
Abstract

A
Where do the placebo effects come from if the placebo itself does not have pharmacological activity?
Drug treatment is embedded in a broader nonpharmacological context, shown in Figure 1. The social, cultural, and material contexts of drug administration, a subject matter for the discipline of social pharmacology that is unfortunately still underrepresented or missing in 21st century medicine, matter greatly for placebo studies. The nonpharmacological context of health interventions elicits expectations, classical conditioning, and associative learning effects on the part of patients, and, by extension, alters neurobiology and organ function, for example, blood pressure, heart rate, anxiety, and mood, among other clinical endpoints. Although placebos cannot cure a serous illness such as cancer, all drugs and health interventions have placebo effects that contribute to their overall effects (Fig. 2).

Nonpharmacological contexts of therapeutic encounters produce placebo and nocebo effects that affect drug efficacy and side effects, respectively (Modified from Özdemir and Endrenyi, 2021).
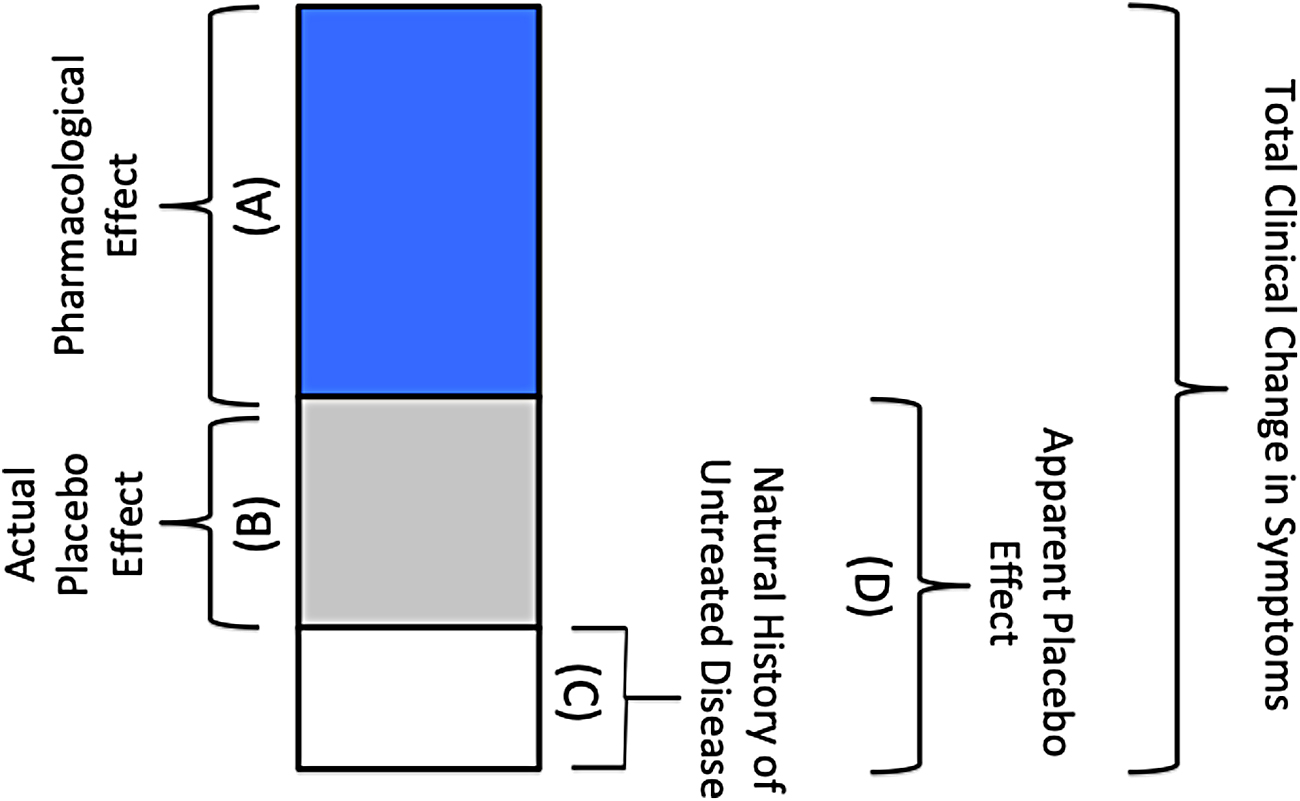
A taxonomy of changes in patients' clinical symptoms by a therapeutic encounter such as drug treatment: (A) the pharmacological effect, produced by a drug's chemical effects on efficacy-related molecular targets, (B) the actual placebo effect, (C) the natural history of untreated disease, regression to the mean and spontaneous remission of symptoms, (D) apparent placebo effect that includes the actual placebo effect and the natural history of untreated disease, for example, in a clinical trial that employs a chemically inert placebo, without a “no treatment” control group. Note that the relationship between pharmacological and placebo effects is not always additive in nature, and may potentially involve complex nonadditive interactions (Modified from Özdemir and Endrenyi, 2021).
