
Abstract
Abstract
Approximately one in two patients with a chronic disease does not take their medicines as prescribed. Poor adherence is a worldwide epidemic and a major source of variability in pharmacokinetics (PK) and pharmacodynamics. Without addressing adherence, precision medicine is unlikely to come to fruition. In drug development, poor adherence confounds the estimates for efficacy and safety of drug candidates. Accurate and high-resolution measurement of adherence is a first step toward effective interventions against poor adherence. We describe a new cross-technology platform to measure adherence. The approach involves, first, building PK models to explain dose—exposure relationships. The model incorporates PK biomarkers by genotyping or phenotyping of drug metabolism, transport and other drug clearance pathways. Importantly, dose—exposure data for model building are obtained in healthy volunteer and/or patient cohorts who are ascertained for full adherence, using edible ingestion sensors (IS) that digitize orally administered medicines. Second, the built model is harnessed to back calculate the dose actually ingested by patients, given the empirically observed drug exposure, PK biomarker, demographic, and other patient data. The proposed platform is envisioned to result in development of both drug and drug-specific companion software for adherence measurement. In terms of feasibility, the new approach overlaps with current drug development timelines spanning the Phase 1 to 4 clinical trial continuum, and thus, could conceivably be implemented without requiring significant changes to the time sensitive clinical trial processes. For the IS-powered tools, the proposed platform creates a new space for applications in clinical trials to ensure adherence.
Drugs Don't Work in Patients Who Don't Take Them
For many patients, taking their medicines according to their health care provider's instructions is difficult. Approximately one in two patients with a chronic disease in developed countries does not take their medicines as prescribed (WHO, 2003). Adherence rates are even lower in developing countries. A worldwide epidemic in all therapeutic fields, poor adherence results in poor health outcomes, treatment failures, drug toxicity and resistance, and unpredictable pharmacokinetics (PK) and pharmacodynamics (PD). Poor medication adherence was estimated to result in $100 billion in the United States annually, by excess hospitalizations alone (Osterberg and Blaschke, 2005).
In drug development, poor adherence confounds the estimates for efficacy and safety of drug candidates (Breckenridge et al., 2017), and by extension, can bias the results of meta-analyses of data from clinical trials.
C. Everett Koop, a former U.S. Surgeon General, said in 1985 “drugs don't work in patients who don't take them.” Over the past decade, there has been marked growth in adherence research, while a new taxonomy for describing and defining adherence to medications was reported (Vrijens et al., 2012).
Measuring Adherence to Medicines
Accurate and high-resolution measurement of adherence is a first step toward effective interventions against poor adherence (Whalley Buono et al., 2017). Numerous approaches to quantify adherence have been reported with each method offering advantages as well as shortcomings (El Alili et al., 2016).
Measurement methods include, for example, the directly observed therapy (DOT) where patients take (swallow) each dose while a health care professional is watching, pill counts, prescription refill rates, and the medication event monitoring system that records opening of the cap on a medication container electronically.
Most recently, remote digital capture of dosing histories was reported, using coencapsulation of an ingestion sensor (IS) with an oral medication, and thus allowing digitized medicines and high-resolution measurement of adherence (Browne et al., 2018).
In this article, we describe a new idea and road map for the adherence measurement. We draw from the history of clinical pharmacology and suggest that two technological breakthroughs in particular, (1) mainstreaming of biomarkers in drug development over the past two decades (Biomarkers Definitions Working Group, 2001) and (2) the recent launch of IS to obtain digital dosing histories offer new opportunities for quantification of adherence.
In brief, early studies of drugs in humans and the field of clinical pharmacology in the 1960s reported the marked disconnect between drug dose and exposure in physiological compartments. Subsequent advances in drug metabolism and pharmacogenetics provided the early clues that person-to-person and between population variability in drug metabolism and other PK pathways account for the missing linkages that explain the dose–exposure relationships for medicines (Endrenyi et al., 1976; Kalow, 1965). The introduction of the concept (Biomarkers Definitions Working Group, 2001) and practice of biomarkers in drug development and clinical medicine presented an opportunity for differential diagnosis of patients who have unusually fast drug metabolism versus those who are nonadherent to their medication (Bertilsson et al., 1985).
Despite their relevance for adherence assessment, PK biomarkers were not systematically pursued with adherence research in focus, compared to the precision medicine, for example. In this context, a bottleneck was the inherent difficulty in establishing cohorts of patients who are ascertained, unequivocally, for full (100%) adherence to their medications. Indeed, even the meticulous DOT method for adherence can be “gamed” and fail. Patients whose adherence is quantified by DOT might appear to swallow a medicine but could hide and retain the drug in the oral cavity. But the recent breakthrough of IS and remote digital capture of ingestion events offer the possibility of not only high-resolution adherence measurement but also building cohorts of patients who are ascertained to be 100% adherent, with a view to adherence research across diverse technology platforms.
