapy affected the incremental costs in the Netherlands and Germany; and the number of laboratory tests ordered did so in Germany and the United Kingdom (Figs. 5–7).
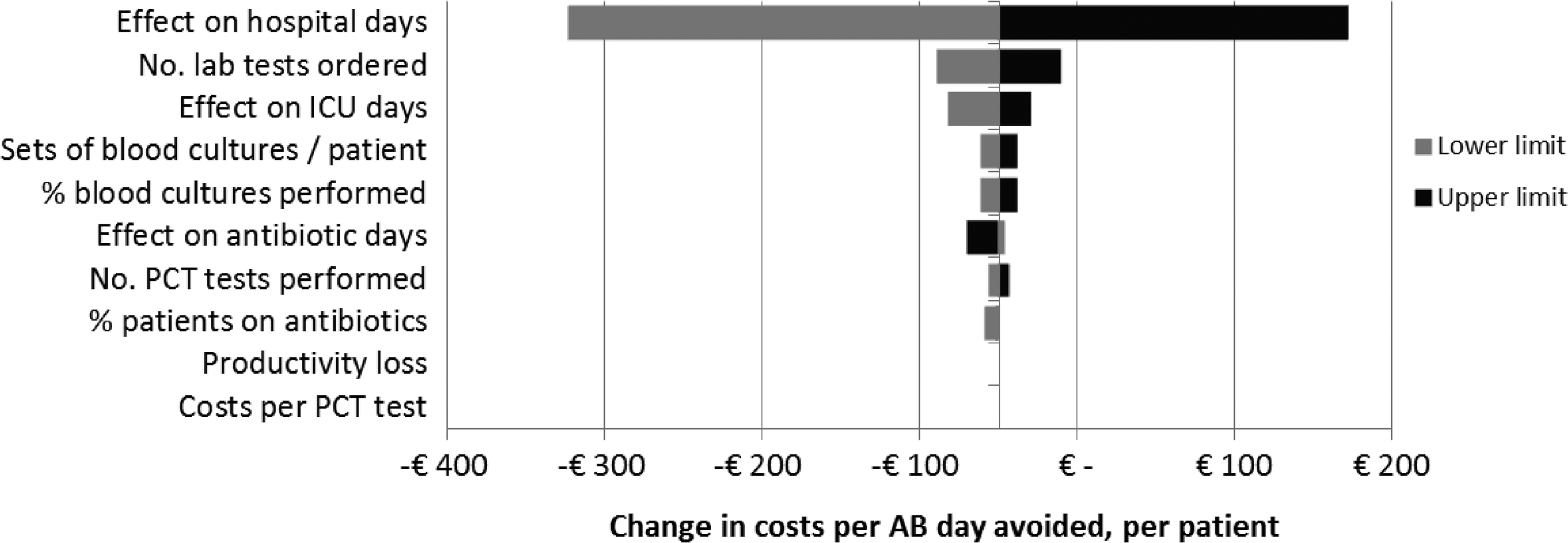
Tornado diagram, The Netherlands. Top 10 parameters influencing the incremental costs per AB day avoided. Tornado diagram showing the sensitivity of model outcomes to changes in parameter inputs. The lower and upper limits used in the sensitivity analysis for each parameter are shown in the gray boxes. The parameters derived from the systematic review (duration of ICU stay, regular ward stay, and antibiotic therapy) are varied with 1 SD below and above the mean. For parameters that showed an effect in the PCT strategy compared to current practice, the impact of changing this effect with ±50% is shown (percentage of patients in whom a blood culture is performed). All input parameters for which no effect was found due to the PCT strategy, a variation of 25% was used as lower and upper limit. ICU, intensive care unit; PCT, Procalcitonin.

Tornado diagram, Germany. Top 10 parameters influencing the incremental costs per AB day avoided. Tornado diagram showing the sensitivity of model outcomes to changes in parameter inputs. The lower and upper limits used in the sensitivity analysis for each parameter are shown in the gray boxes. The parameters derived from the systematic review (duration of ICU stay, regular ward stay, and antibiotic therapy) are varied with 1 SD below and above the mean. For parameters that show an effect in the PCT strategy compared to current practice, the impact of changing this effect with ±50% is shown (percentage of patients in whom a blood culture is performed). All input parameters for which no effect was found due to the PCT strategy, a variation of 25% was used as lower and upper limit.