Placebo effects are clinically appreciable. From the years 1991 to 2015, the average proportion of placebo responders was reportedly 35% to 40% in antidepressant clinical trials in adults with major depression (Furukawa et al., 2016). The size of the placebo effect varies depending on the disease, symptoms, clinical trial design, and patients' genomic variation, among other factors. In addition, placebo effects are observed in studies beyond psychiatry and psychology, including pain management, allergies, immunology, and sleep and gastrointestinal disorders (Schedlowski et al., 2015).
The etymology of placebo has been noted as being from the Latin “I shall please” and placere (to please). In contrast, others (Cai and He, 2019; Lasagna, 1986) have emphasized that the original meaning of the word was “to walk,” instead of “to please.” In a medical context, the use of placebo was noted in the 18th century (Jütte, 2013; Kerr et al., 2008).
Nocebo Effects
Nocebo effects are the opposite of placebo effects, observed in therapeutic encounters accompanied by adversarial contexts that elicit negative expectations such as poor physician and patient communication or a negative clinical setting. Research has shown that nocebo effects are common. For example, in the case of patients who discontinued statin drug therapy due to side effects, a study has shown that 90% of the symptom burden was attributed to nocebo effects (Wood et al., 2020). A meta-analysis of 3544 placebo-treated patients in randomized controlled trials in Parkinson's disease found that 8.8% (95% confidence interval: 6.8–11.5) discontinued placebo treatment due to “intolerance” (Stathis et al., 2013).
A New Challenge for Biomarker Development
Placebogenomics and nocebogenomics
Genomic variation influences health intervention outcomes at multiple levels, including the placebo and nocebo variability (Fig. 3). Placebogenomics and nocebogenomics have been defined as the multiomic studies of interindividual and intraindividual variability in placebo and nocebo phenotypes, respectively (Özdemir and Endrenyi, 2021). It is anticipated that placebogenomic and nocebogenomic biomarkers of placebo and nocebo variability will become available in the coming decade.
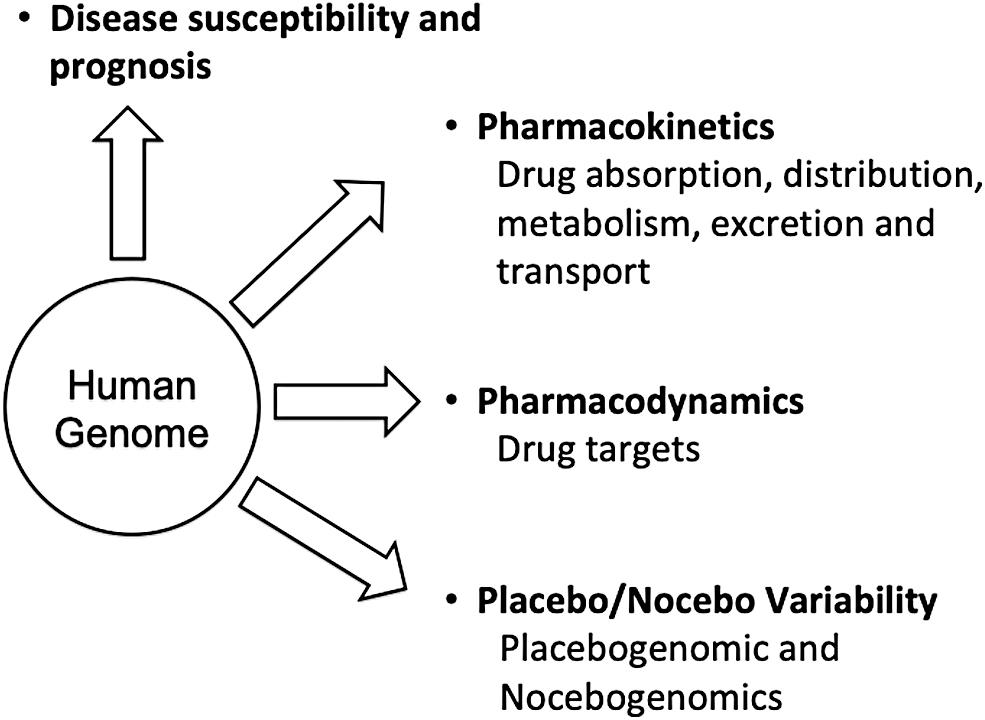
Genomic, epigenomic, and multiomics variations, among patients and populations, can influence (1) disease susceptibility and prognosis, (2) drug pharmacokinetics, (3) drug efficacy targets, and (4) placebo/nocebo effects (Modified from Özdemir and Endrenyi, 2021).
Placebogenomics and nocebogenomics also present new challenges and prospects for biomarker development in the field of personalized medicine. For example, pharmacogenomics, nutrigenomics, and vaccinomics are subfields of personalized medicine. They aim to individually tailor, respectively, drug, nutritional, and vaccine therapeutics based on variations in genome and environmental exposures. The clinical association study design where genomic and phenotypic variations in treatment outcomes are correlated has been a cornerstone of these personalized medicine subfields.