A New Cross-Technology Platform
Against the currently emerging digital transformation of adherence measurements with the IS technology, let us bring the advances in biomarkers and PK modeling into the picture as well. We propose that further innovation in adherence measurement is possible through new contexts for PK biomarkers and modeling as described here.
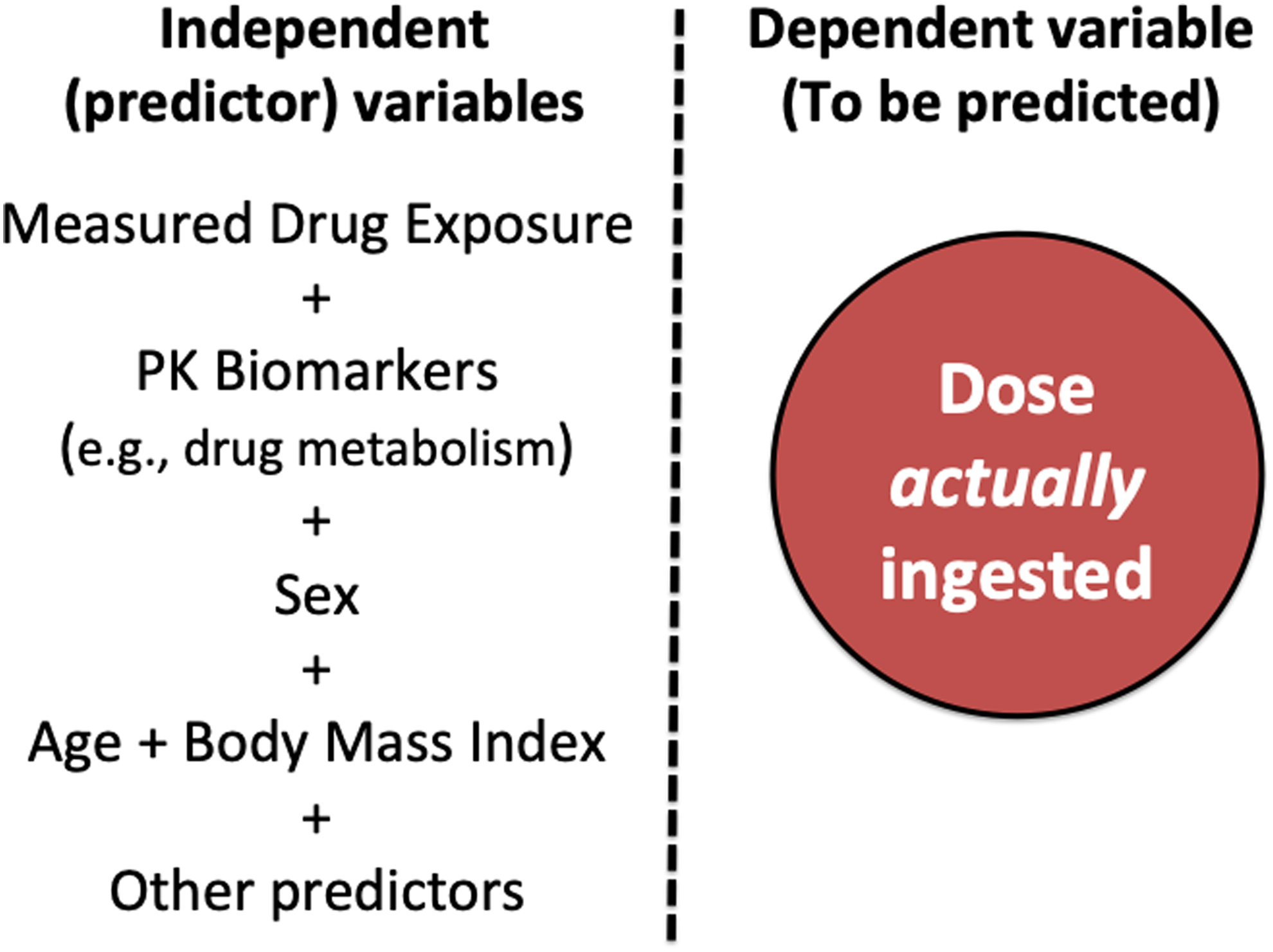
With availability over the past two decades of genetic and phenotypic biomarkers of drug metabolism in particular, and PK biomarkers more generally, it is currently possible to model dose–exposure relationships more precisely. For example, incorporation of drug metabolism biomarkers can significantly improve PK model fit and help explain a greater portion of variability in drug exposure (Linakis et al., 2018). Notably, the aims of clinical PK modeling have historically involved the forecasting of drug exposure in the organism (i.e., as dependent variable), using predictive covariates (i.e., as independent variables) such as biomarker data on PK pathways, age, sex, body mass index, and smoking history, among others (Fig. 1).