Tornado diagram, the United Kingdom. Top 10 parameters influencing the incremental costs per AB day avoided. Tornado diagram showing the sensitivity of model outcomes to changes in parameter inputs. The lower and upper limits used in the sensitivity analysis for each parameter are shown in the grey boxes. The parameters derived from the systematic review (duration of ICU stay, regular ward stay, and antibiotic therapy) are varied with 1 SD below and above the mean. For parameters that show an effect in the PCT strategy compared to current practice, the impact of changing this effect with ±50% is shown (percentage of patients in whom a blood culture is performed). All input parameters for which no effect was found due to the PCT strategy, a variation of 25% was used as lower and upper limit.
None of the changes in these baseline parameter inputs indicated that the PCT strategy would become more costly than the current practice.
Discussion
The health and economic consequences of following a PCT algorithm to guide the prescription of antibiotics and the duration of antibiotic therapy are compared to current practice in this model-based study. Results of the analysis show that the costs of PCT testing would be more than recouped by reduced hospitalization costs (duration of hospital stay, mechanical ventilation, etc.) and reduced costs for antibiotic therapy. Besides this, both the percentage of patients in whom antibiotic therapy is initiated and the duration of antibiotic therapy are reduced in the PCT strategy. PCT testing is thus likely to be a cost-effective and cost-saving method for guiding antibiotic use in patients with COPD exacerbations in the Netherlands, Germany, and the United Kingdom.
PCT testing is expected to reduce the total societal costs per hospitalized patient with a COPD exacerbation of €144, €198, and €81 in the Netherlands, Germany, and the United Kingdom, respectively. Probabilistic sensitivity analyses show that, in all three countries, there is ∼60% probability that the PCT strategy is cost-effective at a willingness-to-pay of €0 and the majority of simulations indicate the PCT strategy to be superior (i.e., less costly and more effective) than current practice dominant.
The data found in the literature on the patient's duration of hospital stay and duration of ICU stay indicated trends to shorter length of stay in the PCT strategy. This effect, however, was not statistically significant. An additional analysis in which the length of stay in the ICU and the general ward for the PCT strategy were both set equal to current practice indicated that the PCT strategy would be more costly than current practice. Notably, when only ICU days in the PCT strategy were set equal to current practice (i.e., no reduction), the PCT strategy remained cost-effective (Figs. 5–7), and the ICERs indicate that the PCT strategy dominates current practice by being less costly and more effective.
The results of our study are in line with the results of the single other study that investigated the health economic consequences of PCT testing in ARIs (Schuetz et al., 2015). This study, performed from a US health system perspective, showed that a PCT strategy for patients with ARI was cost-effective for all ARI diagnoses and achieved without negatively affecting health outcomes (Schuetz et al., 2015).
Strength of this analysis is that all data are based on a systematic literature review, formally synthesizing all evidence to date. Furthermore, extensive sensitivity analyses are performed to deal with parameter uncertainty. These show that the expectation of the PCT strategy being cost-effective is highly robust against changes in input parameters, except when the reduction in hospital and ICU stay was assumed zero, in which case, the total costs are expected to increase slightly in the PCT strategy.
A limitation of the analysis is that for some input parameters (e.g., duration of antibiotic therapy), no country-specific data were available and the input values from the systematic literature search were used. In addition, we assumed that all hospital stay generates productivity loss. As not all patients may have paid work, this may overestimate the real-world productivity loss in each strategy to the same extent. Sensitivity analyses show the potential impact of this per country.
Conclusions and Key Findings in Context
The key study findings in context are presented in Table 7. Applying a PCT algorithm to guide initiation of antibiotic prescription and duration of antibiotic therapy is likely to be cost-effective compared to current practice for patients hospitalized with COPD exacerbations. Antibiotic prescription rate and duration of antibiotic therapy are reduced in the PCT strategy, generating sufficient cost-savings to compensate for upfront costs of performing PCT tests. Economic analysis based on real-life data is recommended for further research. Biomarker-driven prescription algorithms are important instruments for personalized medicine and rational therapeutics (Gokgoz and Akbulut, 2015; Mehla and Ramana, 2016). This also attests the emerging convergence of biomarker research and the broader field of Health Technology Assessment (HTA).
Footnotes
Acknowledgments
All authors met the ICMJE criteria for authorship. The authors have made substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data for the work; drafted the work or revised it critically for important intellectual content; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work. We gratefully acknowledge Ms. Annika Hanson for her editorial support and proofreading of the final article.
Author Disclosure Statement
PANAXEA b.v. received funding from BRAHMS GmbH, part of Thermo Fisher Scientific, Hennigsdorf, Germany, for developing and analyzing the model. The funding party had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication. The views expressed in this article are solely of the authors'.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.