New insights from the field of placebo studies suggest that the biological pathways involved in variable drug and placebo responses might overlap (Özdemir and Endrenyi, 2021). Levine et al. (1978) provided evidence for the involvement of endogenously released opioids by showing that placebo-induced analgesia can be antagonized by naloxone. A positron emission tomography study showed that both opioid and placebo analgesia are associated with increased activity in the rostral anterior cingulate cortex, suggesting related neural mechanisms in placebo and drug action (Petrovic et al., 2002).
Dopamine, opioid, cannabinoid, and serotonin pathways are prominent candidates for genetic studies of placebo and nocebo phenotypes (Hall et al., 2015, 2018; Özdemir and Endrenyi, 2021). Importantly, these pathways are also well-established molecular drug targets. The candidate gene approach to study placebo variability has been recently scaled up with network/pathway analyses. Wang et al. (2017) reported that the “molecular pathways affected by certain drug classes indicate the existence of placebo–drug interactions” (Wang et al., 2017). Taken together, these new findings raise the possibility of placebo–gene–drug interactions (Özdemir and Endrenyi, 2021).
For example, pharmacogenomic association studies of drug responders/nonresponders may want to consider analyses of not only drug-treated but also placebo-treated control subjects. This would allow ascertainment of whether the identified pharmacogenomics association findings reflect a genuine biomarker for pharmacological or placebo variability, or both. Moreover, the apparent placebo effect (Fig. 3) as a phenotype of interest is not ideal for it includes the natural history of disease and, therefore, does not reflect the true extent of placebo variability. A no treatment control group would be necessary, and yet is not always feasible due to ethical concerns.
Outlook
Because all drugs and health interventions have embedded placebo components, candidate genomic biomarkers of variability in drug, nutrition, or vaccine-related outcomes would be more robust if they were evaluated further in placebo-treated groups, while bearing in mind the caveats already noted. This shall ensure that a biomarker candidate is drug response related, instead of a placebo response. It is also noteworthy that placebo studies have so far been neglected in personalized medicine. Yet, placebogenomics and nocebogenomics are poised to advance personalized medicine scholarship so that the biomarker discoveries stand the tests of time, sociocultural context, and placebo/nocebo effects (Brand et al., 2021).
Footnotes
Disclaimer
The views expressed are the personal opinions of the author only.
Author Disclosure Statement
The author declares there are no conflicting financial interests.
Funding Information
No funding was received for this article.