PK model building incorporating drug metabolism and other PK biomarkers in healthy volunteer or patient cohorts with full medication adherence. PK, pharmacokinetics.
We propose a three-step road map for innovation in adherence measurement as outlined in Figures 1–3.
Road map steps 1 and 2
We suggest that biomarker-guided clinical PK models be developed (Fig. 1) so as to enhance the predictive performance of such models in explaining dose–exposure relationships. Once this first step in PK model building is completed, dependent and independent variables can be switched to back calculate the dose actually ingested. In this case, the estimation of the dose actually ingested by the patient becomes the dependent (to be predicted) variable, while the empirically observed clinical data on drug exposure in the blood, PK biomarkers, age, sex, and other covariates serve as independent (predictive covariate) variables (Fig. 2).
The use of biomarker incorporated PK model for back calculation of the dose actually ingested by patients.
We emphasize that our proposed road map crucially requires, in step 1, recruitment of healthy volunteers or patients who are ascertained unequivocally for full adherence to the drug of interest, for example, using the IS-powered high-resolution digitized medication ingestion records or other high-resolution technologies that may be available in the future (Fig. 3).

A three-step road map for innovation in adherence measurement.
In addition, for step 2 of the road map, PK biomarkers are not intended to predict drug exposure in the blood but for adherence measurement (i.e., estimation of the dose actually ingested by the patient, given the observed drug exposure in the blood and other covariates) as illustrated in Figure 2.
Road map step 3
In terms of feasibility, step 1 model building in adherence ascertained cohorts can usefully map on to Phase 1 and 2 drug development timelines, whereas the back calculation of adherence can map on to Phase 3 and 4 drug development (Fig. 3). A corollary of our proposal is that the new approach would result in two companion products in the clinic, (1) the drug itself and (2) a software that can estimate the actual drug dose ingested by patients, and thus the extent to which a given person is adherent (Fig. 3).
Outlook on Adherence Innovation
Poor adherence to medicines is a worldwide public health burden and a major source of variability in PK and PD. Without addressing adherence as a first step in rational therapeutics, precision medicine efforts are unlikely to come to fruition. It is therefore worth to reemphasize the quote “Drugs don't work in patients who don't take them” by C. Everett Koop. Moreover, precision adherence is relevant not only for drugs but also for all orally administered medicinal products.
IS-powered digital medicines are promising for the future of clinical pharmacology and rational therapeutics. Yet, there is still a need for a diversity approaches to adherence measurement for patients who might require or find acceptable each approach to various degrees. Digital medicines and IS would require mapping of the broader societal corollaries of digital data on adherence for responsible innovation (Özdemir, 2019). For example, “the physical and virtual worlds markedly differ in speed, scale, and temporalities, as do our physical self and digital footprints. Digital data are highly fluid and can rapidly move across spaces and places, whereas the physical data and humans are much slower and exist in different scales than our digital footprints” (Özdemir, 2019). The burgeoning field of responsible innovation (Frodeman, 2019; Von Schomberg and Hankins, 2019) can usefully inform and help address the societal impacts and development of IS- and biomarker-powered tools for adherence measurement on the proposed cross-technology platform.
Looking into the future, for the IS powered adherence measurement approaches, the cross-technology platform proposed here could create new applications of IS in drug development (i.e., not only in clinical practice) (Fig. 3). Addressing adherence measurement using sensors and biomarkers would bode well for precision medicine as well: the data on biomarkers can be used for both adherence measurement and dose individualization in the same patient and for drugs that share the same biomarker pathways.
Finally, the proposed road map in Figure 3 naturally aligns with existing drug development timelines spanning the Phase 1 to Phase 4 clinical trial continuum, and thus, could conceivably be implemented without requiring significant changes to the time sensitive clinical trial processes.
Ensuring adherence to medicines is of interest to physicians, patients who stand the most to benefit from drugs taken as prescribed, public health practitioners, the medicinal product industry, and scholars in the field of responsible research and innovation. The prospect of further adherence innovation is worth considering by uniquely integrating biomarkers, IS, and digitized medicines as outlined in this article.
Disclaimer
The views expressed reflect the personal opinions of the authors only.
Footnotes
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.